
While survival in metastatic spinal disease, including cord compression, is largely dictated by tumour biology, surgical intervention remains integral to multidisciplinary care, providing meaningful improvements in pain and health-related quality of life.
Dr. Archisha Marya, Manchester University Hospitals Foundation Trust, Manchester, United Kingdom. E-mail: archisha.marya@mft.nhs.uk
Abstract
Introduction: Metastatic spinal disease, including cord compression, represents a significant complication of advanced malignancy and is associated with pain, neurological deficit, and reduced quality of life. Surgical intervention continues to play a vital role in management for selected patients. Survivorship following surgery varies widely and is influenced by tumour biology and systemic disease burden. The aim of the study is to evaluate survival and functional outcomes in patients surgically treated for metastatic spinal disease, including cord compression, by a single surgeon at a UK tertiary spinal centre.
Materials and Methods: Retrospective case series of prospectively collected data from 45 patients undergoing surgery for metastatic spinal disease, including cord compression. Data included demographics, tumour histology, Bilsky grade, spinal instability neoplastic score (SINS), neurological status, surgical procedure, complications, survival, and functional outcomes (Visual Analogue Scale [VAS], EuroQol-5 dimension [EQ-5D], and Oswestry disability index [ODI]). Paired pre- and post-operative comparisons were performed using appropriate statistical tests (paired t-test or Wilcoxon), and survival analysis was conducted using Kaplan–Meier and Cox regression.
Results: The mean patient age was 61.7 ± 12.9 years (range 23.9–81.3 years), with 51% female predominance. The most common primary tumours were lung (20%), breast (17.8%), myeloma (15.6%), and renal cell carcinoma (13.3%). High-grade epidural spinal cord compression (Bilsky 2–3) was present in 60%. At presentation, 65% had no neurological deficit, 19% had radicular symptoms, and 14% had incomplete spinal cord injury. Most patients had intermediate SINS scores (66%), while 34% were classified as unstable. Decompression with stabilisation was most frequent (67%), followed by debulking (20%) and complex/reconstructive procedures (13%). Post-operative complications occurred in 11% (5/45), with no peri-operative deaths. In the subset with complete functional data (n = 28), mean VAS improved from 47.3 to 68.9 and EQ-5D index from 0.17 to 0.56 (P < 0.001). Median post-operative survival was 12 months, mean survival 31.4 months, and 30-day mortality 4.3%. Tumour histology was a significant predictor of survival (log-rank χ² = 14.4, P = 0.006), with myeloma and breast cancer patients showing the most favourable outcomes. Post-operative ODI category was also associated with survival (log-rank χ² = 12.2, P = 0.028).
Conclusion: Surgery for metastatic spinal disease including cord compression was associated with meaningful functional improvement and survival outcomes that are consistent with historical expectations. These findings support the continued role of surgical intervention as part of a multidisciplinary approach in appropriately selected patients with symptomatic disease.
Keywords: Spine, cord compression, metastases, surgery, functional outcomes, survivorship.
Metastatic spinal disease is a serious complication of malignancy, affecting approximately 5–10% of cancer patients during their illness [1]. It is considered an oncological emergency because untreated compression can lead to irreversible motor deficit, sensory loss, and sphincter dysfunction [2]. Metastatic spinal cord compression (MSCC) typically results from tumour invasion into the epidural space, compressing the spinal cord or cauda equina [3]. Timely recognition and management are therefore critical to preserving neurological function and quality of life. The epidemiological burden of metastatic spinal disease is substantial. Population-based data from South-East Norway reported an annual incidence of 26/100,000 for metastatic spinal disease requiring intervention and 8.1/100,000 for MSCC [4]. In that cohort, 31% of patients presented with established MSCC, and 11% were non-ambulatory at first assessment, highlighting the frequency of late or advanced presentation. Decompression and stabilisation, typically followed by radiotherapy, remain central to the management of selected patients with spinal metastases, particularly those with mechanical instability or progressive neurological decline [5]. Prognostic factors influencing treatment choice include tumour histology, systemic disease burden, functional status, and severity of neurological deficit [6]. Survival outcomes vary significantly depending on the biology of the primary tumour. For example, a large multicentre cohort study by Choi et al. showed that survival outcomes following surgery for metastatic spinal disease, including cord compression, are strongly determined by primary tumour biology and the extent of systemic disease [7]. Their prognostic model reinforces the value of individualised assessment when selecting patients for operative intervention. Despite advances in systemic therapy and radiotherapy techniques, metastatic spinal disease continues to present urgently with pain, instability, and neurological compromise. Surgery remains a critical part of multidisciplinary care, offering mechanical stabilisation and decompression in selected patients. However, contemporary UK data reporting survivorship and functional outcomes following surgery for metastatic spinal disease, including cord compression, remain limited. The aim of this study was to evaluate survival and functional outcomes following surgical treatment of metastatic spinal disease, including cord compression, in a single-surgeon cohort at a UK tertiary centre.
Aims:
The aim of the study is to evaluate survivorship and functional outcomes in a cohort of patients who underwent surgical treatment for metastatic spinal disease, including cord compression, at a UK regional centre between 2018 and 2024.
We analysed a retrospective case series of prospectively collected data for patients who underwent surgical treatment for metastatic spinal disease, including cord compression, under a single surgeon at the Walton Centre, Liverpool, UK, between June 2018 and June 2024. No formal sample size calculation was performed, as this study represents a retrospective analysis of all consecutive eligible patients treated within the study period at a single tertiary center. The cohort size was therefore determined by case availability. The study was registered as a service evaluation with the institutional audit department. Ethical approval was not required under NHS Health Research Authority guidance, as the analysis adhered to anonymized routinely collected data. Data were collected from the spinal oncology referral database at Clatterbridge Cancer Centre. Demographic and clinical information included sex, age at presentation, primary tumor histology, neurological deficits, extent of spinal instability and compression, type of surgery, perioperative complications, pre- and post-operative functional outcomes, and survival. All variables were extracted from the British Spine Registry and cross-verified with EP2 electronic health records to ensure accuracy. Survival status was confirmed through electronic health records at the last follow-up. Statistical data were analyzed using IBM Statistical Package for the Social Sciences Statistics, Version 31.0.
Inclusion criteria:
- Age ≥18 years
- Radiological or histological confirmation of metastatic spinal disease
- Surgical intervention for metastatic spinal disease, including cases presenting with cord compression.
Exclusion criteria:
- Non-surgical management
- No confirmed metastatic spinal pathology.
