
Singh Index serves as a simple and reliable bedside radiographic tool that can guide fixation choice in elderly femoral neck fractures, allowing safe selection of uncemented hemiarthroplasty in high-risk patients with adequate bone quality while minimizing cement-related complications.
Dr Saurabh G Fate, Department of Orthopaedics, Grant Government Medical College and Sir JJ Group of Hospitals, Mumbai, Maharashtra, India. E-mail: fatesaurabh21@gmail.com
Abstract
Introduction: Femoral neck fractures in elderly patients require careful consideration of both bone quality and perioperative risk when selecting between cemented and uncemented hemiarthroplasty. The Singh index provides a simple radiographic assessment of trabecular bone quality. This study evaluates its utility in guiding fixation type selection in high-risk patients.
Materials and Methods: This retrospective comparative case series included 18 elderly patients with displaced femoral neck fractures treated with hemiarthroplasty. Patients were stratified based on the Singh index, with those who had a score of ≥4 undergoing uncemented fixation and those with a score <4 undergoing cemented fixation. All patients were classified as American Society of Anaesthesiologists Grade III or IV. Functional outcomes were assessed using the Harris Hip Score at follow-up.
Results: Pre-operative decision-making based on Singh index correlated with intraoperative findings in 16 out of 18 cases (88.9%). In two cases, intraoperative assessment necessitated a change from uncemented to cemented fixation due to poor bone quality. At a mean follow-up of 6 months, the mean Harris Hip Score was 82.4 in the uncemented group and 78.6 in the cemented group. No cases of bone cement implantation syndrome were observed in the uncemented group, supporting safer fixation selection in high-risk patients.
Conclusion: The Singh index is a useful and practical tool for guiding fixation choice in hemiarthroplasty. In high-risk patients with adequate bone quality, uncemented fixation provides satisfactory functional outcomes while avoiding cement-related complications.
Keywords: Femoral neck fracture, hemiarthroplasty, Singh index, bone cement implantation syndrome, American Society of Anaesthesiologists grade, uncemented fixation.
Femoral neck fractures in the elderly are associated with significant morbidity and mortality and require timely surgical intervention to restore mobility and reduce complications. Hemiarthroplasty remains the standard treatment for displaced femoral neck fractures in elderly patients with limited functional demands. However, the choice between cemented and uncemented fixation continues to be debated, as both techniques have distinct advantages and associated risks [1,2,3,4]. The Singh index, first described in 1970, is a radiographic grading system based on the trabecular architecture of the proximal femur and serves as an indirect indicator of bone quality [5]. Although its correlation with bone mineral density has been questioned, it remains a practical and rapid bedside tool that does not require additional imaging modalities, making it particularly useful in emergency settings [6]. Bone cement implantation syndrome (BCIS) is a potentially serious complication associated with cemented arthroplasty, characterised by hypoxia, hypotension, and cardiovascular instability [7]. Recent studies have reaffirmed its clinical relevance, especially in elderly patients with multiple comorbidities, where it contributes to increased perioperative morbidity and mortality [8,9,10]. Uncemented hemiarthroplasty eliminates the risks associated with bone cement and may reduce operative time and intraoperative physiological stress. However, it requires adequate bone quality to achieve stable fixation [2,3]. In this context, a simple and reliable method to assess bone quality preoperatively becomes essential. This study aimed to evaluate the role of the Singh Index in guiding fixation choice in medically fragile patients and to assess its correlation with intraoperative findings and functional outcomes.
This retrospective comparative case series was conducted at a tertiary care institution and included 18 consecutive elderly patients treated for displaced femoral neck fractures between January 2022 and December 2023. The study design was approved by the institutional review board. The sample size was determined based on the inclusion of all eligible patients during the study period. As this was an exploratory study assessing decision-making utility rather than hypothesis testing, a convenience sampling method was adopted, which is consistent with previously published orthopaedic case series. Patients aged 65 years or older presenting with displaced femoral neck fractures (Garden type III or IV) and classified as American Society of Anaesthesiologists (ASA) Grade III or IV were included in the study. Patients with pathological fractures, prior surgery on the ipsilateral hip, inflammatory arthropathies, or those requiring total hip arthroplasty were excluded from the study. Preoperative radiographic assessment included standard anteroposterior pelvis radiographs. The Singh index was calculated on the fractured hip by evaluating trabecular patterns, with grades ranging from 1 to 6. In cases where the fractured side was not clearly assessable, the contralateral hip was used as a reference. The grading was performed independently by two orthopaedic surgeons, and discrepancies were resolved by consensus. Based on the Singh index, patients were stratified into two groups. Patients with a score of 4 or higher were planned for uncemented hemiarthroplasty, whereas those with a score below 4 were planned for cemented fixation. However, intraoperative assessment of bone quality was performed in all cases by evaluating femoral canal morphology, cortical thickness, and broach stability. All procedures were performed using a standard posterior approach under spinal or general anaesthesia. In the cemented group, third-generation cementation techniques were employed, including canal preparation with pulsatile lavage, distal cement restrictor placement, retrograde cement insertion, and pressurisation. In the uncemented group, press-fit stems designed for metaphyseal fixation were used. Representative cases of uncemented and cemented bipolar hemiarthroplasty are illustrated in Figures 1 and 2, respectively.
