
Outcomes in open fractures are often determined by how well timing, biology, stability, and reconstruction are integrated from the first decision onward.
Dr. Janki Sharan Bhadani, Department of Orthopaedics, Paras HMRI Hospital, Patna, India. E-mail: jsbhadani@gmail.com
Open fractures remain among the most challenging injuries in trauma surgery. They involve contamination, soft-tissue disruption, skeletal instability, and often systemic injury. While traditionally defined by communication between the fracture and the external environment, an open fracture is better understood as a soft tissue injury in which the bone is broken [1]. Prognosis is determined not only by fracture pattern but also by contamination, vascularity, bone loss, host factors, and the quality of care delivered from the earliest hours. The goals of management remain consistent: prevent infection; preserve viable tissue; restore stability; facilitate reconstruction; and promote healing of soft tissue as well as bone to restore function. These objectives depend on the integration of sound principles across the entire pathway of care. The Gustilo-Anderson classification systems remain useful in guiding communication and treatment planning, but they do not replace judgement. [2] Injury severity is often best judged in the operating room, particularly after debridement [3]. Factors such as contamination, periosteal stripping, vascular injury, and bone loss frequently modify both prognosis and strategy.
The management of open fractures is often presented as algorithmic, but in reality, decision-making is frequently more nuanced. Some injuries are straightforward, where the path toward salvage or amputation is relatively clear from the outset. However, many injuries fall into a grey zone where the true extent of damage only becomes evident over time, with repeated assessment or during surgical exploration. This is particularly true when external appearance does not reflect the severity of underlying soft tissue damage, contamination, or tissue devitalisation [4]. An important example is the persistent misconception that an open fracture protects against compartment syndrome because the wound acts as a decompression. This is not always true. Compartment syndrome can still occur in open fractures, even within the same compartment that is open, and failure to recognize this can have serious consequences. Similarly, a seemingly small or benign wound may hide extensive muscle crushing, comminution, or associated degloving injury that fundamentally changes classification and management [5]. Delayed presentation adds another layer of complexity, as tissue viability may evolve and alter salvage potential. What appears salvageable at one point may become non-viable later, while other injuries that appear devastating may still be reconstructed successfully. These examples emphasise that classification systems are guides, not substitutes for judgement. Optimal management of complex open fractures depends on repeated reassessment, thoughtful interpretation of evolving findings, and experience. Much of the expertise in open fracture care lies in recognizing when the injury is not what it first appears to be (Fig. 1).
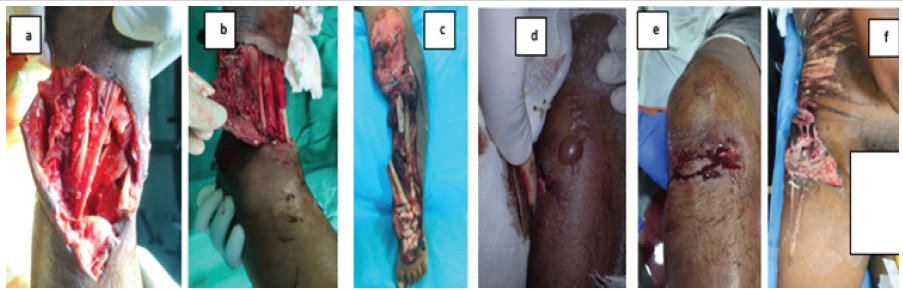
Figure 1: Clinical scenarios illustrating evolving assessment in open fractures. Injury severity and management are not always apparent at presentation. (a, b) Severe Gustilo-Anderson type III B fracture injuries with preserved vascularity, where salvage remains feasible. (c) Delayed presentation of Gustilo-Anderson type III C fracture with a non-salvageable limb. (d) Low-grade open fracture complicated by compartment syndrome, showing that open fractures do not preclude this diagnosis, even in the same open compartment. (e) An apparently benign wound was upgraded to type III after exploration revealed extensive underlying soft tissue injury. (f) Open fracture associated with Morel-Lavallée lesion. These examples highlight the evolving nature of assessment and decision-making in open fractures.
