
Limb-salvage reconstruction in concordant bilateral fibular hemimelia with tetramelic ectrodactyly can achieve limb preservation but carries significant staged-complication risk, requiring meticulous planning, multidisciplinary follow-up, and early counseling about salvage versus amputation.
Dr. Mark A Bachir, California Northstate University, College of Medicine, Elk Grove, California, United States. E-mail: mark.bachir6420@cnsu.edu
Abstract
Introduction: Fibular hemimelia (FH) is a rare congenital limb deficiency that presents with ankle instability, limb length discrepancy, and valgus malalignment, which can coexist with additional limb malformations that can, in turn complicate reconstruction and long-term function.
Case Report: We report a 19-year-old male with congenital bilateral FH, as well as tetramelic ectrodactyl, who pursued limb salvage pathways since infancy despite early consideration of amputation. His course in turn required staged, multidisciplinary management including multiple corrective reconstructive orthopedic procedures, bilateral tibial osteotomies, and external fixation-based reconstruction, with a major limb-lengthening operation in June 2022, which achieved substantial gains of 11 centimeter left and 7 centimeter right that was complicated by right fixator malfunction requiring operative replacement. After a course of rehabilitation, he then achieved meaningful improvements in both mobility and quality of life, allowing him to return to high-demand athletics, including wrestling. Due to progressive right ankle pain and instability from worsening alignment, a revised right ankle realignment and reconstruction with distal tibia osteotomy and internal fixation was performed in June 2025. The post-operative course was complicated by poor wound healing of the right medial foot that progressed to exposed bone and Staphylococcus epidermidis osteomyelitis requiring excisional debridement in September 2025. Margins were unable to exclude residual infection. Management with wound-vacuum therapy and prolonged intravenous daptomycin followed by oral doxycycline suppression pending hardware removal was confirmed in December 2025 with coordinated outpatient infusion, rehabilitation, and wound care follow-up.
Conclusion: This case demonstrates patient-centered tradeoffs between limb salvage and amputation, the rationale behind elective staged reconstruction to optimize alignment and function, and the importance of multidisciplinary surveillance for late complications.
Keywords: Fibular hemimelia, ectrodactyly, limb salvage, congenital limb deficiency, pediatric orthopedics.
Fibular hemimelia (FH) is a longitudinal postaxial limb deficiency characterized by hypoplasia or aplasia of the fibula in infants, commonly accompanied by ankle or foot dysplasia and leg-length discrepancy throughout early fetal development [1,2]. The unilateral incidence is reported as roughly 1 in 40,000 live births, with a range of 1/25,000–1/40,000 [3,4,5,6]. Bilateral FH, however, is considerably more rare and complex [2,7]. Typical associated deformities observed include ankle valgus and relative deficiency of the lateral column of the foot; however are exceptionally rare [1,8].
Ectrodactyly, also known as split-hand/foot malformation (SHFM), is a genetically and phenotypically heterogeneous defect of central-ray formation that produces a median cleft with variable syndactyly or aplasia [9]. The concurrence of bilateral FH with ectrodactyly involving both upper and lower extremities is exceptionally rare and has been described only in a few cases [3,4,5,6,10,11]. The precise prevalence of concordant FH and SHFM remains unknown [7]. The patient’s associated split hand foot phenotype is consistent with disruptions in early limb-bud patterning and impaired maintenance of the apical ectodermal ridge (AER) [12], a signaling center responsible for coordinating proximodistal outgrowth interacting with anteroposterior and dorsoventral patterning programs. Perturbation of the AER is a recurring mechanistic theme across SFHM models and human loci [13].
Genetic data indicate the 7q21.3 region containing Distal-less homeobox 5/6 (DLX5/6) in SHFM1, with reports of a pathogenic copy number or regulatory disruptions involving this locus associated with enhancer landscapes [4,14]. In contrast, in tumor protein p63, a p53 family transcription factor, essential for ectodermal development, is linked to AER stratification, directly modulating Dlx gene expression, with data demonstrating that p63 perturbation decreases Dlx expression and when combined with partial Dlx5/6 loss, can produce severe limb phenotypes supporting the p63-DLX axis in SHFM pathogenesis [11]. Clinically, central ray deficiency seen in SHFM can impair push off during gait in the foot as well as grasp in the hand, which in turn reinforces the idea that reconstructive planning must integrate both bony architecture and functional goals across the upper and lower extremity [15]. In this report, we describe a 19-year-old male diagnosed at birth with bilateral FH and tetramelic ectrodactyly, and we contextualize his phenotype and longitudinal reconstructive course within the current epidemiology and developmental biology of these conditions.