Outcomes:
The primary outcome was overall survival following surgery, defined as the time from index surgery to death. Secondary outcomes included survival by tumor histology, survival by degree of cord compression (Bilsky grade), post-operative functional outcomes, and perioperative complications. Analyses used complete-case methods (EuroQol-5 dimension [EQ-5D]/Visual Analog Scale [VAS] n = 28; Oswestry disability index [ODI] n = 22). For each patient, the following variables were recorded: Age, sex, primary tumor type, spinal instability neoplastic score (SINS), epidural spinal cord compression (Bilsky) grade, neurological status at presentation, operative procedure, post-operative complications, pre- and post-operative functional outcomes (VAS; EQ-5D where available), ODI where available, and survival. Functional outcomes were evaluated using the EQ-5D questionnaire pre- and post-operatively. Health status was summarized as EQ-5D index values, where a score of 1 represented full health and 0 represented death. In addition, EQ VAS scores were collected to complement EQ-5D data, measuring patients’ self-reported health on a scale of 0–100, ranging from “worst health imaginable” to “best health possible.” Primary and secondary survival outcomes evaluated the event of interest, such as the death of a patient. Patients who did not experience the event of interest by the end of follow-up time were censored for the purpose of Kaplan–Meier analysis.
A total of 45 cases were included in the study. The distribution of primary tumour types is summarised in Table 1 and Fig. 1.
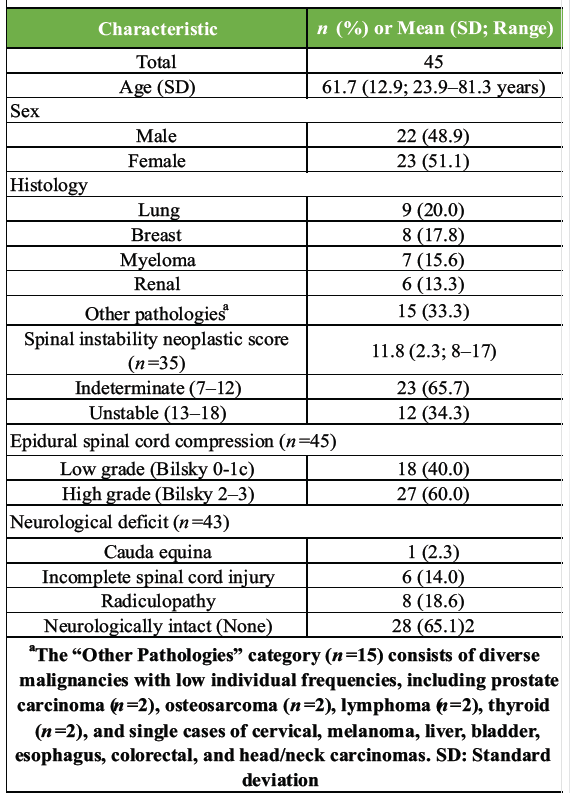
Table 1: Baseline patient demographics and clinical characteristics
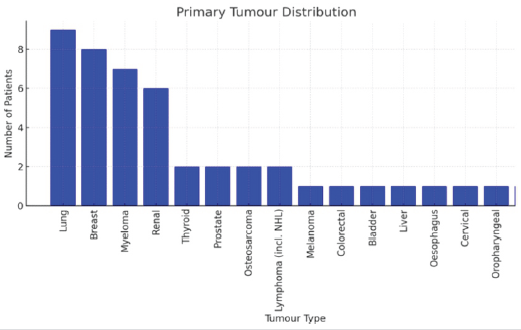
Figure 1: Malignancy frequency (n=45).
The median follow-up duration for the cohort was 12.0 months. The mean follow-up was 27.6 months, reflecting a positively skewed distribution due to a small number of long-term survivors extending up to 108 months post-operatively. Decompression with stabilisation was the most frequent procedure (67%), followed by debulking/extended decompression (20%) and complex/reconstructive procedures (13%). For analysis, procedures were categorised into three cohorts based on procedural complexity. The standard decompression/stabilisation group (n = 30) included patients who underwent decompression and stabilisation only. The debulking/extended decompression group (n = 9) included patients who underwent debulking or debridement in addition to decompression and stabilisation. The complex/reconstructive group (n = 6) included patients who underwent corpectomy, reconstruction/fusion, or vertebral body augmentation in addition to decompression and stabilisation. Pre-operative imaging using the Bilsky scale showed that 60% of patients (n = 27) had high-grade compression (Bilsky 2–3), while 40% (n = 18) had low-grade compression (Bilsky 0–1c) (Fig. 2).
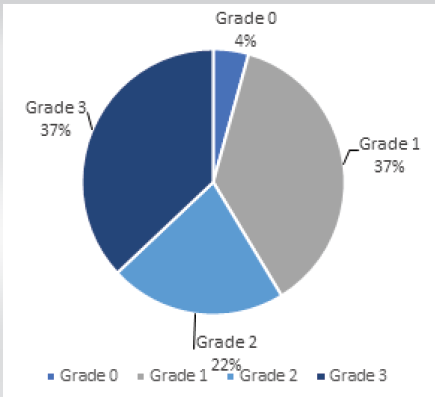
Figure 2: Bilsky grade (n=45).
Pre-operative neurological status was recorded for 43 patients (94%) (Fig. 3).
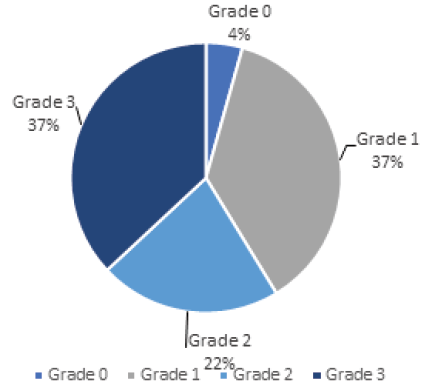
Figure 3: Neurological status at presentation (n=43).
Most patients (n = 28) presented without focal (motor or sensory) neurological deficits. Among those presenting with neurological compromise (n = 15), symptoms included radiculopathy (n = 8), incomplete spinal cord injury (American Spinal Injury Association C/D; n = 6) [8], and cauda equina syndrome (n = 1) [9]. Post-operative neurological outcomes were not consistently recorded. Spinal mechanical stability was assessed preoperatively using the SINS. All patients with available SINS data (n = 35) scored ≥7, showing that no patients had stable spines (SINS 0–6). Most patients (n = 23, 66%) had indeterminate instability (SINS 7–12), while the remaining 12 (34%) were classified as unstable (SINS 13–18). One intraoperative complication (significant bleeding) and five post-operative complications (11%; 5/45), including wound infection, pulmonary embolism, pseudo-ileus, dural tear, and late wound breakdown, were observed [10]. No in-hospital deaths occurred. The 30-day mortality rate was 4.3% (2/45). Overall survival analysis was evaluated as a primary baseline measure for all 45 patients. At the time of data cutoff, 27 deaths (58.7%) had occurred. Kaplan–Meier analysis revealed early post-operative mortality followed by a plateau of long-term survivors. The median overall post-operative survival was 12 months (95% confidence interval [CI]: 0.0–49.5), and the mean survival was 31.38 months. The 1-year overall survival rate was 50.5% (standard error [SE], 0.075), with estimated 2-year and 5-year survival rates of 48.1% (SE, 0.075) and 42.8% (SE, 0.076), respectively (Fig. 4).