Few concepts in trauma care have been as enduring as the 6-h rule. Although rooted in historical surgical principles, it is largely based on animal studies, with no clear consensus from human data [6]. Modern evidence has shifted the focus from rigid timing thresholds to the quality and sequence of care [7]. The emphasis is no longer on an arbitrary deadline for every open fracture but on ensuring that debridement is performed early with proper expertise, planning, and adequate facilities rather than hurriedly and inadequately. What truly matters is that antibiotics, debridement, and stabilisation are delivered promptly and appropriately. Early systemic antibiotics, ideally started within the 1st hour, remain a key determinant of infection prevention. Meticulous debridement and appropriate irrigation should be done by an experienced surgeon to continue to form the biological foundation of treatment [8]. The evolution in thinking has been away from dogma and toward evidence-informed judgement, where urgency is preserved, but rigid rules are replaced by thoughtful prioritisation. Initial skeletal stabilisation is central to this philosophy. It restores alignment, protects soft tissues, facilitates wound management, and supports both healing and staged reconstruction [7]. External fixation remains invaluable in severe soft tissue injury, contamination, vascular compromise, and damage control situations, while early definitive fixation may be appropriate in selected injuries [9] (Fig. 2).
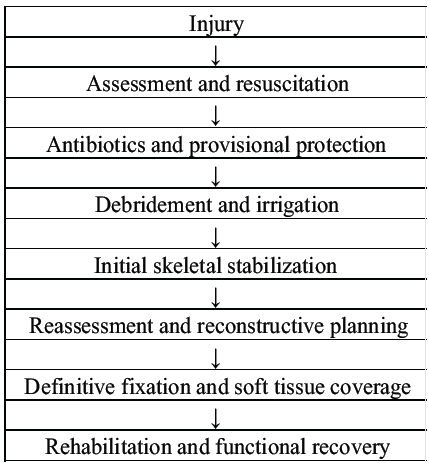
Figure 2: Integrated pathway in open fracture care.
In selected high-risk injuries, local antibiotic strategies, including antibiotic beads or spacers to manage dead space, may complement systemic antibiotics. However, these adjuncts do not replace adequate debridement, removal of devitalised tissue, and stable fixation. Debridement, irrigation, and stabilisation remain complementary, not competing, priorities [10,11]. Our understanding of managing open fractures evolves over time (Table 1).
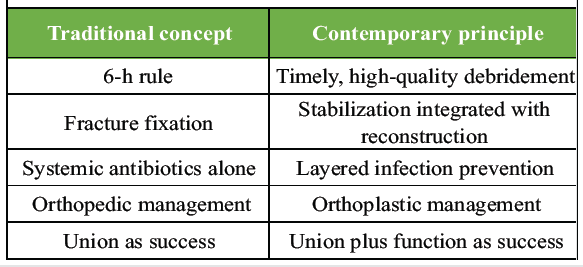
Table 1: From traditional dogma to contemporary principles
Fixation and soft-tissue coverage should not be treated as separate stages managed in sequence but as linked components of one reconstructive strategy. Pin placement, provisional constructs, and definitive fixation choices should anticipate flap options, coverage timing, and potential bone reconstruction. This shift from sequential management to integrated planning has been one of the most important advances in modern open fracture care [12,13].
A common misconception is that success in open fracture care is determined in the initial operation. In reality, open fracture treatment is often staged. Repeat debridement, conversion from temporary to definitive fixation, soft-tissue reconstruction, bone reconstruction, and rehabilitation may all influence outcomes as much as the first procedure [4]. This is true in severe injuries, where the pathway may include staged fixation, local antibiotic spacers, bone grafting, or more complex reconstruction. Rehabilitation also plays a crucial role, as functional recovery depends not simply on union or wound closure but on preserving motion, restoring load transfer, and addressing long-term consequences of injury. The key determinants influencing these outcomes are summarized in Fig. 3. [14] The true success of treatment is often measured months later, in a healed limb that functions.