We present the case of a 19-year-old male with congenital bilateral FH and tetramelic ectrodactyly. Which was characterized by long-standing ankle instability and valgus foot alignment with split foot deformities and ectrodactyly of the left hand with variable syndactyly; while having otherwise normal facial features, intact neurological function, and no known internal congenital anomalies with a normal torso. Pregnancy history was non-contributory; however, prenatal ultrasound and genetic testing identified the limb deformities, while subsequent genetic counseling did not identify a unifying syndrome. Family history includes a sister with Turner syndrome and distant maternal relatives with missing digits without any direct family history of FH.
From early life, the patient pursued a limb salvage course despite recommendations for lower-extremity amputation given the severity of the malformation present. At 15 months of age, his syndactyly of the left hand (Fig. 1) was surgically corrected, followed by multiple left-hand reconstructive procedures, including osteotomy interventions in childhood to address progressive curvature and contracture through long finger osteotomy in 2009 and additional thumb and phalanx osteotomy in 2011.
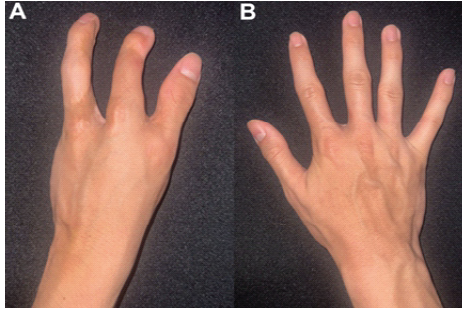
Figure 1: Bilateral split-hand malformation (ectrodactyly). Clinical photographs of the patient’s hands demonstrating ectrodactyly with central ray deficiency. (a) Right hand and (b) left hand are shown, highlighting the characteristic “splithand” configuration and reduced central digits. Images were obtained during clinical evaluation and are presented without identifying features.
He also undertook multiple lower-extremity alignment operations, including bilateral tibial osteotomies with subsequent hardware removal in 2008, and experienced a period of chronic stress fractures between age 8 and 11, which was attributed to limited heel support and increased activity demands. This was managed concurrently with physical therapy, bracing, supports, massage, and analgesics. Imaging during the period of staged reconstruction documented the absence of both fibulae consistent with bilateral FH, congenitally shortened tibiae with postsurgical osteotomy, changes, prior hindfoot arthrodesis changes, external fixation devices, and extremely rocker-bottom pes planus deformity patterns.
To address limb length discrepancies seen and improve both quality of life and function, he underwent a limb-lengthening procedure in June 2022, which showcases an 11 cm left and 7 cm right substantial gain. However, this was complicated by a right fixator malfunction requiring operative replacement in November 2022, followed by prolonged rehabilitation from wheelchair to crutches, followed by eventual fixator removals in the left in July 2023, and right in November 2023, with return to higher activity taking place by late 2023 into early 2024, including recreational sports with ankle soreness due to overactivity past progressed limits. Post-lengthening procedure, worsening right ankle pain and instability from progressive misalignment developed with the sensation of the ankle “snapping” with weight bearing prompting right ankle reconstruction in June 2025 focusing on ankle realignment with distal tibial osteotomy and internal fixation with plates, screws and transfixing wires (Fig. 2). Postoperatively, the patient reported intermittent paresthesia with decreased toe sensation attributed to cast compression, later developing an acute episode of knee pain and swelling with effusion in early August 2025 that was managed conservatively and he transitioned to a walking boot with crutches as needed.

Figure 2: Radiographic confirmation of bilateral fibular hemimelia. Lateral radiographs of the lower extremities demonstrating the tibiae with congenital absence/aplasia of the fibulae bilaterally, consistent with bilateral fibular hemimelia. These images illustrate the underlying bony deficiency that contributes to limblength discrepancy and ankle/hindfoot malalignment, framing the reconstructive pathway and subsequent complications described in the case.
In September 2025, his course was complicated by a poorly healing right medial foot wound accompanied by worsening pain with visible exposed bone containing green-tinged drainage progressing in depth despite outpatient wound care management. He underwent excisional debridement of the wound to the level of the bone in September 2025, with pathology positive for osteomyelitis with cultures growing Staphylococcus epidermidis; however, margin assessment could not exclude residual osteomyelitis. Infectious disease, in turn, recommended prolonged therapy with IV Daptomycin through December 2025, followed by oral doxycycline suppressive therapy until hardware removal could be completed with a wound vacuum being utilized after discharge. Complete blood count, basic metabolic panel was monitored, and a physical therapy evaluation was also arranged post discharge. A peripherally inserted central catheter line was placed in late October 2025 and was then removed in December 2025 as his IV course concluded, as both the wound-vacuum and IV antibiotics had been discontinued. The patient was ambulating (Fig. 3) with crutches while the wound continued to heal, reporting only skin irritation due to wound-vacuum dressings and tape.

