
Arthroscopic fixation of acute reverse bony Bankart lesions using cannulated cancellous screws is a minimally invasive, effective technique that restores glenoid articular congruity and provides stable fixation, especially in moderate-sized posterior glenoid bone defects.
Dr. Rahul Kakran, Department of Orthopaedics, Yashoda Group of Hospitals, Ghaziabad, Uttar Pradesh, India. E-mail: rahul.kakran@yahoo.com
Abstract
Introduction: Reverse bony Bankart lesions are a rare cause of posterior shoulder instability following traumatic dislocation. Optimal management remains controversial, especially in cases with significant glenoid bone loss. Arthroscopic fixation offers a minimally invasive alternative to open procedures.
Case Report: A 50-year-old male presented with pain and instability of the right shoulder following a road traffic accident. Imaging revealed an acute reverse bony Bankart lesion involving approximately 38% of the glenoid surface. The patient was managed with arthroscopic reduction and internal fixation using cannulated cancellous screws. Post-operative rehabilitation was initiated early, with gradual restoration of range of motion and strengthening.
Conclusion: Arthroscopic fixation of reverse bony Bankart lesions is a safe and effective technique in acute cases with moderate bone loss, providing stable fixation, restoration of joint congruity, and good functional outcomes while avoiding the morbidity of open surgery.
Keywords: Reverse bony Bankart, posterior shoulder instability, arthroscopic fixation, glenoid fracture, case report.
Bone defects of the glenoid and humeral head can result in instability and recurrent dislocation because they alter the natural congruency and disrupt the inherent static stabilizers of the glenohumeral joint [1].
In contrast to anterior instability, posterior instability is uncommon, accounting for only 2–12% of all the patients with glenohumeral instability [2,3]. The mechanism resulting in a posterior bony Bankart lesion is usually a traumatic event resulting in posterior translation of the humeral head with the arm positioned in flexion and adduction. This has been well documented in athletes, especially football players and weightlifters, in addition to patients with seizures and those sustaining electric shock [4,5]. Traumatic posterior shoulder dislocations can lead to impression fractures on the anterior surface of the humeral head, known as “reverse Hill–Sachs lesions.”
Depending on the size of the defect, the reverse Hill–Sachs lesion can engage on the posterior glenoid rim with internal rotation, leading to subluxation or recurrent dislocation events. The most common complication after posterior dislocation is recurrent instability, with a 17.7% recurrence rate within the 1st year after dislocation. The risk is highest in patients who are aged <40 years, sustain the dislocation during a seizure, and have a large reverse Hill–Sachs lesion (>1.5 cm3) [5].
There exists a general consensus that glenoid bone loss with recurrent instability should be treated by restoring the articular surface anatomy. The technique used to treat reverse bony Bankart lesions, as well as determining when to add a reverse remplissage procedure, remains controversial, however.
Methods including posterior iliac crest glenoid bone block, open repair with internal fixation, and arthroscopic labral repair have shown variable outcomes in the literature, and an algorithm based on the degree of bone loss is less concise than anterior glenoid bone loss [1,6,7,8].
The purpose of this article is to describe our technique of restoring the glenoid articular surface by repairing a posterior bony Bankart lesion. This allarthroscopic procedure avoids the morbidity of an open technique and allows one to address the posterior bone loss or capsulolabral pathology.
A 50-year-old man sustained a right shoulder fracture dislocation (reduced spontaneously by the patient on his own) following a road traffic accident. Radiograph showed a bony fragment (Fig. 1) and computed tomography (CT) revealed a reverse bony Bankart lesion at the postero-inferior part of the glenoid articular surface from 6’o clock to 10’o clock with Hill Sachs lesion (Fig. 2).
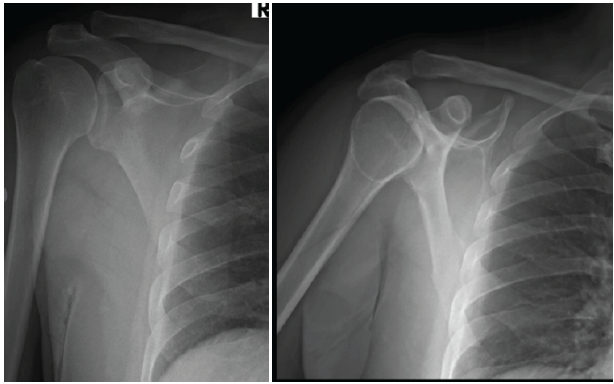
Figure 1: Pre-operative X-rays of the shoulder showing a glenoid fracture.