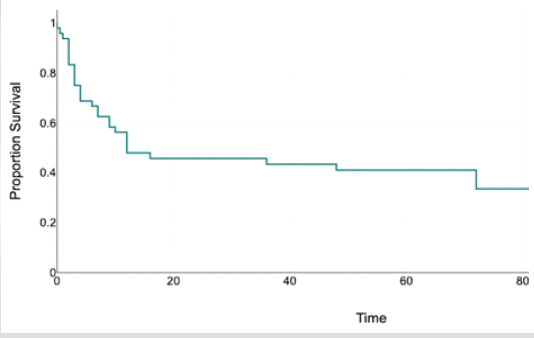
Figure 4: Overall survival curve (n=45).
Stratified by operative procedure, patients who underwent standard decompression and stabilisation (n = 30) showed the longest median survival of 48.0 months (95% CI: 0.0–99.5). The patients who underwent debulking or extended decompression (n = 9) had a median survival of 10.0 months (95% CI: 7.1–13.0). For patients who underwent complex/reconstructive surgery (n = 6), median survival was not reached (NR) at the time of data cutoff. Survival differences among the intervention groups were not statistically significant (Log-Rank χ² = 0.87; P = 0.646) (Fig. 5).
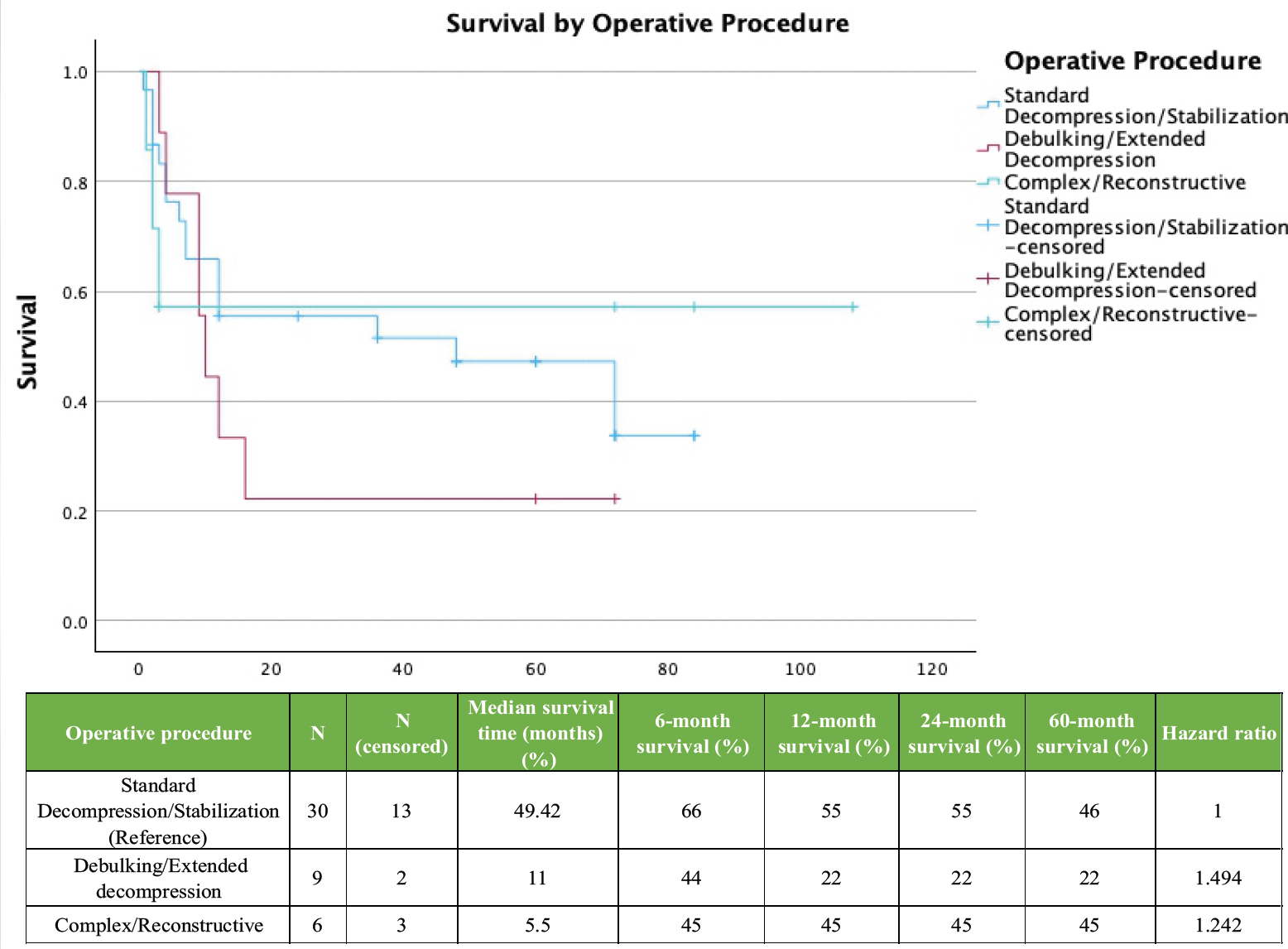
Figure 5: Kaplan–Meier plot of overall survival time (months) for patients stratified by operative (n=45)
Primary tumour histology was a significant predictor of survival (Log-Rank χ² = 14.4, P = 0.006), reflecting heterogeneity among cancer types. Patients with myeloma and breast cancer had the most favourable outcomes, with median survival NR in either group due to >50% of patients remaining alive at follow-up. Mean survival was longest for myeloma patients at 92.0 months (95% CI: 63.4–120.6) and 53.0 months (95% CI: 34.2–71.8) for breast cancer (Fig. 6).