Figure 3:Tetramelic ectrodactyly of the feet. Clinical photograph of the patient’s feet demonstrating tetramelic ectrodactyly with central ray deficiency. The image highlights the functional implications of ray absence for shoe wear, forefoot stability, and push-off mechanics, which informed longitudinal management decisions and counseling regarding expected functional outcomes. Images were obtained during clinical evaluation and are presented.
This case illustrates longitudinal, staged management of congenital FH complicated with associated foot-ray deficiency and the downstream consequences of pursuing limb reconstruction through skeletal maturity, including the need for repeat corrective operations with the risk of late infectious complications around retained hardware. The patient’s tetramelic ectrodactyly with central-ray deficiency of the feet is shown in Fig. 3, reinforces the functional relevance of ray deficiency to shoe wear and push-off mechanics.
Patient management
Management of FH is elective and goal-directed due to the variable deformity spectrum and patient priorities of treatment selection, including limb length equalization, cosmesis, tolerance for repeated procedures, athletic participation, and plantigrade foot balanced with surgical burden and complication risk [8]. Radiographic confirmation of bilateral FH provided in Fig. 2 demonstrates tibial presence with absence of the fibulae bilaterally. In modern limb-salavage pathways, clinical priorities are to stabilize the laterally deficient valgus-prone ankle; correct complex hindfoot malalignment, and address ray deficiency when it affects shoe-wear and pushoff as well as sequence osteonities, soft-tissue balancing, and staged lengthening to achieve a durable plantigrade foot without functional limb-length restoration [1,8]. Within these frameworks, the paley shortening osteotomy realignment distal tibia procedure is used when the distal fibula is hypoplastic and ankle valgus is dynamic, while the Paley SUPERankle is utilized for fixed equino-valgus deformity, and more complex hindfoot malalignment requires supramalleolar shortening and realignment osteotomy with adjunctive osteotomies and soft-tissue reconstruction to obtain a stabilized plantigrade foot [1]. In this patient’s course, objective anthropometrics documented an increase in height from 1.562 m to 1.6 m between January 2023 and August 2025, consistent with the cumulative effect of growth across adolescence and the reconstructive lengthening trajectory pursued during this period.
A core management decision in FH is amputation with prosthetic fitting versus limb reconstruction and lengthening, as this choice is preference sensitive due to each pathway having a number of intense surgeries, increased rehabilitation time, complication exposures, and long-term function considerations. Comparative outcomes showcase data that suggest that both approaches can yield functional and psychosocial benefit. However, reconstruction is associated with a higher rate of compilation burden, while amputation is associated with fewer procedures and, in some cohorts and meta-analytic data, higher patient satisfaction [16,17]. Clinicians may recommend early amputation for severe deficiency when there is an unlikely opportunity for plantigrade braceable foot despite reconstruction, or when limb length discrepancy and deformity would require multiple staged operations with prolonged rehabilitation [8]. However, patients who prioritize retaining native limbs may accept an extended surgical process to preserve body image, proprioception, or, after having exhausted all available options, when reconstructive techniques can reasonably achieve a stable plantigrade foot and length equalization [1]. In this case, the patient’s preference for limb salvage was reinforced by concerns about phantom limb pain associated with amputees. While phantom limb pain is reported variably across populations, it is a meaningful patient-perceived risk that can impact shared decision making and thus underscores the importance of values-based counseling rather than purely anatomic pathways [18,19].
Limb lengthening can, in turn, provide a substantial increase in functional gains but also carries a predictable morbidity risk that should be managed with structured analgesia, physical therapy, close monitoring for mechanical and infectious complications, and sleep support. Complication risks during distraction osteogenesis increases with increased lengthening demands and treatment complexity, pediatric cohorts demonstrate that severity and frequency of complications can be modeled to reflect the magnitude and tempo of the distraction [20]. External fixation is also associated strongly with pin tract infections as a common adverse effect requiring standardized pin site care protocols and early treatment to prevent its progression to deep infection of osteomyelitis [21]. Fracture is also a recognized complication after fixator removal in pediatric lengthening, with risk influenced by the degree of lengthening and the underlying etiology, and therefore functional return-to-sport requires conditioning and realistic counseling regarding reinjury risk [22]. This patient’s record documents progression to high-demand athletic participation, including wrestling, consistent with the functional intent of reconstitution and reflecting meaningful improvements in mobility and quality of life after the reconstructive course. Coinciding with such, the clinical course also demonstrates the durability costs of limb salvage as the patient sustained a right malleolar fracture during wrestling and later requiring ongoing management for a chronic non-healing medial foot wound, underscoring the reality that even a “successful” reconstruction can leave patients with activity limitations, increased susceptibility to injury, and residual pain.
