
The clavipectoral fascial block is an effective and acceptable method for the surgical fixation of clavicle fractures.
Dr. Siddhartha Sinha, Department of Orthopaedics, Hamdard Institute of Medical Sciences and Research, New Delhi - 110 062, India. E-mail: siddharthasinha87@gmail.com
Abstract
Introduction: The clavipectoral fascial plane block (CPB) can be used in clinical situations where general anesthesia (GA) is contraindicated. CPB has been reported to provide a better hemodynamic profile and lower complications compared to GA. This study aimed to evaluate the patient satisfaction, radiological and functional outcomes of CPB in the surgical management of clavicle fractures.
Materials and Methods: A single-arm prospective cohort study was conducted between November 2022 and July 2024. All patients with clavicle fractures meeting the inclusion criteria were operated on with CPB, and conversion to GA was done if required. Pre-operative parameters were measured, and intraoperative monitoring was recorded. Numeric rating scale (NRS) score, quick disabilities of the arm, shoulder, and hand (QuickDASH) score, Constant and Murley score, bone union, and complications were recorded. Post-operative assessment was done at 2 weeks, 6 weeks, and 12 weeks.
Results: Thirty patients with clavicle fractures were operated on using CPB. Hemodynamic stability was maintained intraoperatively in 90% of cases, with no significant elevations in blood pressure or pulse rate. 90% of participants did not require intraoperative fentanyl administration or conversion to GA, and 70% did not necessitate rescue analgesia postoperatively. Statistically significant reduction in NRS pain scores, improvement in QuickDASH functional scores, and improved Constant–Murley shoulder function scores over 12 weeks were noted. All fractures united with visible callus formation at 12 weeks. The majority (73.3%) experienced no post-operative complications, and high levels of patient satisfaction were reported.
Conclusion: The findings indicate that CPB represents a safe and effective modality for achieving surgical anesthesia in clavicle fracture osteosynthesis and provide favourable patient-reported outcomes.
Keywords: Clavicle, shoulder, patient satisfaction, pain, clavipectoral block, clavicle fracture osteosynthesis.
Clavicle fractures have been treated traditionally by non-operative methods; however, there has been a recent trend toward operative methods, as it allows for early rehabilitation, decrease the chances of non-union, and improve functional outcomes [1]. The choice of anesthesia for clavicle surgeries is limited to either general anesthesia (GA) or regional anesthesia (RA) in the form of Interscalene Brachial plexus block (ISBPB) and, more recently, the clavipectoral fascial plane block (CPB) as described by Valdez [2]. Both blocks often require supplementation with an intermediate cervical plexus block (ICPB) for optimal use.
The CPB has gained interest as an RA, as it offers an additional advantage of post-operative analgesia after surgery. It consists of a local anesthetic injection under the clavipectoral fascia in the region of the supraclavicular nerve that covers the clavicle, shoulder, and superior region of the chest. CPB provides pain relief through blocking of sensory nerve branches within the clavipectoral fascia and clavicle plane. The CPB can avoid the possible adverse events associated with an interscalene block, such as ipsilateral phrenic nerve palsy, vocal cord paralysis, vertebral artery injection, total spinal anesthesia, and pneumothorax [3,4]. CPB has also been reported to provide a better pulmonary function in the postoperative period and also circumvent the need for mechanical ventilation, especially in cases of pneumothorax and rib fractures [4,5,6]. This technique has gained importance in recent years for the management of clavicle fractures. Some authors have also reported using it for the removal of clavicle plates, as well as providing post-operative analgesia for patients undergoing surgery with clavicular fractures [7,8]. Being a newer modality, there are very few studies that have explored the use of CPB for the fixation of clavicle fractures, with most reports being limited to case reports or case series. To the best of our knowledge, no study has assessed prospectively the impact of this block on the functional outcomes of patients with clavicle fractures. This study aimed to assess the functional and radiological outcomes as well as the efficacy of pain management in patients with clavicle fractures undergoing fixation with CPB.