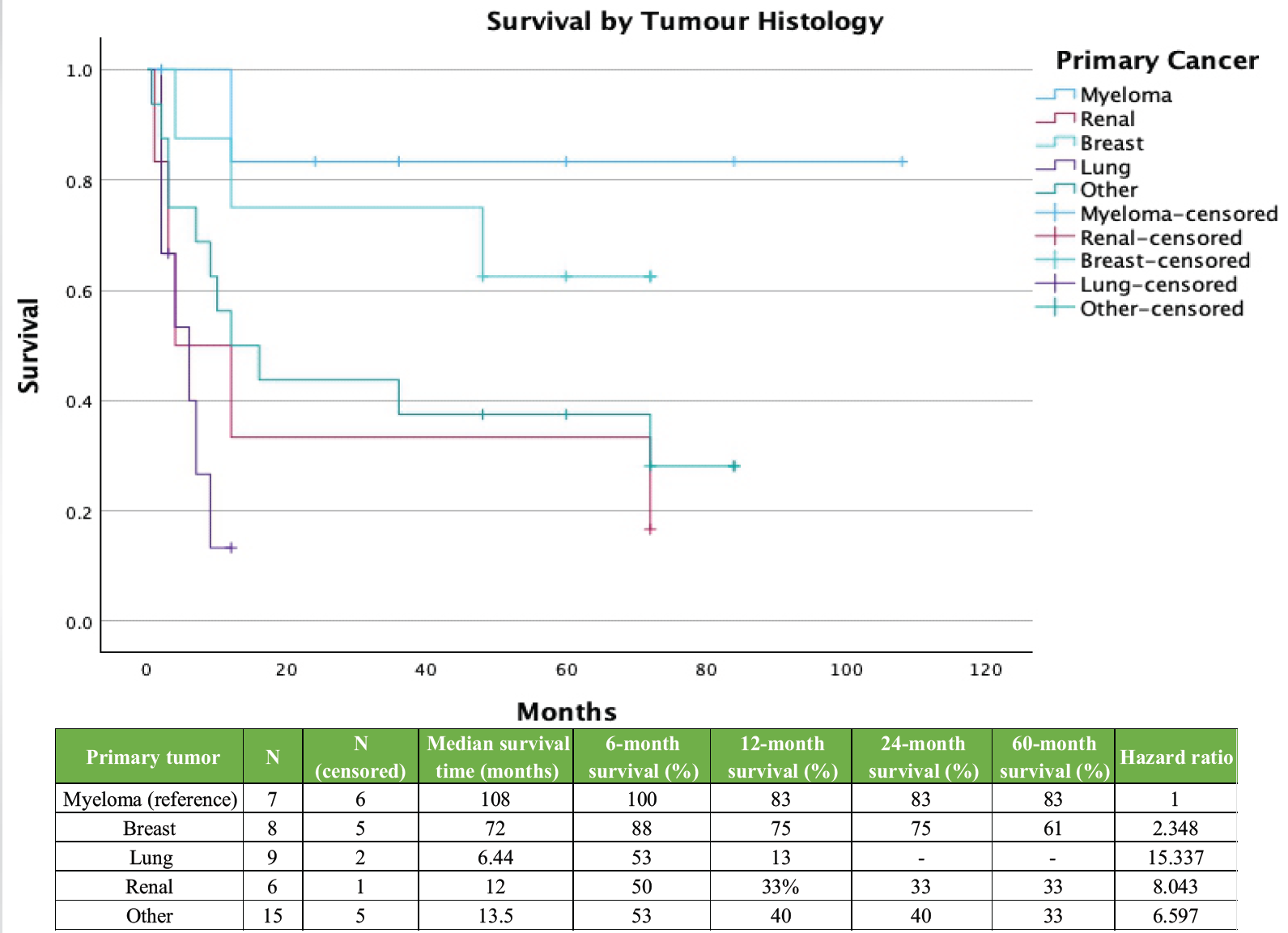
Figure 6: Survival by primary tumor histology (n=45).
In contrast, renal cell carcinoma and lung cancer patients experienced rapid post-operative decline, with median survival of 4.0 months (95% CI: 0.0–14.8) and 6.0 months (95% CI: 0.9–11.1), respectively. The “other pathologies” group (n = 15) showed an intermediate profile, with a median survival of 12.0 months (95% CI: 3.2–20.9). A multivariate Cox proportional hazards model assessing age, tumour histology, and operative procedure identified tumour histology as the only statistically significant predictor of post-operative survival (P = 0.030). Using myeloma as the reference, lung cancer patients had a significantly higher mortality hazard (hazard ratio [HR]: 16.0; 95% CI: 1.9–137.8; P = 0.012). Renal (HR: 8.4; 95% CI: 0.9–74.0; P = 0.056) and “other” histologies (HR: 7.0; 95% CI: 0.9–56.8; P = 0.056) trended toward increased hazard, while breast cancer did not differ significantly from myeloma (HR: 2.4; 95% CI: 0.2–23.0; P = 0.463). Extent of surgery, either extended debulking/decompression (HR: 0.9; 95% CI: 0.3–2.3; P = 0.776) or complex/reconstructive procedures (HR: 1.0; 95% CI: 0.2–4.0; P = 0.987), did not significantly impact survival nor did patient age (HR: 1.0; 95% CI: 0.9–1.0; P = 0.844). Kaplan–Meier analysis using the SINS assessed the impact of preoperative mechanical instability on survival (Fig. 7).
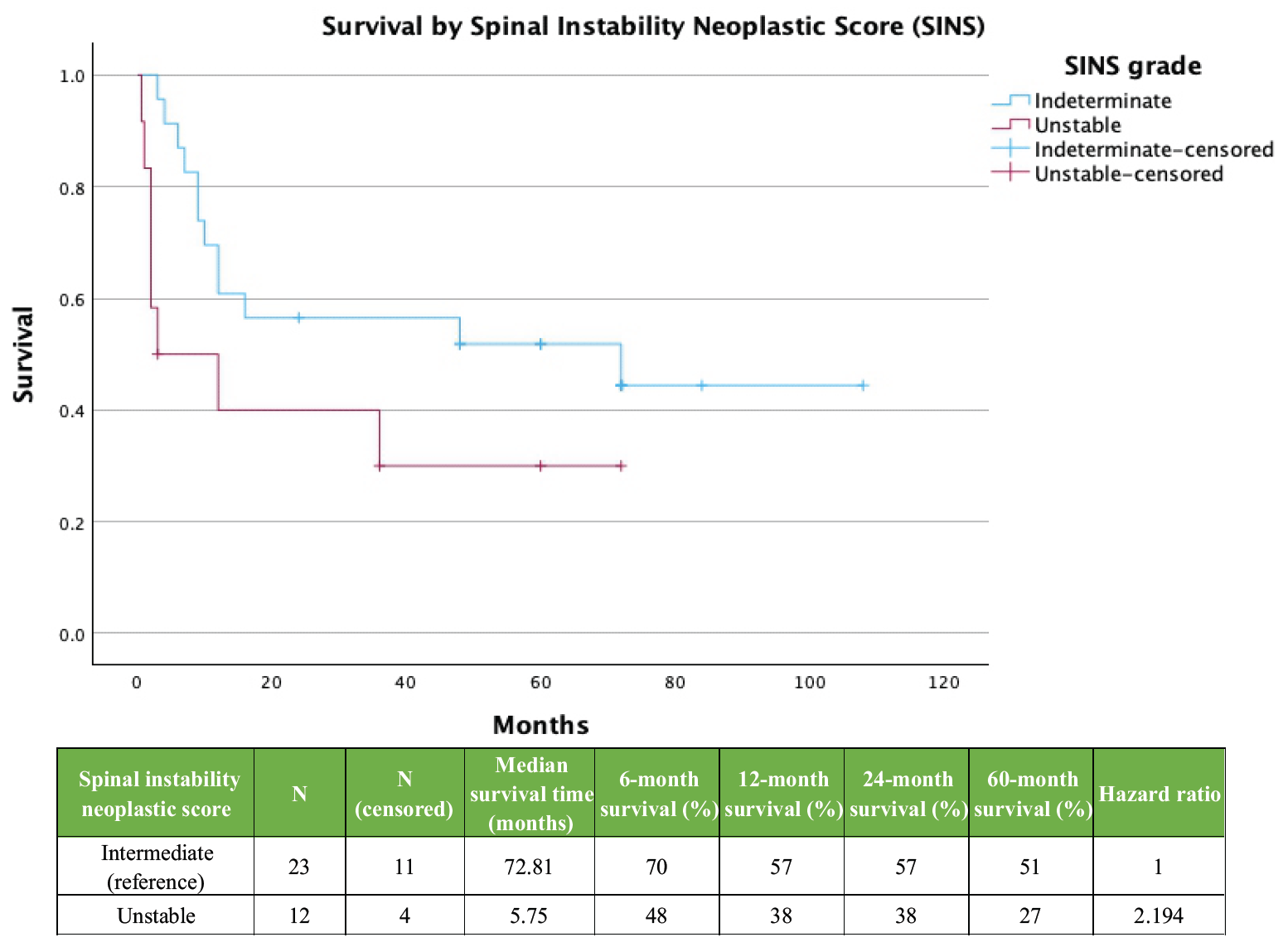
Figure 7: Kaplan–Meier survival plot by SINS (n=35).