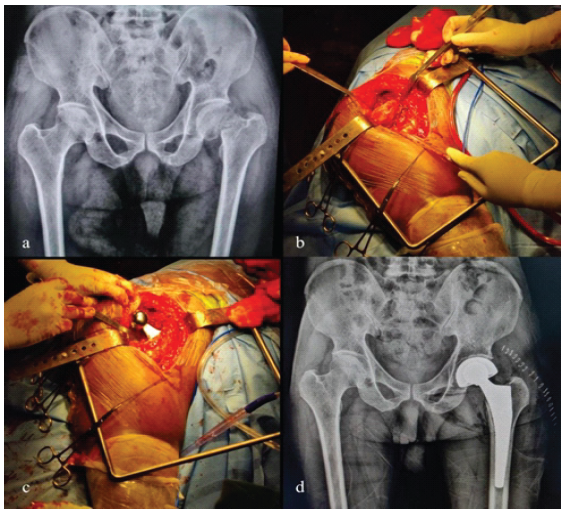
Figure 1: Pre-operative X-rays, intraoperative clinical picture, and post-operative X-rays of a patient with an uncemented bipolar. (a) Pre-operative X-ray pelvis and both hip (PBH) anteroposterior (AP) view of left-sided neck of femur fracture. (b) Intraoperative clinical picture showing exposure. (c) Intraoperative clinical picture showing implant placement. (d) Post-operative X-ray PBH AP view of left-sided uncemented bipolar hemiarthroplasty.

Figure 2: Pre-operative X-rays, intraoperative clinical picture, and post-operative X-rays of a patient with cemented bipolar. (a) Pre-operative X-ray pelvis and both hips (PBH) anteroposterior (AP) view of right-sided neck of femur fracture. (b) Post-operative X-ray PBH AP view of right-sided cemented bipolar hemiarthroplasty. (c) Intraoperative clinical picture showing cement insertion.
Intraoperatively, the pre-operative plan was followed in 16 out of 18 cases. In two patients with a pre-operative Singh index of 4, poor bone quality was noted intraoperatively, leading to a change in fixation from un-cemented to cemented. No cases required conversion from cemented to uncemented fixation. Post-operative management was standardised across both groups, including early mobilisation and physiotherapy. Patients were followed up for a minimum duration of 6 months. Functional outcomes were assessed using the Harris Hip Score, and complications, including BCIS, implant instability, and perioperative mortality, were recorded.
A total of 18 patients were included in the study, with a mean age of 76.5 years (range 69–85 years) (Table 1).
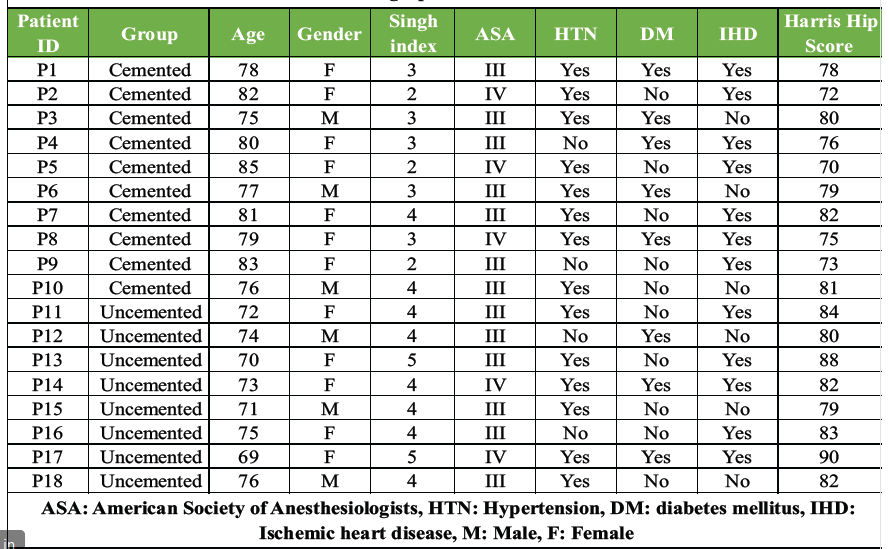
Table 1: Patient demographics and clinical characteristics
The majority of patients were female (66.7%). All patients were classified as ASA Grade III or IV, indicating a high-risk cohort with significant systemic comorbidities. The mean Singh index in the uncemented group was 4.25 (range 4–5), whereas in the cemented group, it was 2.90 (range 2–4), demonstrating a clear distinction in bone quality between the two groups. Pre-operative decision-making based on the Singh index showed strong correlation with intraoperative findings, with agreement in 16 out of 18 cases (88.9%). In two cases (11.1%), intraoperative findings revealed poor bone quality despite a Singh index of 4, leading to conversion from uncemented to cemented fixation. No cases required reverse conversion. Comorbidities were prevalent, with hypertension present in 83.3% of patients, ischaemic heart disease in 66.7%, and diabetes mellitus in 44.4%. At a mean follow-up of 6 months, functional outcomes assessed using the Harris Hip Score were satisfactory in both groups. The uncemented group had a mean Harris Hip score of 82.4 (range 76–90), whereas the cemented group had a mean score of 78.6 (range 70–85). In the uncemented group, 62.5% of patients achieved good to excellent outcomes, whereas in the cemented group, 40% achieved good outcomes. No patient in either group had a poor outcome. No intraoperative mortality was observed. No cases of BCIS were observed in the uncemented group. There were no cases of implant loosening, dislocation, or periprosthetic fracture during follow-up.
The present study demonstrates that the Singh index is a clinically useful and practical tool for guiding fixation choice in elderly patients with femoral neck fractures. The high concordance between pre-operative planning and intraoperative findings (88.9%) observed in this study supports its reliability as a decision-making aid. Previous studies comparing cemented and uncemented hemiarthroplasty have largely focused on functional outcomes and complication rates rather than preoperative decision-making tools. Parker and Gurusamy reported that cemented hemiarthroplasty provides better initial stability but is associated with longer operative times and higher intraoperative physiological stress [4]. Similarly, Figved et al. demonstrated improved fixation with cemented stems but highlighted increased operative complexity [5]. More recent literature has shifted focus toward perioperative risk, particularly the role of BCIS. Rassir et al. reported that BCIS remains associated with increased perioperative morbidity and mortality in elderly patients [10]. Fenelon et al. further demonstrated that the fixation method may influence early mortality, particularly in high-risk patients [11]. Bökeler et al. and Moldovan emphasised that despite advancements in cementation techniques, BCIS continues to remain a clinically relevant concern in elderly patients undergoing cemented hemiarthroplasty [12,13]. Unlike these studies, the present study focuses on pre-operative stratification using the Singh index, which is a significant distinguishing factor. While previous literature has acknowledged the importance of bone quality, there is limited evidence on the use of a simple radiographic index to guide fixation choice in real-time clinical practice. Another important distinction of this study is the integration of intraoperative validation. While the Singh index provided reliable pre-operative guidance, the study highlights that intraoperative assessment remains essential, as evidenced by the two cases requiring a change in fixation strategy. This combined approach enhances clinical decision-making and reduces the risk of inappropriate fixation. In terms of functional outcomes, the findings of this study are comparable to existing literature. The slightly higher Harris Hip scores observed in the uncemented group were consistent with studies suggesting reduced post-operative pain and faster recovery with cementless fixation in appropriately selected patients [4,9]. However, unlike previous studies, this study specifically demonstrates that such outcomes can be achieved safely when guided by the Singh index. Furthermore, this study uniquely focuses on a high-risk population (ASA III/IV), where avoidance of cement-related complications is particularly relevant. The absence of BCIS in the uncemented group reinforces the clinical importance of careful patient selection. The findings of this study suggest that the Singh index can serve as a practical decision-making tool in routine clinical practice, particularly in resource-limited settings where advanced imaging, such as dual-energy X-ray absorptiometry, is not readily available. Its ability to guide fixation choice while correlating well with intraoperative findings enhances its applicability in emergency orthopaedic care.
Limitations:
This study has several limitations, including its small sample size, retrospective design, and relatively short follow-up duration. Although functional outcomes were assessed using the Harris Hip Score, long-term outcomes and detailed statistical comparisons were not performed. The age difference between groups may also represent a confounding factor.
The Singh index is a simple, reliable, and clinically useful tool for guiding fixation choice in hemiarthroplasty for femoral neck fractures. When combined with intraoperative assessment, it allows safe selection of uncemented fixation in patients with adequate bone quality, thereby reducing cement-related complications without compromising functional outcomes.
A combined approach using the Singh index and intraoperative assessment allows individualised fixation strategies in elderly high-risk patients, optimising outcomes while minimising perioperative complications.