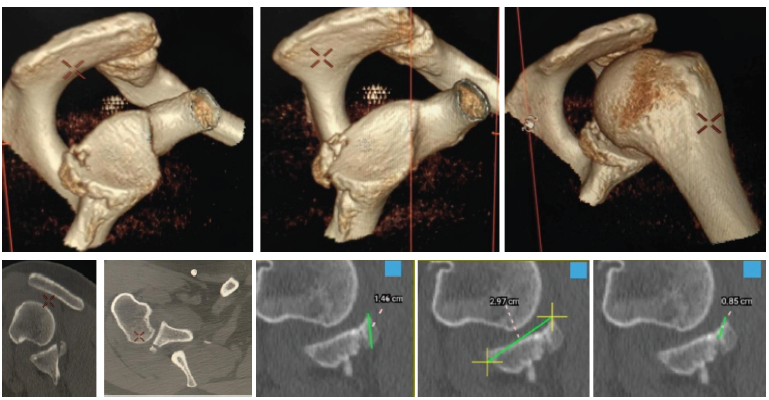
Figure 2: Pre-operative non-contrast computed tomography scan of the shoulder showing reverse bony Bankart lesion at the postero-inferior part of the glenoid articular surface 6 o’clock to 10 o’clock, with Hill–Sachs lesion.
The size of the bony fragment was 38% of the glenoid surface area on the 3dimensional CT (Fig. 2). MRI scan of shoulder revealed a reverse bony Bankart lesion at the posteroinferior part of the glenoid articular surface from 6’o clock to 10’o clock with Hill–Sachs lesion (Fig. 3) and therefore, we decided to fix the fracture by arthroscopic reduction and internal fixation of the reverse bony Bankart lesion.
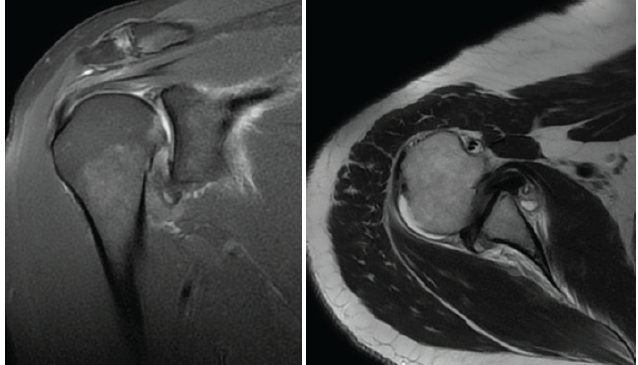
Figure 3: Pre-operative magnetic resonance imaging scan of the shoulder showing reverse bony Bankart lesion at the postero-inferior part of the glenoid articular surface with Hill–Sachs lesion, surgical technique.
Surgical technique
The procedure was performed under general anesthesia with the patient positioned in the lateral decubitus position and the affected limb placed under traction to allow optimal visualization of the glenohumeral joint. After standard sterile preparation and draping, a posterior portal was established for diagnostic arthroscopy, followed by creation of an anterosuperior portal and an accessory posterolateral portal under direct visualization.
Initial diagnostic arthroscopy confirmed the presence of a reverse bony Bankart lesion involving the posteroinferior glenoid rim (Fig. 4). Hematoma, debris, and fibrous tissue were debrided using a motorized shaver to clearly delineate the fracture fragment and glenoid bed. Care was taken to preserve the capsulolabral attachments to maintain vascularity. The fracture bed was gently freshened to promote healing (Fig. 5).
Figure 4: Diagnostic arthroscopy showing presence of reverse bony bankart lesion involving posteroinferior glenoid rim.
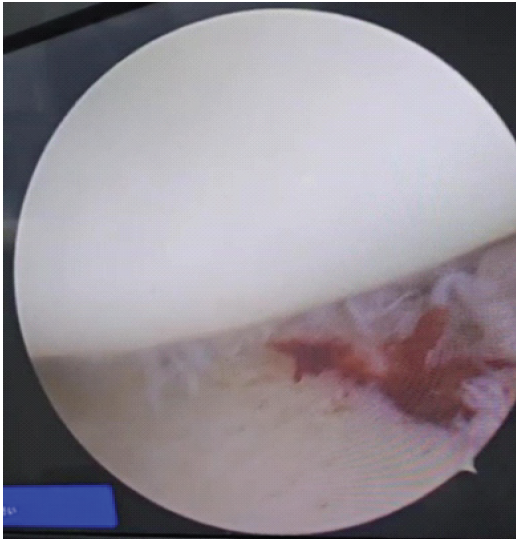
Figure 5: Arthroscopic image showing freshening of the glenoid fracture bed and bleeding bony ends to promote healing.