This single-arm prospective cohort study was conducted at a Tertiary care hospital from November 2022 to July 2024 after obtaining approval from the Institutional Ethics Committee (HIMSR/IEC/0065/2022). The manuscript follows the STROBE checklist for cohort studies. The sample size was calculated to be 30 based on a study by Wolf et al. The sample size was calculated based on the proportion of subjects with non-unions (pn = 6.7%) with alpha (α = 1.96) and power of 80% [9]. Based on the above, the sample size was calculated to be 97, on the basis of hospital data, the maximum possible number available was expected to be 40, so applying the finite population correction, the sample size was calculated to be 30. All consenting patients aged between 18 and 65 years with displaced clavicle fractures planned for fixation were assessed for inclusion in the study. The inclusion and exclusion criteria are given in Fig. 1.
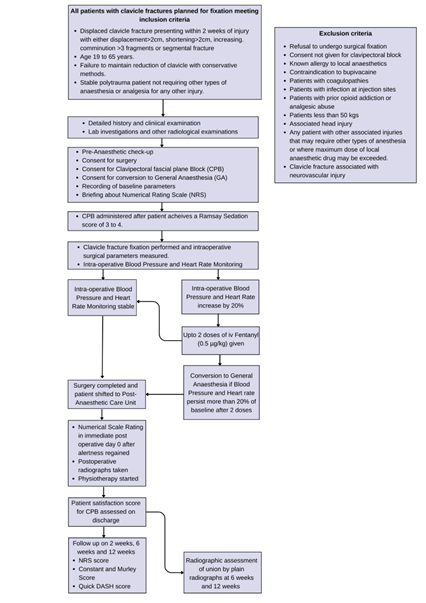
Figure 1: Flow chart of the study protocol.
All eligible patients underwent a detailed physical examination, and appropriate blood and radiological investigations were ordered. After obtaining pre-anesthetic clearance, the consent was obtained, and the surgery was planned. Consent for surgery, CPB, and conversion to GA was taken from the patient. Baseline parameters were recorded for heart rate (HR), blood pressure (BP), and the patient was briefed about the numerical scale rating for pain scoring before surgery.
Clavipectoral fascial block technique
The CPB block was performed after the patient was shifted to the operating table. The patient was positioned supine on the table under standard monitoring, and intravenous (IV) access was secured by two 20-G cannulas. Injection propofol (bolus 1 mg/kg bolus followed by infusion 25–75 µm/kg/min) to maintain a Ramsay sedation score of 3–4 throughout the surgery was administered. Under aseptic precautions, an ultrasound-guided CPB was administered after achieving a Ramsay sedation score of 4. An ultrasound linear probe (7–15 MhZ) was placed on the anterior border of the medial third of the clavicle. Using an “in plane approach,” a 22-gauge spinal needle with a three-way extension was inserted in a caudal to cephalic direction, visualizing the periosteum of the clavicle and surrounding fascia. A drug solution of 10 mL of 0.25% bupivacaine was injected between these layers. In addition, the 10 mL of the bupivacaine solution was injected at the fracture site. An additional 5 mL of bupivacaine solution was injected 5 cm medial and lateral to the fracture, totalling 30 mL solution, not exceeding 2.5 mg/kg. Sensory loss at the incision site was verified using tooth forceps before surgery commenced. If necessary, up to 10 mL of 1% lignocaine was infiltrated locally at the incision site. In addition, all patients received 0.1 mg/kg of dexamethasone and 15 mg/kg of paracetamol (PCM) at the start of surgery. Once the effect of the CPB was confirmed, clavicle fixation was done by standard methods using plates with lag screws. Intraoperative monitoring was done, and additional IV Fentanyl (0.5 µg/kg) was administered if HR or BP increased by 20% from baseline during surgery. Conversion to GA was done if pain and discomfort persisted despite 2 doses of IV Fentanyl. Post-surgery, patients were transferred to the post-anesthetic care unit (PACU), where they were monitored according to standard PACU protocols. All post-operative parameters were recorded by the investigator. The modified Observer’s Assessment of Alertness/Sedation (MOASS) was used to assess sedation at 5-min intervals. Once patients achieved a MOASS score of 5 (responsive to their name spoken in a normal tone/awake), they were evaluated using the 11-point NRS for pain. All patients received 1 g of PCM orally 3 times a day during the post-operative period, with the first dose scheduled 8 h after the intraoperative dose. An additional 100 mg of tramadol orally was administered on demand or if the NRS score reached 4 or higher. Cervical block was not administered as part of the protocol.