Ten patients (22.2%) were excluded due to missing baseline data, leaving 35 cases for analysis. Patients were stratified into intermediate instability (SINS 7–12, n = 23) and unstable (SINS 13–18, n = 12). The unstable cohort showed a rapid decline in survival compared with the intermediate group, with a median survival of 3.0 months (95% CI: 0.0–18.4) versus 72.0 months (95% CI: 0.0–174.5). Despite this difference, the result did not reach statistical significance (Log-Rank χ² = 3.14; P = 0.076). To evaluate the prognostic effect of spinal cord compression, patients were stratified into low-grade (Bilsky 0–1c, n = 18) and high-grade (Bilsky 2–3, n = 27) groups. Kaplan–Meier analysis showed no statistically significant difference (Log-Rank χ² = 1.95; P = 0.162). Median survival was 72.0 months (NR) for low-grade compression and 12.0 months (95% CI: 9.6–14.4) for high-grade compression. Mean survival was 61.1 months (95% CI: 38.6–83.6) and 29.2 months (95% CI: 16.9–41.4), respectively (Fig. 8).
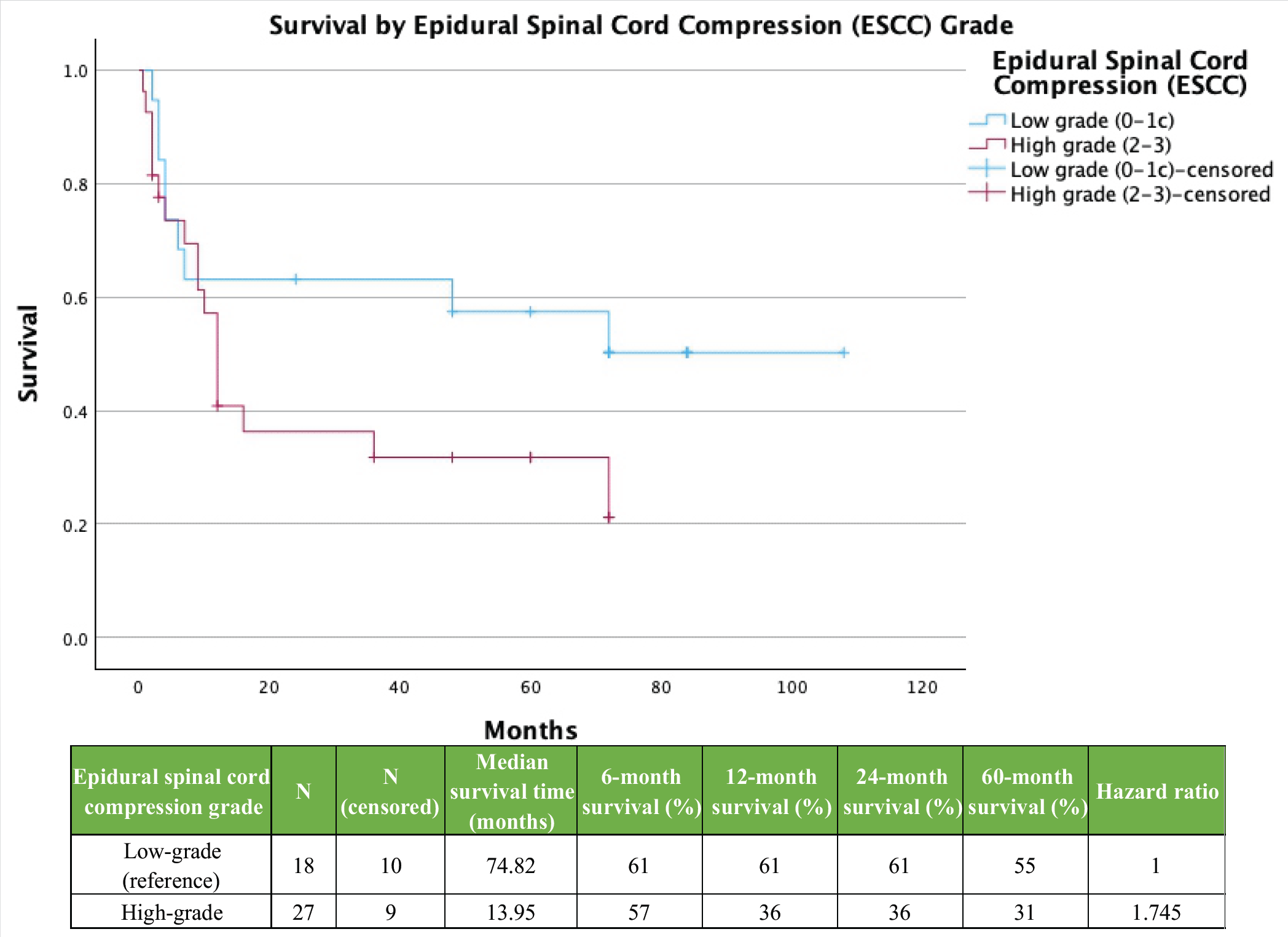
Figure 8: Survival by epidural spinal cord compression Grade (n=45).
Median survival NR to >50% of patients remaining alive at follow-up. A secondary bivariate Cox proportional hazards model assessed the combined impact of SINS and Bilsky grade on post-operative survival, with 35 patients included after listwise deletion of missing data. The model was not statistically significant (P = 0.064). Adjusted for SINS, high-grade compression showed a trend toward increased mortality (HR: 2.3; 95% CI: 0.8–6.3; P = 0.122). Adjusted for compression, unstable SINS was associated with a higher hazard (HR: 2.2; 95% CI: 0.9–5.5; P = 0.095). Wide CIs reflect reduced statistical power due to small sample size. Kaplan–Meier survival analyses are summarised in Table 2, with multivariate Cox proportional hazards results presented in Table 3.
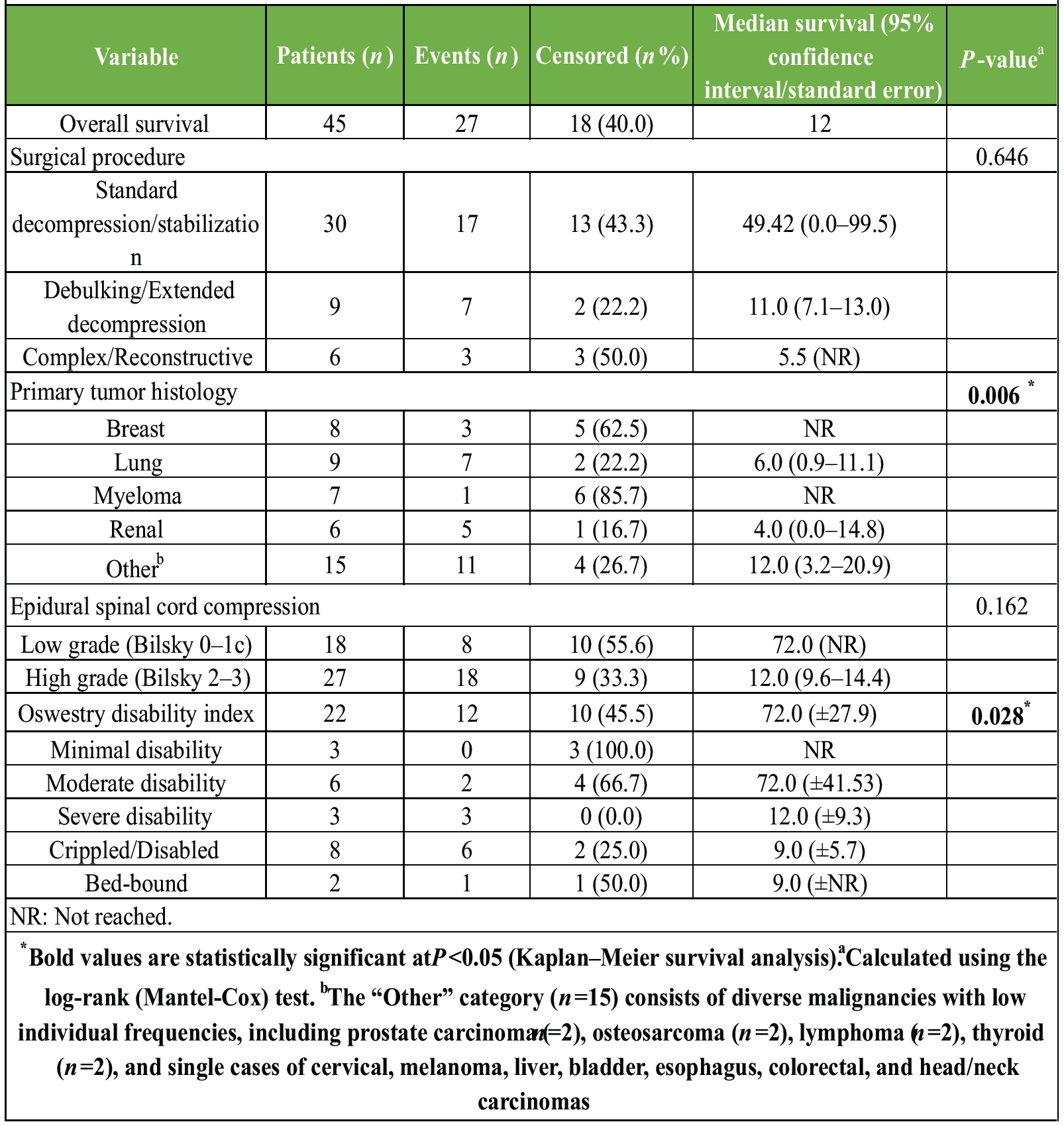
Table 2: Univariate Kaplan–Meier analysis of factors associated with survival
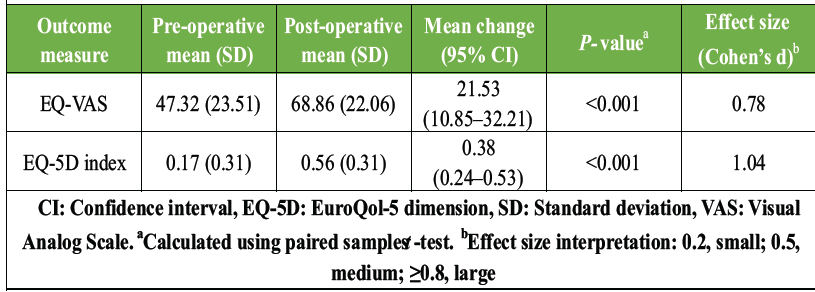
Table 3: Functional outcomes: (EQ-5D VAS) (n=28)
Functional outcomes were assessed using paired pre- and post-operative measures. EQ-5D data were available for 28 patients (61%). Surgical intervention led to significant improvements in both the EQ-5D index and VAS scores. The EQ-5D index increased from 0.17 (standard deviation [SD]: 0.32) pre-operatively to 0.56 (SD: 0.31) post-operatively, a mean improvement of 0.38 (95% CI: 0.24–0.53; P < 0.001), exceeding the minimal clinically important difference (Δ ≥ 0.10) (Table 3) [11]. Effect size analysis indicated a large treatment effect (Cohen’s d = 1.04). EuroQol-VAS scores rose from 47.32 (SD: 23.51) to 68.86 (SD: 22.06), a mean improvement of 21.53 points (95% CI: 10.85–32.21; P < 0.001), representing a medium-to-large clinical benefit (Cohen’s d = 0.78). ODI scores were available for 22 patients (48.9%) and were stratified into five categories of disability: minimal (0–20%, n = 3, 13.6%); moderate (21–40%, n = 6, 27.3%); severe (41–60%, n = 3, 13.6%); crippled (61–80%, n = 8, 36.4%); and bed-bound (81–100%, n = 2, 9.1%). Within this subgroup, 12 deaths occurred (54.5%), with 45.5% of patients censored at last follow-up. Kaplan-Meier analysis revealed a statistically significant difference in survival across ODI categories (Log-Rank χ² = 12.2; P = 0.028) (Fig. 9).
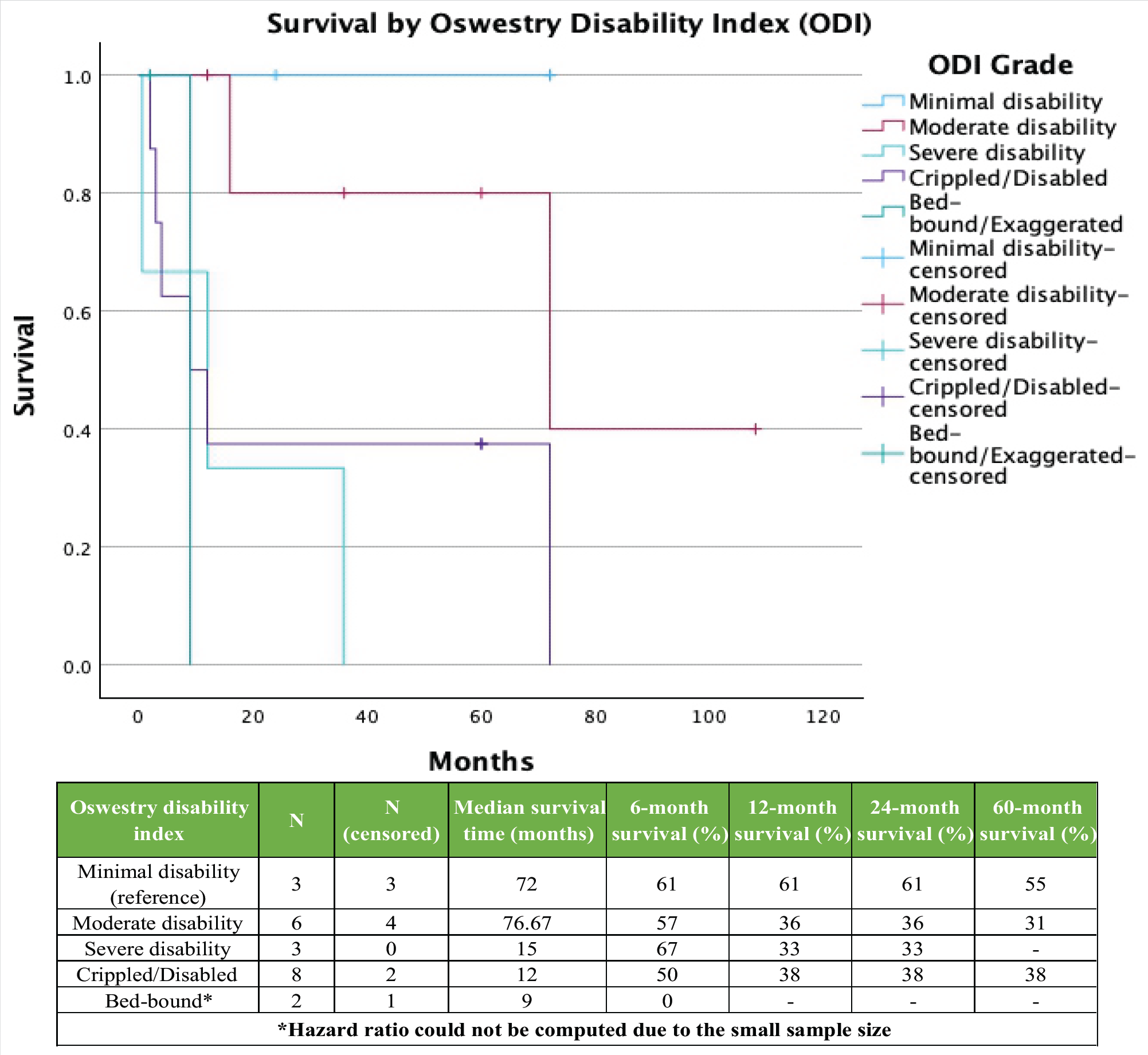
Figure 9: Survival by Oswestry disability Index (n=22).
Patients with minimal disability had no recorded deaths. The moderate disability group experienced 2 deaths (33% mortality) with a median survival of 72.0 months (SE: 41.5). The crippled group accounted for 5 deaths with a median survival of 9.0 months (SE: 5.7). Patients with severe disability (n = 3) had 100% mortality, with a median survival of 12.0 months (SE: 9.3). Bed-bound patients had a median survival of 9.0 months. The post-operative ODI category was significantly associated with survival, though causality cannot be inferred.
This contemporary UK single-surgeon series cohort demonstrates that surgical intervention for metastatic spinal disease, including cord compression, results in clinically meaningful improvements in health-related quality of life, with survival outcomes consistent with modern oncological practice. The median post-operative survival was 12 months (95% CI: 0–49.5), with a mean survival of 31.38 months and a 1-year overall survival rate of 50.5% in our cohort, which aligns with survival durations reported in older studies, where median survival ranged from 6 to 12 months [12,13]. It is, however, important to consider disparities between studies, including variation in oncological therapies, selection bias, and the demographics and systemic disease burden of included patients. The demographic characteristics of our cohort are consistent with those reported across multiple studies, including Lomas and Laba [13] and more recent analyses by Yaari et al. [14] and Zanaty and George [15]. However, unlike prostate-predominant series such as Bhanot et al. [16], our sample demographic was predominantly lung, breast, haematological, and renal malignancies. This tumour distribution is consistent with epidemiological patterns, as described by Cole and Patchell [1] and reinforced by guidelines from Loblaw and Laperriere [2]. Tumour histology emerged as the strongest predictor of postoperative survival in both univariate and multivariate analyses [6,7,12]. Patients with breast, thyroid, or haematological malignancies had comparatively prolonged survival, whereas lung, gastrointestinal, and oesophageal cancers were associated with poorer outcomes. These results highlight that tumour biology, rather than radiological severity alone, is the dominant determinant of survival and underscore the importance of integrating clinical and imaging parameters for individualised prognostication. Most patients in this series underwent decompression with stabilisation, an approach well supported by the foundational work of Klimo and Schmidt [5] and validated in the Patchell trial [3], which showed improved outcomes for surgical decompression followed by radiotherapy. The variation in operative strategies, including tumour debulking and fusion, mirrors the heterogeneity described in modern surgical series such as those by Yaari et al. [14]. Although vertebroplasty and kyphoplasty were not used in our cohort, their efficacy for pain control in selected cases is supported by Sadeghi-Naini et al. [17]. The high proportion of patients presenting with Bilsky grade 3 compression suggests late presentation or aggressive tumour biology. This aligns with the challenges described in the development of the SINS classification by Fisher et al. [18]. The importance of prompt diagnosis and intervention is reinforced by Rades et al., who showed improved neurological outcomes with earlier treatment [19]. Despite the severity of radiological compression, most patients remained neurologically intact on presentation, reflecting a dissociation between neuroimaging severity and neurological status, also observed by Fehlings et al. [12]. The post-operative improvements in functional status and pain scores in this cohort echo findings from Patchell et al. [3] and Choi et al. [7]. Notably, functional improvement and pain relief, as reflected in EQ-5D and ODI scores, reinforce that surgical intervention in metastatic spinal disease is primarily aimed at preserving meaningful life, even when survival may be limited. This may also suggest that preserved or improved functional capacity post-operatively may serve as a surrogate marker for systemic disease control and overall resilience. The overall complication rate was low, with no perioperative deaths and a 30-day mortality of 4.3%. This reinforces that surgery for metastatic spinal disease can be performed safely in appropriately selected patients, particularly when conducted within a multidisciplinary framework involving oncology, radiology, and rehabilitation teams.
Limitations:
This study has several important limitations that affect the interpretation and generalisability of its findings: The cohort size was relatively small, limiting statistical power for subgroup analyses (e.g., by tumour type, Bilsky grade, or SINS category). Consequently, observed survival differences between diagnostic groups should be interpreted with caution. As a single-centre, single-surgeon series, the study is susceptible to selection and referral bias, which may limit external validity. Surgeon-specific decision-making, institutional practices, and local referral patterns may reduce generalisability to centres with different case mixes, resources, or surgical strategies. Residual confounding is likely, as key prognostic variables, including performance status, detailed systemic disease burden, post-operative neurological status, and specific oncological therapies, were incompletely captured. Functional outcome data (VAS and EQ-5D) were also incomplete and analysed using complete-case methods, potentially affecting survival estimates and the observed magnitude of functional improvement. Some immortal time bias is unavoidable, since patients had to survive long enough to be referred, assessed, and undergo surgery. Therefore, survival estimates should be interpreted as reflecting outcomes in surgically selected patients discussed in a multidisciplinary setting, rather than all patients with metastatic spinal disease.
In this single-centre, single-surgeon series, surgery for metastatic spinal disease, including cord compression, led to meaningful improvements in pain and health-related quality of life, with survival outcomes broadly consistent with previously reported surgical cohorts. These findings support the role of surgical intervention within a multidisciplinary approach for appropriately selected patients. However, the retrospective design, modest cohort size, and incomplete functional outcome data mean that the results should be interpreted as descriptive and hypothesis-generating. Larger prospective, multi-centre studies with standardised neurological, oncological, and patient-reported outcome measures are needed to better define prognostic factors and the incremental benefit of surgery.
Metastatic spinal disease, including cord compression, is a time-critical emergency. Despite the modest cohort size, our data emphasize the importance of integrating tumor biology, functional status, and mechanical stability into surgical decision-making, and suggest that the primary aim of surgery is to relieve pain and improve quality of life rather than prolong survival.
References
- 1. Cole JS, Patchell RA. Metastatic spinal cord compression: Epidemiology and clinical presentation. Clin Oncol (R Coll Radiol) 2009;21:753-9. [Google Scholar] [PubMed]
- 2. Loblaw DA, Laperriere NJ. Emergency treatment of malignant extradural spinal cord compression: An evidence-based guideline. J Clin Oncol 1998;16:1613-24. [Google Scholar] [PubMed]
- 3. Patchell RA, Tibbs PA, Regine WF, Payne R, Saris S, Kryscio RJ, et al. Direct decompressive surgical resection in the treatment of spinal cord compression caused by metastatic cancer: A randomised trial. Lancet 2005;366:643-8. [Google Scholar] [PubMed]
- 4. Zaikova O, Giercksky KE, Fosså SD, Kvaløy S, Johannesen TB, Skjeldal S. A population-based study of spinal metastatic disease in South-East Norway. Clin Oncol (R Coll Radiol) 2009;21:753-9. [Google Scholar] [PubMed]
- 5. Klimo P Jr., Schmidt MH. Surgical management of spinal metastases. Oncologist 2004;9:188-96. [Google Scholar] [PubMed]
- 6. Kim HJ, Park JS, Park SJ, Kang DH, Lee CS. Survival and prognostic factors after surgery in single spinal metastasis: Comparison of isolated-single spinal metastasis and single spinal metastasis with other metastasis. Glob Spine J 2024;15:2246-54. [Google Scholar] [PubMed]
- 7. Choi D, Fox Z, Albert T, Arts M, Balabaud L, Bünger C, et al. Prediction of quality of life and survival after surgery for symptomatic spinal metastases: A multicenter cohort study to determine suitability for surgical treatment. Neurosurgery 2015;77:698-708. [Google Scholar] [PubMed]
- 8. Roberts TT, Leonard GR, Cepela DJ. Classifications in brief: American spinal injury association (ASIA) impairment scale. Clin Orthop Relat Res 2017;475:1499-504. [Google Scholar] [PubMed]
- 9. Todd NV. Guidelines for cauda equina syndrome. Red flags and white flags. Systematic review and implications for triage. Br J Neurosurg 2017;31:336-9. [Google Scholar] [PubMed]
- 10. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004;240:205-13. [Google Scholar] [PubMed]
- 11. Copay AG, Glassman SD, Subach BR, Berven S, Schuler TC, Carreon LY. Minimum clinically important difference in lumbar spine surgery patients: A choice of methods using the oswestry disability index, medical outcomes study questionnaire short form 36, and pain scales. Spine J 2008;8:968-74. [Google Scholar] [PubMed]
- 12. Fehlings MG, Nater A, Tetreault L, Kopjar B, Arnold P, Dekutoski M, et al. Surgical management of metastatic spinal cord compression: A systematic review. J Neurosurg Spine 2010;13:710-8. [Google Scholar] [PubMed]
- 13. Lomas MT, Laba TL. Outcomes of surgery for metastatic spinal cord compression: A 10-year institutional experience. Spine 2006;31:2424-9. [Google Scholar] [PubMed]
- 14. Yaari LS, Novack L, Shemesh S, Sidon E, Haviv B, Sheinis D, et al. Patient outcomes and survival following surgery for spinal metastases. J Spinal Cord Med 2021;44:204-11. [Google Scholar] [PubMed]
- 15. Zanaty A, George KJ. Outcomes and efficiency of managing patients admitted for surgery for spinal metastases. Surg Neurol Int 2022;13:312. [Google Scholar] [PubMed]
- 16. Bhanot K, Widdifield J, Huang A, Paterson JM, Shultz DB, Finkelstein J. Survival after surgery for spinal metastases: A population-based study. Can J Surg 2022;65:E512-8. [Google Scholar] [PubMed]
- 17. Sadeghi-Naini M, Aarabi S, Shokraneh F, Janani L, Vaccaro AR, Rahimi-Movaghar V. Vertebroplasty and kyphoplasty for metastatic spinal lesions: A systematic review. Clin Spine Surg 2018;31:203-10. [Google Scholar] [PubMed]
- 18. Fisher CG, DiPaola CP, Ryken TC, Bilsky MH, Shaffrey CI, Berven SH, et al. A novel classification system for spinal instability in neoplastic disease: An evidence-based approach and expert consensus from the spine oncology study group. Spine (Phila Pa 1976) 2010;35:E1221-9. [Google Scholar] [PubMed]
- 19. Rades D, Veninga T, Fehlauer F, Stalpers LJ, Schulte RW, Obralic N, et al. Prognostic factors and results of radiotherapy alone in metastatic spinal cord compression: A scoring system. Radiother Oncol 2008;87:197-203. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Multifocal Non-contiguous Spinal Tuberculosis: A Report of 3 Surgically-Treated Patients
April 1, 2026 Multifocal Non-contiguous Spinal Tuberculosis: A Report of 3 Surgically-Treated Patients March 1, 2025 Surgical Interventions in Chronic Recurrent Multifocal Osteomyelitis Affecting the Spine: A Case Report with Literature Review
March 1, 2025 Surgical Interventions in Chronic Recurrent Multifocal Osteomyelitis Affecting the Spine: A Case Report with Literature Review July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes
July 1, 2026 Stepwise Surgical Correction of Fixed Flexion Deformity in Total Knee Arthroplasty: Functional Outcomes July 1, 2026 Chronic Acromioclavicular Joint Instability: Outcomes after Stabilization without Tendon Graft Augmentation
July 1, 2026 Chronic Acromioclavicular Joint Instability: Outcomes after Stabilization without Tendon Graft Augmentation