The bony fragment was carefully mobilized using a probe and periosteal elevator to restore its anatomical position. Adequate mobilization was ensured to achieve anatomic reduction without tension. Reduction was achieved under direct arthroscopic visualization and temporarily maintained with a probe (Fig. 6).
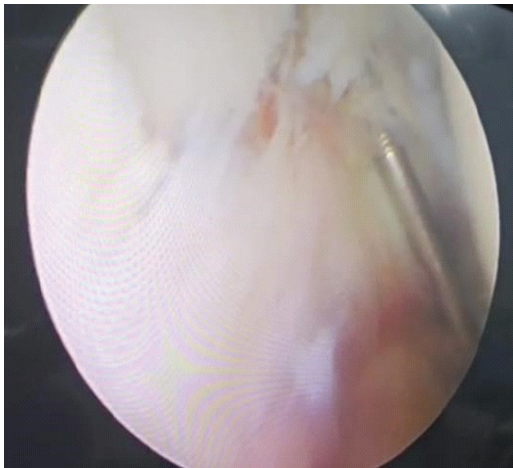
Figure 6: Arthroscopic image showing fracture fragment mobilization and temporary fixation using guide wire.
A guidewire for cannulated fixation was then introduced percutaneously through the posterolateral portal, ensuring a trajectory perpendicular to the fracture plane (Fig. 7).
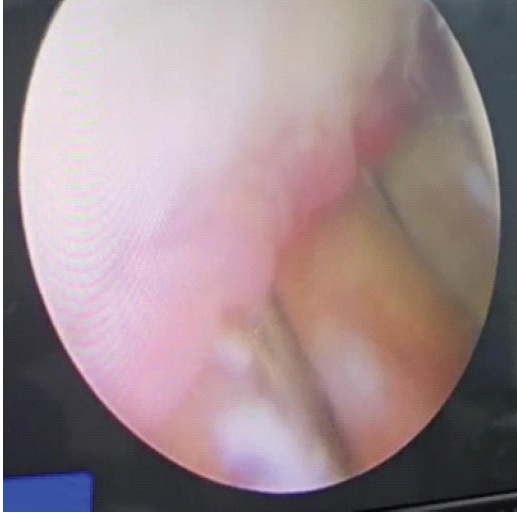
Figure 7: Arthroscopic image showing guide wire placement through the posterolateral portal.
Proper positioning of the guidewire was confirmed arthroscopically. Overdrilling was subsequently performed, and an appropriately sized cannulated cancellous screw was inserted over the guidewire to achieve compression and stable fixation of the fragment (Fig. 8). The screw head was carefully countersunk beneath the articular surface to prevent intra-articular prominence (Fig. 9).

Figure 8: Clinical image showing measurement of screw size.
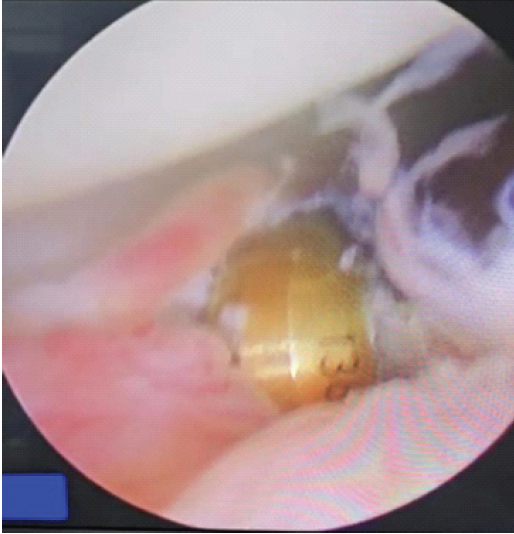
Figure 9: Arthroscopic image showing final screw placement.
Following fixation, the stability of the construct and restoration of the glenoid articular congruity were confirmed arthroscopically. The shoulder was gently taken through a range of motion to ensure the absence of hardware impingement and maintenance of reduction. Final inspection of the joint was performed before closure (Fig. 10).
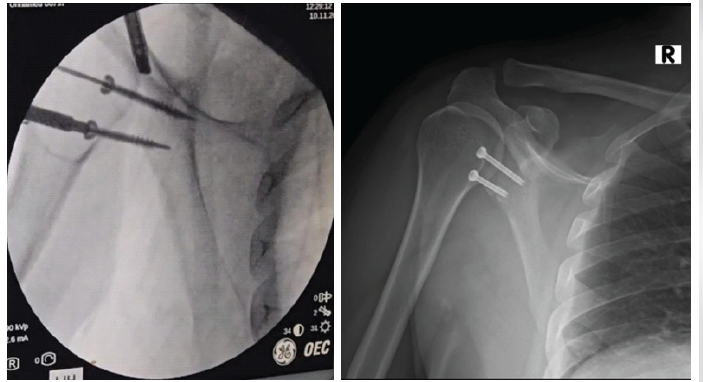
Figure 10: C arm image showing final stable fixation and Immediate post-operative X rays.
All portals were closed in layers, and a sterile dressing was applied. The limb was immobilized in a sling postoperatively, and a structured rehabilitation protocol was initiated. Immediate post-operative X rays showed stable fixation and satisfactory alignment (Fig. 10).
Tips and pearls
- Adequate mobilization of the fragment is essential for anatomical reduction
- Maintain soft tissue attachments to preserve the blood supply
- Use a pre-operative CT scan (3D reconstruction) to plan the screw trajectory
- Ensure perpendicular screw placement for optimal compression
- Always countersink the screw head to prevent articular damage
- Early arthroscopic visualization allows precise reduction compared to open methods
Pitfalls
- Inadequate mobilization may lead to malreduction
- Incorrect screw trajectory can result in poor fixation or joint penetration
- Prominent hardware may cause cartilage damage or impingement
- This technique may not be suitable for large or chronic lesions with significant bone loss
- Failure to recognize associated injuries (e.g., reverse Hill–Sachs lesion) may lead to persistent instability.
Post-operative protocol and follow-up
- For the immediate post-operative period, the patient was started on shoulder shrugs, scapular retraction, elbow, and wrist range of motion exercises, along with isometric shoulder strengthening exercises.
- After 2 weeks, passive range of motion was started till forward elevation of 90° and external rotation with the elbow at the side to 30°. Sling was discontinued at 4 weeks, after which active-assisted and active range of motion exercises were started. Shoulder abduction and external rotation were avoided for 6 weeks.
- Radiographs obtained 3 months showed maintained alignment and appropriate positioning of fixation and reconstruction hardware with no evidence of implant failure or loss of reduction (Fig. 11).
- After 6 weeks, active external rotation to 45° and abduction to 90° was initiated. At week 12, a full active range of motion was allowed, and strengthening started (Fig. 12).
- Return to sports was initiated at 6 months after regaining sufficient strength, as determined by the physiotherapist and clinician.
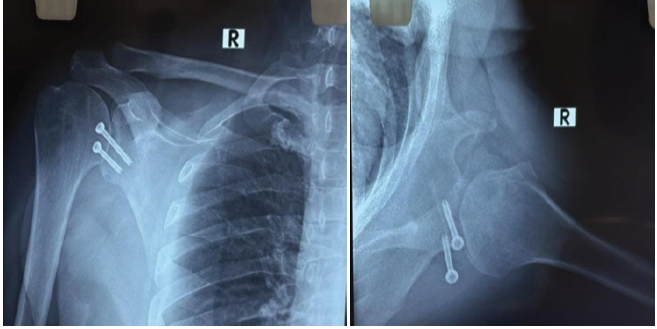
Figure 11: Three-month post-operative X-rays.

Figure 12: Three-month post-operative clinical images showing the full range of movement of the right shoulder.
- To date, there has been a paucity of literature accurately establishing which posterior bone defects should be managed with bony procedures, as well as the correlation between posterior bone loss and risk of redislocation. Algorithms on anterior bone loss have been reported in the literature, however. These algorithms take into account the degree of bone loss; location of defects; associated reverse Hill–Sachs lesions; and patient age, activities, and medical factors such as unstable epilepsy [1].
- DeLong et al. [9] reported in their systematic review on posterior shoulder instability that stabilization with anchors results in fewer recurrences and revisions than anchorless repairs in young adults engaging in highly demanding physical activity. Furthermore, the literature has suggested that patients with posterior labral tears treated arthroscopically have good outcomes with respect to stability, recurrence of instability, patient satisfaction, return to sport, and return to the previous level of play.
- A double-horizontal mattress configuration also reduces strangulation of the tissue and possible tissue necrosis, as described by DeLong et al. [9] and Koo et al. [10]. Using the subscapularis to fill the reverse Hill–Sachs lesion effectively externalizes the lesion and prevents engagement on the posterior–inferior glenoid with internal rotation of the arm.
- Carefully scrutinizing advanced imaging, such as CT and/or magnetic resonance imaging, provides better visualization of bone loss and more accurate estimation of the degree of bone loss. This is particularly important for bone loss >20%, in which posterior bone block procedures may be required for stability. Limitations exist regarding our technique.