Post-operative protocol
In the postoperative period, an elbow pouch sling was given for support, and passive-assisted shoulder external rotation was started 24 h after surgery. Assisted shoulder abduction started at 2 weeks, and active shoulder movements, including 90° abduction and forward flexion, started at 6 weeks. Wound dressing was done 72 h after surgery, and suture removal was done after 2 weeks. Radiographs (Chest AP and Zanca Views) were taken immediately postoperative to evaluate the alignment of fracture fragments. These were then repeated at 6 and 12 weeks. Patient satisfaction scores regarding choice of anesthesia were measured on a Likert scale of 1–5 at the time of discharge. Functional outcomes were assessed using the Constant and Murley score and the quick disabilities of the arm, shoulder, and hand (QuickDASH) score [10,11]. Pain was measured using the NRS score [12]. The assessment was done 2 weeks, 6 weeks, and 12 weeks postoperatively. A flowchart of the study protocol is shown in Fig. 1.
Statistical analysis
Each entry was anonymised, and the data were coded and recorded in Microsoft Excel 2019. Statistical analysis was performed using Statistical Package for the Social Sciences version 23. Normality of continuous variables at each follow‑up time point was assessed using the Shapiro–Wilk test. Continuous variables that followed a normal distribution were expressed as mean ± standard deviation, while non‑normally distributed variables were summarised using median and interquartile range. Categorical variables were described using frequencies and percentages. Changes in continuous outcome variables over time within the same cohort were analysed using repeated‑measures analysis of variance (RM-ANOVA) for normally distributed data. For non‑normally distributed data, comparisons across time points were performed using the Friedman test. Where statistically significant differences were observed, post hoc pairwise comparisons were conducted using Bonferroni‑adjusted tests. A P < 0.05 was considered statistically significant.
A total of 37 patients were included in the study, but 7 were lost to follow-up, and a total of 30 participants were included in this study. The mean age of the study group was 38.67 ± 10.69 years. 80% of participants were males (n = 24). The most frequently operated fracture type was Allman type 2 (66.7%, n = 20). 56.6% (n = 17) of participants underwent open reduction and internal fixation using clavicle plates. Other participants underwent either fixation by a hook plate or fixation with a lag screw and clavicle plate. Demographic details of the study participants are given in Table 1.
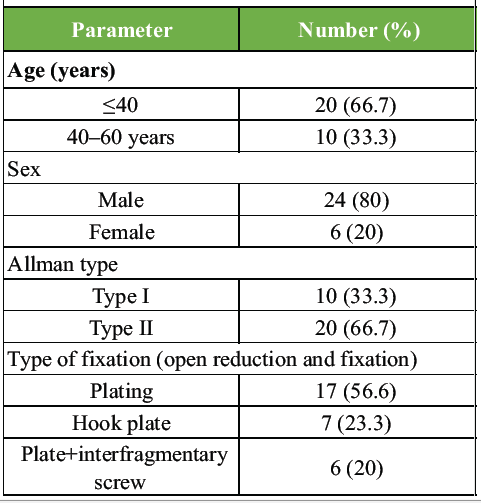
Table 1: Demographic parameters of the study
The mean distance of fractures from the lateral end of the clavicle was 7.34 ± 1.48 cm (Range = 4.8–10.0 cm). The mean incision distance from the lateral end of the clavicle was 3.07 ± 0.87 cm (Range = 1.6–5.0 cm). 90% of the participants (n = 27) did not experience an increase in BP or PR of >20%. Three participants required the use of IV Fentanyl during surgery and conversion to GA. The average intraoperative movements were 8.96 ± 3.60 (range = 4.0–19.0). Rescue analgesia was administered to 30% (n = 9) patients (Table 2).