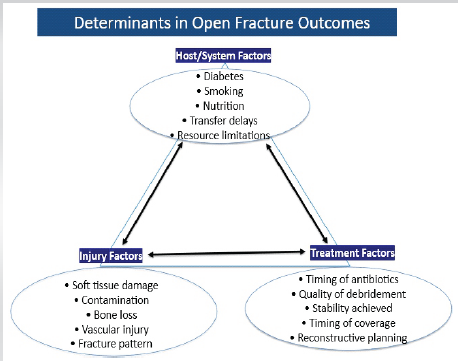
Figure 3: Key determinants of outcome in open fractures [14].
The challenge in open fracture care is to integrate timing, biology, stability, and reconstruction more intelligently from the first decision onwards. That includes recognizing the importance of host factors, system related factors, and resource limitations. In settings of constrained infrastructure or limited Orthoplastic access, timely transfer may itself be an important decision. Outcomes in open fractures are rarely determined by one antibiotic, one debridement, one fixation construct, or one timing threshold. Therefore, the outcome is also determined by how well these principles are integrated from injury through reconstruction and rehabilitation.
The future of open fracture care lies not in choosing between timing, fixation, biology, or reconstruction, but in integrating all four from the very first decision, because those first decisions often determine everything that follows.
Successful management of open fractures is not defined by a single operation but by how well early decisions integrate timely debridement, stable fixation, infection control, and planned reconstruction. Repeated reassessment, coordinated orthoplastic strategy, and structured rehabilitation are essential, as final outcomes depend on restoring both biological healing and functional recovery.
References
- 1. Diwan A, Eberlin KR, Smith RM. The principles and practice of open fracture care, 2018.Chin J Traumatol. 2018 Aug;21(4):187-192. doi: 10.1016/j.cjtee.2018.01.002. Epub 2018 Feb 21. Erratum in: Chin J Traumatol. 2025 Sep;28(5):386-387. doi:10.1016/j.cjtee.2020.12.004. PMID: 29555119; PMCID: PMC6085196. [Google Scholar] [PubMed] [CrossRef]
- 2. Rajasekaran S, Sabapathy SR. A philosophy of care of open injuries based on the Ganga hospital score. Injury. 2007;38(2):137-146. doi:10.1016/j.injury.2006.04.135 [Google Scholar] [PubMed] [CrossRef]
- 3. Axelrod D, Comeau-Gauthier M, Prada C, Bzovsky S, Heels-Ansdell D, Petrisor B, Jeray K, Bhandari M, Schemitsch E, Sprague S. Change in Gustilo-Anderson classification at time of surgery does not increase risk for surgical site infection in patients with open fractures: A secondary analysis of a multicenter, prospective randomized controlled trial. OTA Int. 2022 Dec 28;6(1): e231. doi: 10.1097/OI9.0000000000000231. PMID: 36760661; PMCID: PMC9904191. [Google Scholar] [PubMed] [CrossRef]
- 4. Gustilo RB, Mendoza RM, Williams DN. Problems in the management of type III (severe) open fractures: a new classification of type III open fractures. J Trauma. 1984;24(8):742-746. doi:10.1097/00005373-198408000-00009 [Google Scholar] [PubMed] [CrossRef]
- 5. Gamulin A, Wuarin L, Zingg M, Belinga P, Cunningham G, Gonzalez AI. Association between open tibia fractures and acute compartment syndrome: A retrospective cohort study. Orthop Traumatol Surg Res. 2022;108(5):103188. doi: 10.1016/j.otsr.2021.103188. [Google Scholar] [PubMed] [CrossRef]
- 6. Nicolaides M, Pafitanis G, Vris A. Open tibial fractures: An overview. J Clin Orthop Trauma. 2021; 20:101483. Published 2021 Jun 24. doi: 10.1016/j.jcot.2021.101483 [Google Scholar] [PubMed] [CrossRef]
- 7. Dheenadhayalan J, Nagashree V, Devendra A, Velmurugesan PS, Rajasekaran S. Management of open fractures: A narrative review. J Clin Orthop Trauma. 2023;44:102246. Published 2023 Sep 1. doi: 10.1016/j.jcot.2023.102246 [Google Scholar] [PubMed] [CrossRef]
- 8. Diefenbeck M, Haustedt N, Schmidt HG. Surgical debridement to optimise wound conditions and healing. Int Wound J. 2013;10 Suppl 1(Suppl 1):43-47. doi:10.1111/iwj.12187 [Google Scholar] [PubMed] [CrossRef]
- 9. Mussatto JCDA, Balsimelli F, Mussatto GDA, Zamboni C, Christian RW, Mercadante MT. Interference of external damage control fixation in definitive osteosynthesis. Acta Ortop Bras. 2022;30(4): e250322. Published 2022 Aug 26. doi:10.1590/1413-785220223004e250322 [Google Scholar] [PubMed] [CrossRef]
- 10. Whiting PS, Obremskey W, Johal H, Shearer D, Volgas D, Balogh ZJ. Open fractures: evidence-based best practices. OTA Int. 2024;7(3 Suppl): e313. Published 2024 May 3. doi:10.1097/OI9.0000000000000313 [Google Scholar] [PubMed] [CrossRef]
- 11. Hake ME, Young H, Hak DJ, Stahel PF, Hammerberg EM, Mauffrey C. Local antibiotic therapy strategies in orthopaedic trauma: Practical tips and tricks and review of the literature. Injury. 2015;46(8):1447-1456. doi: 10.1016/j.injury.2015.05.008 [Google Scholar] [PubMed] [CrossRef]
- 12. Gopal S, Majumder S, Batchelor AG, Knight SL, De Boer P, Smith RM. Fix and flap: the radical orthopaedic and plastic treatment of severe open fractures of the tibia. J Bone Joint Surg Br. 2000;82(7):959-966. doi:10.1302/0301-620x.82b7.10482 [Google Scholar] [PubMed] [CrossRef]
- 13. Agashe VM, Bhadani JS, Maini L. Beyond Hardware: The Orthoplastic Approach to Managing Infected Nonunions. Indian J Orthop. 2024;58(12):1777-1781. Published 2024 Nov 23. doi:10.1007/s43465-024-01289-y [Google Scholar] [PubMed] [CrossRef]
- 14. Coombs J, Billow D, Cereijo C, Patterson B, Pinney S. Current Concept Review: Risk Factors for Infection Following Open Fractures. Orthop Res Rev. 2022; 14:383-391.Published 2022 Nov 7. doi:10.2147/ORR.S384845 [Google Scholar] [PubMed] [CrossRef]



Related Articles in Journal of Orthopaedic Case Reports
 January 10, 2022 Late Presentation of Palmar Dislocation of the Fifth Metacarpal Bone: Review of the Literature, Treatment Algorithm, and Case Report
January 10, 2022 Late Presentation of Palmar Dislocation of the Fifth Metacarpal Bone: Review of the Literature, Treatment Algorithm, and Case Report January 10, 2024 Kirschner Wires and Bone Allograft Salvage Finger Motion in Pathologic Fracture of Middle Phalanx Enchondroma: A Case Report
January 10, 2024 Kirschner Wires and Bone Allograft Salvage Finger Motion in Pathologic Fracture of Middle Phalanx Enchondroma: A Case Report April 1, 2026 Novel Technique for Fracture Non-Union in Children – A Case Report
April 1, 2026 Novel Technique for Fracture Non-Union in Children – A Case Report September 29, 2019 Secretory Paravertebral Paraganglioma of the Lumbar Spine: A Case Report and Review of Literature
September 29, 2019 Secretory Paravertebral Paraganglioma of the Lumbar Spine: A Case Report and Review of Literature