- First, it is only reliable for smaller posterior bony Bankart lesions. In lesions with a larger degree of bone loss, the technique may not provide adequate stability, thus necessitating other bony procedures.
- Second, our case demonstrates an acute injury. Chronic lesions are more difficult to mobilize and may be healed in a medial position, requiring extensive mobilization.
- Finally, we suggest explaining to the patient that an open procedure may be required if the reverse Hill–Sachs lesion or posterior bone loss is greater than expected. In conclusion, our technique offers concise arthroscopic management of a posterior bony Bankart lesion and moderate-sized reverse Hill–Sachs lesion and provides immediate stability for an acute posterior dislocation of the shoulder.
- To the best of our knowledge, this specific combination of injury pattern and its single-stage arthroscopic management has never been documented in the world literature.
Arthroscopic fixation of reverse bony Bankart lesions is a safe and effective technique for managing acute posterior shoulder instability with moderate glenoid bone loss. It provides anatomical restoration, stable fixation, and favorable functional outcomes while minimizing surgical morbidity. Careful patient selection and pre-operative assessment of bone loss are essential for optimal results
In patients with acute posterior shoulder instability and reverse bony Bankart lesions, arthroscopic fixation should be considered as a first-line treatment for moderate-sized defects, as it offers stable fixation, early rehabilitation, and avoids complications associated with open procedures.
References
- 1. Longo UG, Rizzello G, Locher J, Salvatore G, Florio P, Maffulli N, et al. Bone loss in patients with posterior gleno-humeral instability: A systematic review. Knee Surg Sports Traumatol Arthrosc 2016;24:612-7. [Google Scholar] [PubMed]
- 2. Maffulli N, Longo UG, Gougoulias N, Caine D, Denaro V. Sport injuries: A review of outcomes. Br Med Bull 2011;97:47-80. [Google Scholar] [PubMed]
- 3. Maffulli N, Longo UG, Spiezia F, Denaro V. Aetiology and prevention of injuries in elite young athletes. Med Sport Sci 2011;56:187-200. [Google Scholar] [PubMed]
- 4. Buhler M, Gerber C. Shoulder instability related to epileptic seizures. J Shoulder Elbow Surg 2002;11:339-44. [Google Scholar] [PubMed]
- 5. Robinson CM, Seah M, Akhtar MA. The epidemiology, risk of recurrence, and functional outcome after an acute traumatic posterior dislocation of the shoulder. J Bone Joint Surg Am 2011;93:1605-13. [Google Scholar] [PubMed]
- 6. Smith T, Goede F, Struck M, Wellmann M. Arthroscopic posterior shoulder stabilization with an iliac bone graft and capsular repair: A novel technique. Arthrosc Tech 2012;1:e181-5. [Google Scholar] [PubMed]
- 7. Bradley JP, McClincy MP, Arner JW, Tejwani SG. Arthroscopic capsulolabral reconstruction for posterior instability of the shoulder: A prospective study of 200 shoulders. Am J Sports Med 2013;41:2005-14. [Google Scholar] [PubMed]
- 8. Williams RJ 3rd, Strickland S, Cohen M, Altchek DW, Warren RF. Arthroscopic repair for traumatic posterior shoulder instability. Am J Sports Med 2003;31:203-9. [Google Scholar] [PubMed]
- 9. DeLong JM, Jiang K, Bradley JP. Posterior instability of the shoulder: A systematic review and meta-analysis of clinical outcomes. Am J Sports Med 2015;43:1805-17. [Google Scholar] [PubMed]
- 10. Koo SS, Burkhart SS, Ochoa E. Arthroscopic double-pulley remplissage technique for engaging hill-sachs lesions in anterior shoulder instability repairs. Arthroscopy 2009;25:1343-8. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report
July 1, 2026 Extradigital Glomus Tumor of the Knee Mimicking Osteoarthritis: A Case Report July 1, 2026 Shoulder Injuries Secondary to Proning: Sequelae of Long COVID Syndrome: A Case Report
July 1, 2026 Shoulder Injuries Secondary to Proning: Sequelae of Long COVID Syndrome: A Case Report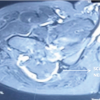 July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report
July 1, 2026 Large Posterior Proximal Femur Osteochondroma Presenting in Adulthood – Diagnostic Challenges and Management Strategy: A Case Report July 1, 2026 Varied Reduction and Fixation Modalities for Scapula Fractures: A Case Series
July 1, 2026 Varied Reduction and Fixation Modalities for Scapula Fractures: A Case Series