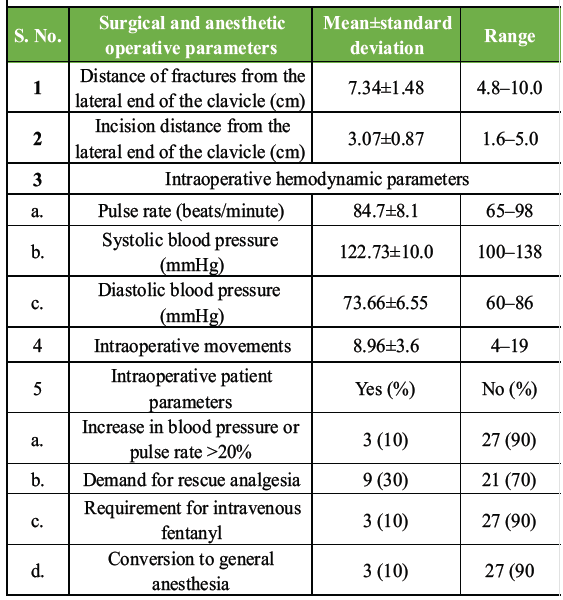
Table 2: Surgical and anesthetic parameters recorded in the study
The mean NRS score on post-operative day 0 (POD-0) was 3.53 ± 1.69. This decreased to 2.06 ± 0.90 at 2 weeks, 1.48 ± 0.63 at 6 weeks, and 1.24 ± 0.51 at 12 weeks (Table 3).
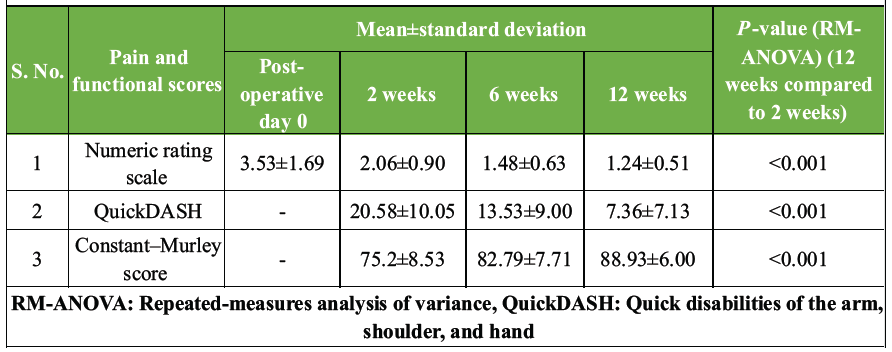
Table 3: Pain and functional scores recorded in the study
The RM-ANOVA test indicated a highly significant P < 0.0001, suggesting significant differences in NRS scores across different time points. In addition, pairwise comparisons against POD-0 also yielded P < 0.0001 at each subsequent time interval, indicating statistically significant reductions in pain scores compared to baseline throughout the follow-up period. At 2 weeks post-procedure, the mean QuickDASH score was 20.58 ± 10.05. It decreased to 13.53 ± 9.00 at 6 weeks and to 7.36 ± 7.13 at 12 weeks. The RM-ANOVA test revealed a highly significant P < 0.0001, indicating significant differences in QuickDASH scores across each follow-up (Table 3). The mean constant–Murley score was 75.72 ± 8.53 at 2 weeks post-procedure. It increased to 82.79 ± 7.71 at 6 weeks, then to 88.93 ± 6.00 at 12 weeks. The RM-ANOVA test yielded a highly significant P < 0.0001, indicating significant differences in constant–Murley scores across the 3 time points (Table 3).
Fracture union was assessed at 6 weeks after surgery; 40% (n = 12) showed the appearance of callus formation with an acceptable fracture reduction. 56.7% (n = 17) showed an acceptable reduction but no callus formation. 3.3% (n = 1) showed a loss of reduction with the absence of callus formation. All fractures showed bridging callus by the end of 12 weeks. 73.3% (n = 22) of patients did not experience any complications related to the CPB, 10% (n = 3) had to be converted to GA during the surgical procedure. 6.7% (n = 2) had superficial infections and a painful shoulder after the procedure. One patient reported paresthesia along the surgical site (Fig. 2).
73.3% (n = 22) of patients reported a satisfaction level of 4, the interquartile range for the patient satisfaction was 0. 13.3% (n = 5) gave a rating of 5 for the procedure and type of anesthesia (Fig. 3).