Psychosocial considerations should be treated as part of the core clinical outcomes rather than secondary endpoints. Ilizarov-based lengthening is a psychologically stressful procedure in the short term due to prolonged treatment duration, sleep disruption, pain, and social prescription, yet long-term follow-up studies suggest broadly normal psychosocial functioning while still reporting residual physical constraints, pain, and reduced motor function as compared with their normative peers [23]. This aligns with the patient’s narrative, dictating that recovery was isolating and emotionally draining while ultimately enabling social reintegration and athletic identity through perceived success of the reconstructive management including autonomy, peer participation, and mental health, rather than only radiographic alignment. The later infectious complications in his course highlighted a known risk profile seen in prolonged reconstructive pathways due to retained and revised repeated incisions increasing susceptibility to soft-tissue compromise and deep infection, making multidisciplinary follow-up with orthopedics, podiatry, infectious disease, rehabilitation, and wound care essential when chronic wounds and suspected osteomyelitis emerged.
This case highlights and emphasizes the complex and long-term management of congenital bilateral FH with associated tetramelic ectrodactyly, simultaneously emphasizing the diversity in which functional outcomes are shaped not only by the initial anatomy but also by the total effects of staged reconstruction across growth. In turn, this patient’s course showcases how limb salvage can, in turn, provide meaningful gains in quality of life, mobility, and participation through sequenced osteotomies, soft-tissue balancing, and limb lengthening while also underscoring the substantial impact of treatment burden, prolonged rehabilitation, and ongoing susceptibility to complications. The development of a chronic non-healing wound with biopsy-confirmed osteomyelitis following ankle malalignment in particular illustrates the importance and need for postoperative surveillance, vigilance of care, multidisciplinary coordination, and individualized wound care and antimicrobial strategies when hardware must be retained. Ultimately, this report emphasizes that amputation and limb salvage pathways represent important yet distinct, preference-sensitive pathways, with shared decision making integrating psychosocial context, realistic counseling on complication risk and operative timelines, and patient values being integral in achieving positive outcomes that align with patient-defined goals.
Limb-salvage reconstruction for complex congenital limb deficiencies such as concordant bilateral fibular hemimelia with tetramelic ectrodactyly can preserve function but is frequently prolonged and complication-prone; careful patient selection, staged planning, and close multidisciplinary follow-up are essential, with early counseling that compares expected outcomes of salvage versus amputation.
References
- 1. Paley D. Surgical reconstruction for fibular hemimelia. J Child Orthop 2016;10:557-83. [Google Scholar] [PubMed]
- 2. Birch JG, Lincoln TL, Mack PW, Birch CM. Congenital fibular deficiency: A review of thirty years’ experience at one institution. J Pediatr Orthop 2011;31:363-70. [Google Scholar] [PubMed]
- 3. Lin G, Xu N, Xi R. Apical ectodermal ridge regulates three principal axes of limb development and shapes the individual digits. Front Cell Dev Biol 2020;8:611228. [Google Scholar] [PubMed]
- 4. Robledo RF, Rajan L, Li X, Lufkin T. The Dlx5 and Dlx6 homeobox genes are essential for craniofacial, axial, and appendicular skeletal development. Genes Dev 2002;16:1089-101. [Google Scholar] [PubMed]
- 5. Wang X, Xin Q, Li L, Li J, Zhang C, Qiu R, et al. Exome sequencing reveals a heterozygous DLX5 mutation in a Chinese family with autosomal-dominant split-hand/foot malformation. Eur J Hum Genet 2014;22:1105-10. [Google Scholar] [PubMed]
- 6. Kantaputra PN, Carlson BM. Genetic regulatory pathways of split-hand/foot malformation. Clin Genet 2019;95:132-9. [Google Scholar] [PubMed]