References
- 1. Singh M, Nagrath AR, Maini PS. Changes in trabecular pattern of the upper end of the femur as an index of osteoporosis. J Bone Joint Surg Am 1970;52:457-67. [Google Scholar] [PubMed]
- 2. Koot VC, Kesselaer SM, Clevers GJ, De Hooge P, Weits T, Van Der Werken C. Evaluation of the Singh index for measuring osteoporosis. J Bone Joint Surg Br 1996;78:831-4. [Google Scholar] [PubMed]
- 3. Sah AP, Thornhill TS, LeBoff MS, Glowacki J. Correlation of Singh index with bone mineral density. J Bone Joint Surg Am 2007;89:2615-21. [Google Scholar] [PubMed]
- 4. Parker MJ, Gurusamy KS. Cemented versus uncemented hemiarthroplasty. Injury 2006;37:566-73. [Google Scholar] [PubMed]
- 5. Figved W, Opland V, Frihagen F, Jervidalo T, Madsen JE, Nordsletten L. Cemented versus uncemented hemiarthroplasty for displaced femoral neck fractures. Clin Orthop Relat Res 2009;467:2426-35. [Google Scholar] [PubMed]
- 6. Donaldson AJ, Thomson HE, Harper NJ, Kenny NW. Bone cement implantation syndrome. Br J Anaesth 2009;102:12-22. [Google Scholar] [PubMed]
- 7. Taylor F, Wright M, Zhu M. Hemiarthroplasty of the hip with and without cement: A randomized clinical trial. J Bone Joint Surg Am 2012;94:577-83. [Google Scholar] [PubMed]
- 8. Langslet E, Frihagen F, Opland V, Madsen JE, Nordsletten L, Figved W, et al. Cemented versus uncemented hemiarthroplasty for displaced femoral neck fractures: 5-year follow-up of a randomized trial. Clin Orthop Relat Res 2014;472:1291-9. [Google Scholar] [PubMed]
- 9. Inngul C, Enocson A, Hedbeck CJ, Lapidus LJ. Registry study. Acta Orthop 2015;86:286-92. [Google Scholar] [PubMed]
- 10. Rassir R, Schuiling M, Sierevelt IN, Van Der Hoeven CW, Nolte PA. What are the frequency, related mortality, and factors associated with bone cement implantation syndrome in arthroplasty surgery? Clin Orthop Relat Res 2021;479:755-63. [Google Scholar] [PubMed]
- 11. Fenelon C, Murphy EP, Pomeroy E, Murphy RP, Curtin W, Murphy CG. Perioperative mortality after cemented or uncemented hemiarthroplasty for displaced femoral neck fractures-a systematic review and meta-analysis. J Arthroplasty 2021;36:777-87.e1. [Google Scholar] [PubMed]
- 12. Bökeler U, Bühler A, Eschbach D, Ilies C, Liener U, Knauf T. The influence of a modified 3rd generation cementation technique and vacuum mixing of bone cement on the bone cement implantation syndrome (BCIS) in geriatric patients with cemented hemiarthroplasty for femoral neck fractures. Medicina (Kaunas) 2022;58:1587. [Google Scholar] [PubMed]
- 13. Moldovan F. Bone cement implantation syndrome: A rare disaster following cemented hip arthroplasties-clinical considerations supported by case studies. J Pers Med 2023;13:1381. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Primary Hemiarthroplasty for Management of Femoral Neck Fracture in a Patient with Ipsilateral Below-Knee Amputation: A Case Report with Review of Literature
April 1, 2026 Primary Hemiarthroplasty for Management of Femoral Neck Fracture in a Patient with Ipsilateral Below-Knee Amputation: A Case Report with Review of Literature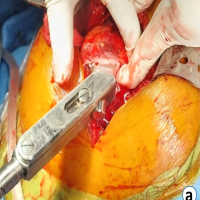 August 6, 2024 Hemodynamic Effects of Bone Cement Implantation in Hip Arthroplasty: Insights from a Prospective Study in Eastern India
August 6, 2024 Hemodynamic Effects of Bone Cement Implantation in Hip Arthroplasty: Insights from a Prospective Study in Eastern India August 1, 2026 Posterior Acetabular Wall Fracture Mimicking a Subcapital Femoral Neck Fracture on Plain Radiographs: A Diagnostic Pitfall and the Role of Intraoperative Fluoroscopy: A Case Report
August 1, 2026 Posterior Acetabular Wall Fracture Mimicking a Subcapital Femoral Neck Fracture on Plain Radiographs: A Diagnostic Pitfall and the Role of Intraoperative Fluoroscopy: A Case Report August 1, 2026 Platelet-Rich Plasma Augmentation of Osteosynthesis in Femoral Neck Fractures: A Prospective Comparative Study Demonstrating Accelerated Union and Improved Function
August 1, 2026 Platelet-Rich Plasma Augmentation of Osteosynthesis in Femoral Neck Fractures: A Prospective Comparative Study Demonstrating Accelerated Union and Improved Function