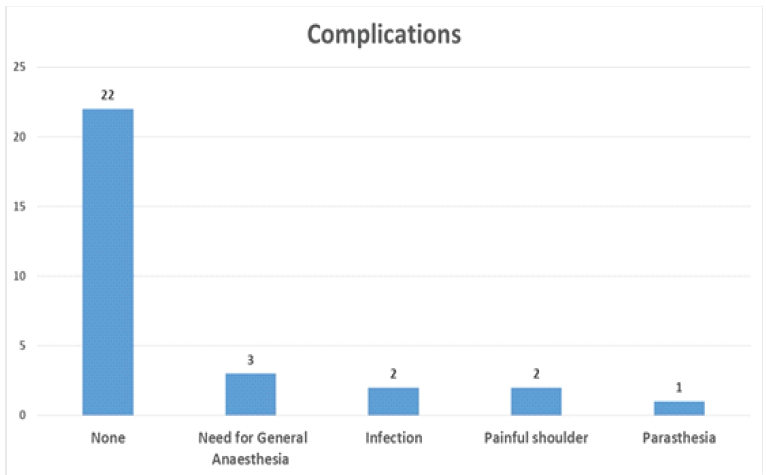
Figure 2: Complications reported during the study.
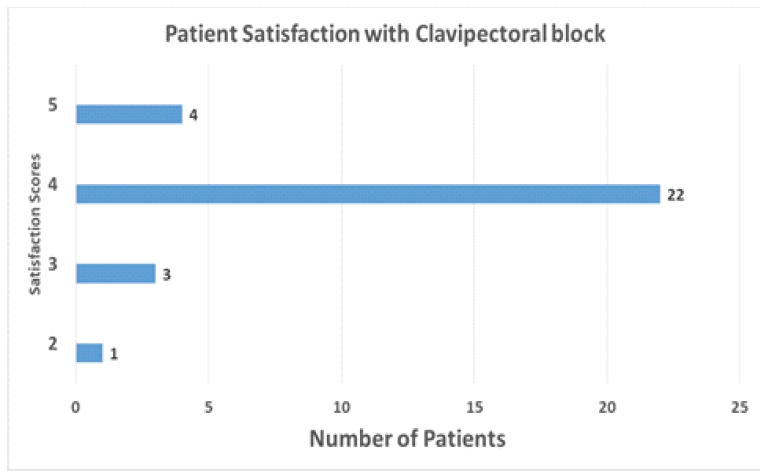
Figure 3: Patient satisfaction with the clavipectoral block.
This study is one of the few studies which has assessed the use of the CPB in the fixation of clavicle fractures. 73.3% patients reported a satisfaction score of 4, reflecting a good acceptability to the CPB, with only three patients having to be converted to GA. The NRS score, QuickDASH score, and Constant–Murley score all showed an improvement in each follow-up, and all fractures united by 12 weeks. The interpretation of these findings should be taken in an associative and not causative form. CPB may be associated with improved pain control and functional outcomes in addition to factors such as fracture stability after fixation and a well-structured rehabilitation protocol, since it allows for early initiation of rehabilitation.
The demographic characteristics of this study showed a male predominance and an average of 38.67 ± 10.69 years, which were similar to studies by Kihlström et al. and Yan et al. [13,14]. Allman type II fractures (66.7%) were more common than type I (33.3%) in this study, which were similar to the results reported by Robinso and Zhuo et al. [5,15].
Analgesia effectiveness
The effectiveness of analgesia by CPB in this study was evidenced by stable hemodynamics in 90% of cases and limited need for supplemental fentanyl (10%). This compares favorably with other regional anesthetic techniques. Zuho et al. reported stable hemodynamics for patients undergoing surgery under CPB as well as ISBPB with no difference between the two groups [5]. Rosales and Aypa reported excellent anesthesia with CPB lasting up to 16 h [3]. The average NRS score at the end of 24 h (POD-0) was 3.53 ± 1.69 for this study. Xu et al. reported a similar Visual Analog Scale (VAS) score of 4 (2–4) after 24 h in the CPB group and anesthesia duration of 20 ± 5.8 h. Labandeyra et al. reported a lower VAS score of 0.96 ± 1.29 at the end of 24 h [16].
Functional outcomes and fracture union
There was a progressive improvement in functional outcomes on each follow-up. QuickDASH scores decreased from 20.6 to 7.4 at final follow-up. The Constant–Murley scores increased from 75.7 to 88.9 over 12 weeks. Kukreja et al. reported similar improvements in functional scores following surgical fixation with RA [17]. However, this study showed slightly better early functional recovery, possibly attributed to the effective pain control provided by CPB. This study reported 100% union rate at 12 weeks, which compares favourably with previous studies. Meta-analyses by Zhang et al. reported union rates ranging from 92% to 97% for surgically managed clavicle fractures [18]. Fracture union is not related to the anesthesia technique however, a higher rate of union in this study may be attributed to the combination of stable fixation, effective post-operative pain control and a structured rehabilitation protocol enabling early mobilization.
Safety and satisfaction profile
ISBPB can cause diaphragm and upper arm paralysis. The advantages of a CPB include decreased incidence of post-operative diaphragm palsy, upper arm palsy, decreased rates of post-operative nausea and vomiting, decreased use of opioid based analgesia, fewer respiratory complications, and improved pain scores [19,20]. The CPB does not carry the risk of pneumothorax, and the overall complication rate of this study was 26.7%, which is similar to that reported by Mishra et al. [21]. This study showed lower rates of major complications, with most being minor and self-limiting. The infection rate (6.7%) was comparable to previously reported rates of 4.4–7.8% in similar studies [15,18,22]. Asadollahi et al. reported overall complication rates of 24–36% in clavicle fracture surgery [22,23]. Zhuo et al. in their study reported that ultrasound-guided CPB with intermediate cervical block significantly reduced hemi-diaphragmatic paralysis while providing adequate anesthesia [5]. Xu et al. reported 3 cases of Horner’s syndrome in patients administered superficial cervical plexus block (SCPB) combined with ISBPB and none in patients administered SCPB and CPB [24]. Labanderya et al. reported no conversion to GA, no neurological blockade of the upper limb or hemidiphragmatic paralysis [16]. The reported results indicate that the block is a relatively safer block to administer and also carries minimal complications.
In this study, 86.6% patients reported a high satisfaction score following surgery, which exceeded those reported in some previous studies, with an interquartile range of 0. Morrison et al. reported satisfaction rates of 75–80% with traditional anesthetic approaches. The higher satisfaction in this study might be attributed to the combination of effective pain control and early functional recovery facilitated by CPB.
The CPB has been shown to spread to the deltoid, pectoralis major, sternocleidomastoid, trapezius muscle, and the anterosuperior margin of the clavicular periosteal plane [16]. Considering this distribution, preparing for the rescue analgesia will make the surgery more comfortable for the patient, surgeon, and anesthetist in the event of a failed or inadequate block. The need for rescue analgesia in 30% of patients in this study suggests room for improvement in the technique. Recent studies by Zhang et al. and Asadollahi et al. have explored adjuvant medications and modified techniques to prolong analgesia duration, reporting lower rescue analgesia requirements of 15–20% [18,22,23]. Xu et al. reported a longer duration, lesser complications and better 24 h VAS score when combining intermediate cervical plexus with a superficial cervical block compared to an interscalene brachial block [24].
Learning curve and surgeon anesthetist co-ordination
The learning curve for this block is relatively short, making it easier to learn, administer, and teach [25]. The coordination between the surgeon and anesthetist also becomes important as the patient is relatively aware during the procedure. Both should communicate well with each other to ensure that the patient is comfortable during the procedure. A detailed discussion of both the surgical and anesthesia team among themselves and with the patient is essential before proceeding with the block and surgery. It may better prepare both for the procedure, especially the patient and may make them more cooperative. Pre-incision verification of the effectiveness of the block and effectively identifying and managing changes also requires good surgeon anesthetist coordination. In this study, a conversion rate to GA may also indicate good surgeon anesthetist coordination during the surgery.
Drawbacks
The drawbacks of this study were that it was a single-center study with an absence of a control group. A small sample size and relatively short follow-up duration were also considerable drawbacks. No objective assessment of diaphragm excursion was performed; a bedside pulmonary function test would also have improved the reporting the efficacy of this method for fixation of clavicle fractures. Observer bias during patient satisfaction reporting may have occurred.
CPB provides significant improvements in pain control in the intraoperative and postoperative period. It provides stable intraoperative hemodynamic conditions for surgery with a low need for conversion to GA or rescue analgesia. This, along with a high patient satisfaction and good radiological and functional outcomes, suggests that CPB is an acceptable method of RA for use in the fixation of clavicle fractures. CPB may have the potential to optimize perioperative care and contribute to better overall patient outcomes. More studies with control groups and longer follow-up are required before integrating CPB into clinical practice.
The clavipectoral fascial block is an effective and acceptable method for the surgical fixation of clavicle fractures.
References
- 1. Khan LK, Bradnock TJ, Scott C, Robinson CM. Fractures of the clavicle. J Bone Joint Surg Am 2009;91:447-60. [Google Scholar] [PubMed]
- 2. L. Valdés-Vilches. Part of Lecture: Analgesia for Clavicular Surgery/Fractures. Lugano, Switzerland: 36th Annual ESRA Congress; 2017. [Google Scholar] [PubMed]
- 3. Rosales AL, Aypa NS. Clavipectoral plane block as a sole anesthetic technique for clavicle surgery-A case report. Anesth Pain Med 2022;17:93-7. [Google Scholar] [PubMed]
- 4. Pereira CS, Ferros C, Dinis I, Pereira D, Miguel D, Vico M. Clavipectoral fascial plane block for clavicle fracture surgery: A case report. J Perioper Pract 2024;34:375-7. [Google Scholar] [PubMed]
- 5. Zhuo Q, Zheng Y, Hu Z, Xiong J, Wu Y, Zheng Y, et al. Ultrasound-guided clavipectoral fascial plane block with intermediate cervical plexus block for midshaft clavicular surgery: A prospective randomized controlled trial. Anesth Analg 2022;135:633-40. [Google Scholar] [PubMed]
- 6. Yadav A, Sharma RP, Magar KT, Joshi AD. Ultrasound-guided clavipectoral fascial plane block for clavicle surgery: A case report. Nepal Med J 2023;6:57-9. [Google Scholar] [PubMed]
- 7. Gonçalves D, Sousa CP, Graça R, Miguelez MP, Sampaio C. Clavipectoral fascia plane block combined with superficial cervical plexus block for the removal of osteosynthesis material from clavicle fracture. Cureus 2023;15:e43146. [Google Scholar] [PubMed]
- 8. Sabaa MA, Elbadry AA, El Malla DA. Ultrasound-guided clavipectoral block for postoperative analgesia of clavicular surgery: A prospective randomized trial. Anesth Pain Med 2022;12:e121267. [Google Scholar] [PubMed]
- 9. Wolf S, Chitnis AS, Manoranjith A, Vanderkarr M, Plaza JQ, Gador LV, et al. Surgical treatment, complications, reoperations, and healthcare costs among patients with clavicle fracture in England. BMC Musculoskelet Disord 2022;23:135. [Google Scholar] [PubMed]
- 10. Constant CR, Murley AH. A clinical method of functional assessment of the shoulder. Clin Orthop Relat Res 1987;214:160-4. [Google Scholar] [PubMed]
- 11. Beaton DE, Wright JG, Katz JN, Upper Extremity Collaborative Group. Development of the QuickDASH: Comparison of three item-reduction approaches. J Bone Joint Surg Am 2005;87:1038-46. [Google Scholar] [PubMed]
- 12. Jensen MP, Karoly P, Braver S. The measurement of clinical pain intensity: A comparison of six methods. Pain 1986;27:117-26. [Google Scholar] [PubMed]
- 13. Kihlström C, Möller M, Lönn K, Wolf O. Clavicle fractures: Epidemiology, classification and treatment of 2 422 fractures in the Swedish fracture register; an observational study. BMC Musculoskelet Disord 2017;18:1-9. [Google Scholar] [PubMed]
- 14. Yan MZ, Yuen WS, Yeung SC, Wing-Yin CW, Wong SC, Si-Qi WW, et al. Operative management of midshaft clavicle fractures demonstrates better long-term outcomes: A systematic review and meta-analysis of randomised controlled trials. PloS One 2022;17:e0267861. [Google Scholar] [PubMed]
- 15. Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br 1998;80:476-84. [Google Scholar] [PubMed]
- 16. Labandeyra H, Heredia C, Váldes-Vilches LF, Prats-Galino A, Sala-Blanch X. Clavipectoral fascia plane block in midshaft clavicle fractures: A cadaveric study. J Clin Anesth 2024;96:111469. [Google Scholar] [PubMed]
- 17. Kukreja P, Davis CJ, MacBeth L, Feinstein J, Kalagara H. Ultrasound-guided clavipectoral fascial plane block for surgery involving the clavicle: A case series. Cureus 2020;12:e9072. [Google Scholar] [PubMed]
- 18. Zhang C, Huang J, Luo Y, Sun H. Comparison of the efficacy of a distal clavicular locking plate versus a clavicular hook plate in the treatment of unstable distal clavicle fractures and a systematic literature review. Int Orthop 2014;38:1461-8. [Google Scholar] [PubMed]
- 19. Merella F, Mossetti V. Ultrasound-guided upper and lower extremity nerve blocks in children. BJA Educ 2020;20:42-50. [Google Scholar] [PubMed]
- 20. Tsuji T, Takeuchi S, Tsuji R, Nakano H. Ultrasound-guided clavipectoral fascial plane block combined with intermediate cervical plexus block for surgery on a displaced midshaft clavicular fracture in an adolescent athlete: A case report. Cureus 2024;16:e64504. [Google Scholar] [PubMed]
- 21. Mishra A, Kumar D, Yadav A, Pandey D, Sinha AK. Functional outcome of conservative versus plate osteosynthesis in displaced midshaft clavicle fracture in manual labours. Int J Surg 2017;4:966-70. [Google Scholar] [PubMed]
- 22. Asadollahi S, Hau RC, Page RS, Richardson M, Edwards ER. Complications associated with operative fixation of acute midshaft clavicle fractures. Injury 2016;47:1248-52. [Google Scholar] [PubMed]
- 23. Asadollahi S, Bucknill A. Acute medial clavicle fracture in adults: A systematic review of demographics, clinical features and treatment outcomes in 220 patients. J Orthop Traumatol 2019;20:24. [Google Scholar] [PubMed]
- 24. Xu G, Su P, Cai B, Liu Y, Jiang D, He Y, et al. Ultrasound-guided superficial cervical plexus block combined with clavipectoral fascial plane block or interscalene brachial plexus block in clavicle surgery: A single-centre, double-blind, randomized controlled trial. J Clin Monit Comput 2023;37:985-92. [Google Scholar] [PubMed]
- 25. Sonawane K, Dharmapuri S, Saxena S, Mistry T, Balavenkatasubramanian J, Balavenkatasubramanian J. Awake single-stage bilateral clavicle surgeries under bilateral clavipectoral fascial plane blocks: A case report and review of literature. Cureus. 2021;13:e20537. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Isolated Calcific Deposition in the Subacromial Bursa: A Rare Case Report and Arthroscopic Management
August 1, 2026 Isolated Calcific Deposition in the Subacromial Bursa: A Rare Case Report and Arthroscopic Management May 1, 2026 Spontaneous Remodeling of Posterior Sternoclavicular Joint Dislocations in Skeletally Immature Patients: A Case Report
May 1, 2026 Spontaneous Remodeling of Posterior Sternoclavicular Joint Dislocations in Skeletally Immature Patients: A Case Report May 1, 2026 A Rare Occurrence of Chronic Recurrent Multifocal Osteomyelitis in Clavicle: Case Report
May 1, 2026 A Rare Occurrence of Chronic Recurrent Multifocal Osteomyelitis in Clavicle: Case Report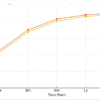 April 1, 2026 Mid-term Functional Outcomes Following One-stage Single-Sitting Bilateral and Unilateral Unicompartmental Knee Arthroplasty: A 5-year Prospective Cohort Study
April 1, 2026 Mid-term Functional Outcomes Following One-stage Single-Sitting Bilateral and Unilateral Unicompartmental Knee Arthroplasty: A 5-year Prospective Cohort Study