- 7. Manasra MR, Azzam S, Al-Tarawneh S. A case of congenital fibular hemimelia associated with skeletal and non-skeletal malformations. World J Clin Cases 2025;13:e11879310. [Google Scholar] [PubMed]
- 8. Fuller CB, Shannon CE, Paley D. Lengthening reconstruction surgery for fibular hemimelia: A review. Children (Basel) 2021;8:467. [Google Scholar] [PubMed]
- 9. Sowińska-Seidler A, Socha M, Jamsheer A. Split-hand/foot malformation-molecular cause and implications in genetic counseling. Hum Genet 2014;133:1157-72. [Google Scholar] [PubMed]
- 10. Panman L, Zeller R. Patterning the limb before and after SHH signalling. Trends Genet 2003;19:359-66. [Google Scholar] [PubMed]
- 11. Lo Iacono N, Mantero S, Chiarelli A, Garcia E, Mills AA, Morasso MI, et al. Regulation of Dlx5 and Dlx6 gene expression by p63 is involved in EEC and SHFM congenital limb defects. Development 2008;135:1377-88. [Google Scholar] [PubMed]
- 12. Kouwenhoven EN, Van Heeringen SJ, Tena JJ, Oti M, Dutilh BE, Alonso ME, et al. Genome-wide profiling of p63 DNA-binding sites identifies an element that regulates gene expression during limb development in the 7q21 SHFM1 locus. PLoS Genet 2010;6:e1001065. [Google Scholar] [PubMed]
- 13. Duijf PH, Van Bokhoven H, Brunner HG. Pathogenesis of split-hand/split-foot malformation. Hum Mol Genet 2003;12:R51-60. [Google Scholar] [PubMed]
- 14. Velinov M, Ahmad A, Brown-Kipphut B, Shafiq M, Blau J, Cooma R, et al. A 0.7 Mb de novo duplication at 7q21.3 including the genes DLX5 and DLX6 in a patient with split-hand/split-foot malformation. Am J Med Genet A 2012;158A:3201-6. [Google Scholar] [PubMed]
- 15. Gurrieri F, Everman DB. Clinical, genetic, and molecular aspects of split-hand/foot malformation: An update. Am J Med Genet A 2013;161A:2860-72. [Google Scholar] [PubMed]
- 16. Birch JG, Paley D, Herzenberg JE, Morton A, Ward S, Riddle R, et al. Amputation versus staged reconstruction for severe fibular hemimelia: Assessment of psychosocial and quality-of-life status and physical functioning in childhood. JBJS Open Access 2019;4:e0053. [Google Scholar] [PubMed]
- 17. Elmherig A, Ahmed AF, Hegazy A, Herzenberg JE, Ibrahim T. Amputation versus limb reconstruction for fibula hemimelia: A meta-analysis. J Pediatr Orthop 2020;40:425-30. [Google Scholar] [PubMed]
- 18. Melzack R, Israel R, Lacroix R, Schultz G. Phantom limbs in people with congenital limb deficiency or amputation in early childhood. Brain 1997;120:1603-20. [Google Scholar] [PubMed]
- 19. Diers M, Fuchs X, Bekrater-Bodmann R, Flor H. Prevalence of phantom phenomena in congenital and early-life amputees. J Pain 2023;24:502-8. [Google Scholar] [PubMed]
- 20. Antoci V, Ono CM, Antoci V Jr., Raney EM. Bone lengthening in children: How to predict the complications rate and complexity? J Pediatr Orthop 2006;26:634-40. [Google Scholar] [PubMed]
- 21. Kazmers NH, Fragomen AT, Rozbruch SR. Prevention of pin site infection in external fixation: A review of the literature. Strat Trauma Limb Reconstr 2016;11:75-85. [Google Scholar] [PubMed]
- 22. Launay F, Younsi R, Pithioux M, Chabrand P, Bollini G, Jouve JL. Fracture following lower limb lengthening in children. A series of 58 patients. Orthop Traumatol Surg Res 2013;99:72-9. [Google Scholar] [PubMed]
- 23. Moraal JM, Elzinga-Plomp A, Jongmans MJ, Roermund PM, Flikweert PE, Castelein RM, et al. Long-term psychosocial functioning after Ilizarov limb lengthening during childhood. Acta Orthop 2009;80:704-10. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Radiation-Associated Femoral Nonunion and Fixation Failure Following Limb-Salvage Surgery for Thigh Soft-tissue Sarcoma: Two Case Reports and a Review of the Literature
July 1, 2026 Radiation-Associated Femoral Nonunion and Fixation Failure Following Limb-Salvage Surgery for Thigh Soft-tissue Sarcoma: Two Case Reports and a Review of the Literature July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases
July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases July 1, 2026 Severe Metallosis after Tumor Mega-Prosthesis: Revise or Retain? – A Case Series
July 1, 2026 Severe Metallosis after Tumor Mega-Prosthesis: Revise or Retain? – A Case Series July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis
July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis