
Radial head prosthesis provides superior stability and functional scores, particularly in unstable or complex fractures, whereas radial head excision remains a viable option for isolated fractures in low-demand patients despite a higher long-term risk of valgus instability.
Dr Hemal Kumar V. Patel, Department of Orthopaedics, B.J. Medical College and Civil Hospital, Ahmedabad - 380016, Gujarat, India. E-mail: patelhemal777@gmail.com
Abstract
Introduction: Complex comminuted fractures of the radial head (Mason type III/IV) remain challenging to manage. This study compares functional and clinical outcomes between radial head prosthesis and excision.
Materials and Methods: This retrospective study included 40 adult patients who underwent operative management for acute, displaced radial head fractures (Mason Type III or IV) at a single institution between November 2022 and November 2024. A total of 2 years of the patient’s medical records, operative reports, and radiographic images were reviewed. Patients were categorised into two treatment groups: Group A (Excision, n = 20) received radial head excision, and Group B (Replacement, n = 20) was treated with metallic radial head replacement arthroplasty. Inclusion criteria required a minimum of 6-month follow-up. Pre-operative data, including patient demographics, injury mechanism, and fracture classification, were collected, and post-operative follow-up data focused on assessing clinical outcomes using the Mayo Elbow Performance Index (MEPI) and Broberg-Morrey scores, alongside complications.
Results: The mean age was 44 years of age with a standard deviation of ±7.4. Operative time (69.85 vs. 50.4 min, P < 0.001) and hospital stay (7.6 vs. 4.95 days, P = 0.0003) were longer for the prosthesis. MEPI and Broberg-Morrey scores were higher in the prosthesis group at all follow-ups (P < 0.05). Instability occurred in 40% of excision cases but none in prosthesis cases.
Conclusion: Radial head replacement offers better early functional outcomes and joint stability.
Keywords: Radial head fracture, prosthesis, excision, functional outcome, elbow instability.
In the past 30 years, our enhanced comprehension of the elbow has provided critical insights into the intricacies of this diarthrodial joint [1]. The functional anatomy of the elbow joint complex is unique in orientation and configuration. The elbow is the mechanical junction between the first two segments of the upper limb [2]. The radial head is a crucial element that facilitates the elbow’s inherent stable motion through a synergistic connection between a bony foundation and its adjacent soft tissue [1]. The radial head is crucial for preserving elbow stability, especially against valgus stress, accounting for approximately 30% of valgus resistance [3]. Studies indicate that radial head fractures constitute between 1.7% and 5.4% of all fractures [1]. Radial head fractures constitute 20% of all elbow fractures and are prevalent injuries [1]. Radial head fractures are the most prevalent type of elbow fracture, occurring at a rate of 2.5–2.9/10,000 individuals each year [1]. Cutler (1926), in one of the earliest extensive reviews, suggested that direct trauma was the most prevalent mechanism of injury to the radial head [4]. Research on static loading at the elbow indicates that approximately 60% of the force is conveyed through the radio capitellar joint [4]. The primary objective of surgical intervention is to restore elbow stability to maintain the intricate physiological kinematics of the elbow [5]. Inadequate surgical intervention may result in adverse results, including post-traumatic arthritis, instability, and stiffness [6]. Radial head excision has traditionally been executed for irreparable fractures; however, long-term consequences, including proximal radial migration, valgus instability, diminished grip strength, and secondary osteoarthritis, have restricted its application [3]. Modern prosthetic designs have established radial head replacement as a dependable option, reinstating joint biomechanics and averting instability-related complications [3]. Numerous comparative studies have demonstrated enhanced functional outcomes and less degenerative alterations with replacement relative to excision [3]. The Mason classification, subsequently revised by Kumar et al., continues to serve as the benchmark for the categorisation of radial head fractures [3]. Mason type I and II injuries are often treated conservatively or with open reduction and internal fixation (ORIF); however, Mason type III (comminuted) and type IV (with dislocation) present considerable treatment problems. In such instances, ORIF frequently fails due to comminution, suboptimal bone quality, and concomitant instability, necessitating excision or prosthetic replacement [3]. The present study aims to compare the long-term functional outcomes of radial head excision versus prosthesis in surgically treated Mason type III/IV fractures to determine the ideal management approach.
An observational study was undertaken in the Department of Orthopaedics, B.J. Medical College and Civil Hospital, Ahmedabad, from November 2022 to November 2024. There were 40 skeletally mature patients with Mason type III/IV radial head fractures; all of them were included in the study. 20 underwent prosthetic replacement, whereas 20 underwent excision. Exclusion criteria: Associated fractures of the proximal ulna/distal humerus, open fractures, distal radio-ulnar joint disruption, terrible triad injuries, and pre-existing arthritis. All procedures used the Kocher approach. Owing to the retrospective nature of this study, treatment groups were not randomised. The surgical intervention – either radial head excision or replacement – was dictated by the attending surgeon’s clinical judgement, primarily accounting for Mason fracture type, concomitant ligamentous injury, and the patient’s activity level. In the prosthesis group, the comminuted head was excised and replaced with an appropriately sized prosthesis. In the excision group, fragments were removed, and bone ends were smoothed. Functional assessments were done using Mayo Elbow Performance Score (MEPS) and Broberg-Morrey scales at 3 weeks, 3 months, and 6 months. Data were analysed using an independent t-test and Chi-square tests, with significance at P < 0.05. The MEPS is a 100-point scale that evaluates elbow function based on pain, range of motion, stability, and daily function. Scores are categorised as follows: excellent (90–100), good (75–89), fair (60–74), or poor (<60). The Broberg and Morrey Elbow score is a widely used clinical tool to assess elbow function after injury or surgery, particularly radial head fractures, evaluating pain, motion (range of motion [ROM]), strength, stability, and patient satisfaction/function, assigning points for each, with higher scores (up to 100) indicating better outcomes (excellent: 95–100, good: 80–94, fair: 60–79, poor: <60) by looking at ranges of flexion/extension, forearm rotation, grip, and pain levels.
Surgical procedure:
- Anesthesia
- General or brachial plexus nerve blocks.
- Patient positioning and preparation
- Orientation: The patient is placed in the supine position. The affected limb is draped and positioned on a radiolucent hand table with the elbow flexed to 90°
- Haemostasis: A pneumatic tourniquet is applied to the proximal upper arm to ensure a bloodless surgical field, optimising visualisation of the deep structures.
- Surgical exposure (The Kocher Approach) (Fig. 1)
- Incision: A 5–7 cm longitudinal skin incision is centered over the lateral epicondyle, extending distally toward the ulnar shaft
- Deep dissection: The interval is developed between the anconeus (radial nerve) and the extensor carpi ulnaris
- Neurological protection: To protect the posterior interosseous nerve, the forearm is maintained in pronation throughout the dissection. This manoeuvre shifts the nerve anteriorly, increasing the safety margin from the surgical site.
- Capsulotomy and articular access
- Incising the capsule: The common extensor origin and lateral joint capsule are incised to reveal the radio-capitellar joint
- Annular ligament: The annular ligament is identified and divided longitudinally, providing clear exposure of the radial head and neck
- Ligamentous preservation: High priority is given to preserving the lateral ulnar collateral ligament. Iatrogenic injury to this structure must be avoided to prevent subsequent posterolateral rotatory instability.

Figure 1: Kocher’s approach.
In case of radial head resection:
- Fragment removal: All loose osteochondral fracture fragments are identified and excised
- Osteotomy level: The resection level is typically planned at the proximal border of the proximal radioulnar joint (PRUJ)
- Bone work: A transverse osteotomy of the radial neck is performed using an oscillating saw or osteotome
- Refinement: The residual bone edges are meticulously contoured using a rongeur or rasp. This prevents soft tissue irritation and minimizes the risk of heterotopic ossification
- Lavages: The joint is thoroughly cleared of hematoma and micro-fragments using pulsatile lavage
- Secondary assessment: The articular surfaces of the capitellum and the proximal ulna are carefully inspected to rule out or address concomitant chondral shearing or “kissing” lesions.
In case of radial head replacement:
- Radial neck resection
Using an oscillating saw, a transverse osteotomy is performed perpendicular to the long axis of the radius. This cut is typically made at the level of the proximal border of the PRUJ to prepare the surface for the implant.
- Preparation of the medullary canal
Access to the radial canal is established using a starter awl or a small burr. This creates a clear entry point and path for the prosthetic stem.
- Graduated canal shaping
The canal is incrementally widened using sequential rasps or reamers. This ensures the bone is precisely contoured to provide a stable, “snug” fit for the specific dimensions of the final implant.
- Trial implantation and sizing
A trial stem and head are inserted to assess the restoration of the “lateral column”. This step is critical for evaluating how the components interface with the surrounding anatomy.
- Height and alignment verification
To prevent “overstuffing” the joint (which can lead to pain and stiffness), the trial head height is verified. The top of the implant should sit flush with the proximal border of the coronoid process.
- Dynamic kinematic testing
The elbow is put through a full range of motion – including flexion, extension, and forearm rotation – to confirm smooth tracking against the capitellum and proper stability within the PRUJ.
- Final component fixation
Once the fit is confirmed, the permanent prosthesis is seated. Depending on the patient’s bone quality and the design of the implant, the stem is either press-fit (for long-term biological integration) or secured with bone cement. Ligaments were sutured if not damaged, and layered sutures were taken.
Rehabilitation protocol:
Radial head replacement:
This procedure uses a prosthetic implant to maintain the elbow’s structural integrity.
- Primary objective: Maintain joint stability and proper alignment while ensuring the implant is sized correctly to avoid “overstuffing” (excessive pressure on the joint)
- Initial protection: The arm is typically secured in a posterior splint at 90° flexion for the first 10–14 days to allow tissues to begin healing
- Movement protocol: If the joint is deemed stable, active-assisted ROM starts early – often within 48 h post-op
- Key restrictions: To ensure the prosthetic stem integrates properly, patients must avoid heavy lifting and aggressive stretching into full extension until week 6
- Clinical focus: Recovery prioritises protecting the LCL/MCL repairs and preventing the implant from loosening over time.
Radial head excision (resection):
This procedure involves the complete removal of the radial head, prioritising immediate mobility and pain reduction.
- Primary objective: Eliminate painful bone-on-bone contact and facilitate a rapid return to movement
- Initial protection: Minimal downtime; a simple sling is used for comfort, usually for only 1–3 days
- Movement protocol: To prevent the elbow from “freezing”, active ROM is encouraged almost immediately (within 24–48 h)
- Key restrictions: Weight-bearing is generally advanced as quickly as the patient’s pain tolerance allows, offering a faster timeline than arthroplasty
- Clinical focus: Long-term monitoring is essential to watch for proximal radial migration (the radius shifting toward the shoulder) or valgus instability (weakness on the inner elbow).
Follow-up period:
Post-op, week 2 (suture removal), week 6, month 3, month 6.
We analysed 40 patients with severe radial head fractures, split evenly between radial head excision (20 patients) and prosthetic replacement (20 patients). All subjects were tracked for a minimum of 6 months to evaluate recovery.
Surgical and clinical distribution
Data from the procedures showed that patients receiving a prosthesis faced longer operative times and more extended hospital stays than those who underwent excision. Despite the more intensive initial surgical requirements, the prosthetic group showed distinct advantages in long-term recovery.
Functional performance
The effectiveness of each treatment was measured at three intervals (3 weeks, 3 months, and 6 months) using the MEPS and the Broberg-Morrey scale.
- Final scores: By the 6-month mark, the prosthetic replacement group achieved significantly higher functional scores on both the MEPS and Broberg-Morrey scales (P < 0.05) compared to the excision group
- Mobility trade-offs: The two methods resulted in different mechanical advantages for the elbow
- Flexion: Patients with a prosthesis reached a superior range of flexion
- Extension: Conversely, patients in the excision group retained better elbow extension
- Complications: The most significant disparity between the two methods is the incidence of joint instability. While 40% of the excision group experienced instability, the most frequent complication for that cohort, the prosthesis group reported no such cases. In contrast, the prosthetic approach was uniquely associated with mechanical and biological hurdles, including elbow stiffness (10%) and osteolysis (5%), complications that were entirely absent in the excision group. Although both procedures carried an identical 5% risk of infection, the overall data suggest a clear trade-off: A prosthesis successfully prevents instability but introduces risks of stiffness and bone degradation that excision avoids.
Limitations of the study
While this study provides valuable insight into the comparison of radial head prosthesis versus excision in comminuted radial head fractures, several limitations, such as small sample size, geographical area, loss to follow-up, and lack of old data, must be taken into consideration.
A radial head fracture constitutes one component of the terrible triad injury, and for optimal healing, it requires appropriate care [1]. The management of comminuted Mason type III radial head fractures accompanied by ligament damage remains contentious [4]. Multiple surgical interventions have been proposed for these intricate injuries, including ORIF, removal of the radial head, and radial head replacement [4]. A fracture of the radial head is likely to impair its blood supply. The ORIF of a comminuted radial head is frequently technically challenging. Consequently, ORIF is deemed unreliable for comminuted fractures due to the potential for osteonecrosis, non-union, or displacement of fragments [4]. This study involved a total of 40 individuals who underwent surgery and were meticulously examined for a duration of 6 months. Twenty patients underwent radial head excision, while another twenty received a radial head prosthesis. This retrospective study included randomly selected patients, and the entire research was completed based on follow-up data. The operative time and hospital stay were longer in replacement than in excision (Table 1).
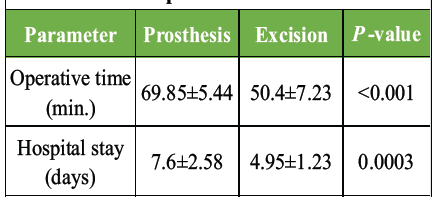
Table 1: Comparison of hospital stay and operative time
While comparing the data at 6 months, MEPS scores were higher in prosthesis patients and Broberg-Morrey scores were also higher in prosthesis patients (Table 2).
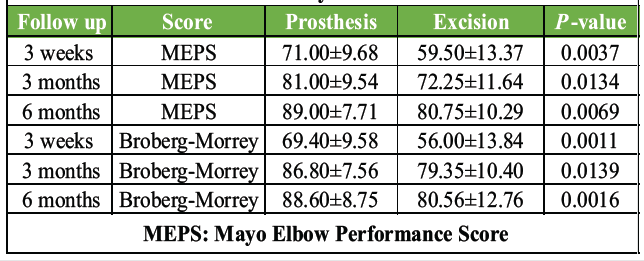
Table 2: Functional outcomes measured by MEPS and Broberg-Morrey scales
While comparing the individual movements at the end of 6 months, better elbow flexion was seen in replacement patients while better extension result seen in radial excision patients (Table 3).
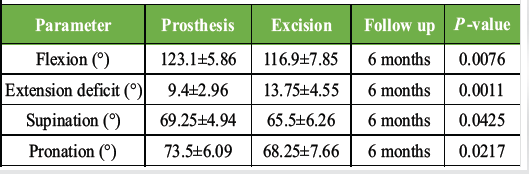
Table 3: Range of motion comparisons at 6 months (Figs. 2 and 3)

Figure 2: Post-operative X-ray of radial head prosthesis with 6-month follow-up elbow movements.
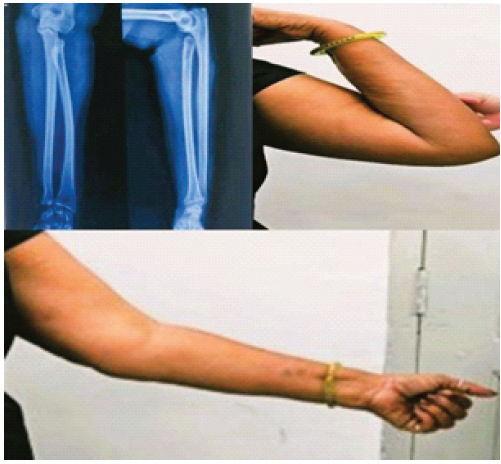
Figure 3: Post-operative X-ray of radial head excision with 6-month follow-up elbow movements.
While comparing the complications, 40% excision patients reported elbow instability at the end of 6 months; none were seen in the replacement group. The rate of infection was similar in both patients and elbow stiffness was seen in 10% of replacement patients, none in excision. In the study published by Lópiz et al. and Kumar et al., there were higher MEPS scores [7,8]. The absence of the radial head modifies stress distribution across the forearm and elbow, increasing the risk of instability, valgus deformity, and arthritis, especially in younger and more active individuals [3]. Replacement, conversely, sustains radio capitellar contact, hence preserving joint kinematics and spreading axial stress. Numerous biomechanical investigations demonstrate that prosthesis replacement reinstates valgus and axial stability more well than excision, aligning with our findings [3]. Research by Herbertsson et al. indicated that removal of the radial head may result in stiffness, weakness, and pain [9]. Our study yielded the same results. Harrington et al. documented that among 20 instances of titanium radial head replacement, with an average follow-up of 12 years (range, 6–9 years), 16 cases exhibited excellent or good outcomes without any prosthesis-related problems [10]. Radial head replacement can establish efficient radio-capitellar contact, enhancing stability under valgus, posterolateral, and axial stress of the forearm [11]. This therapy strategy yields satisfactory short- and mid-term outcomes [11]. Lópiz et al. advocated radial head replacement as the primary treatment choice in a recent study, citing a higher incidence of complications, increased reoperation rates, and inferior clinical outcomes in patients who underwent radial head resection [7]. By offering comparative data from an Indian tertiary care context, our study contributes to the body of existing knowledge. Limitations include the small sample size and the retrospective methodology. To assess late problems such as arthritis and prosthesis loosening, a lengthier follow-up is also required. Notwithstanding these drawbacks, the study offers solid proof that radial head replacement is the best surgical approach for comminuted fractures [3]. Radial head arthroplasty provides a reliable foundation for long-term limb function and consistently yields excellent results when treating non-reconstructable, comminuted fractures [12].
This study concluded that radial head replacement is a realistic and favourable alternative for Mason type III/IV radial head fractures. Radial head replacement resulted in superior joint stability and improved functional outcomes compared to radial head excision. Excision remains a viable choice for low-demand patients or in the absence of prosthetic implants. Additional longitudinal studies are advised to assess implant durability and delayed problems.
The below data contain all the post-operative parameters of the prosthetic and excision groups at different intervals.
| Table 1: Comparison of hospital stay and operative time | |||
| Parameter | Prosthesis | Excision | P-value |
| Operative time (min.) | 69.85±5.44 | 50.4±7.23 | <0.001 |
| Hospital stay (days) | 7.6±2.58 | 4.95±1.23 | 0.0003 |
| Table 2: Functional outcomes measured by MEPS and Broberg-Morrey scales | ||||
| Follow up | Score | Prosthesis | Excision | P-value |
| 3 weeks | MEPS | 71.00±9.68 | 59.50±13.37 | 0.0037 |
| 3 months | MEPS | 81.00±9.54 | 72.25±11.64 | 0.0134 |
| 6 months | MEPS | 89.00±7.71 | 80.75±10.29 | 0.0069 |
| 3 weeks | Broberg-Morrey | 69.40±9.58 | 56.00±13.84 | 0.0011 |
| 3 months | Broberg-Morrey | 86.80±7.56 | 79.35±10.40 | 0.0139 |
| 6 months | Broberg-Morrey | 88.60±8.75 | 80.56±12.76 | 0.0016 |
| MEPS: Mayo Elbow Performance Score | ||||
| Table 3: Range of motion comparisons at 6 months (Figs. 2 and 3) | ||||
| Parameter | Prosthesis | Excision | Follow up | P-value |
| Flexion (°) | 123.1±5.86 | 116.9±7.85 | 6 months | 0.0076 |
| Extension deficit (°) | 9.4±2.96 | 13.75±4.55 | 6 months | 0.0011 |
| Supination (°) | 69.25±4.94 | 65.5±6.26 | 6 months | 0.0425 |
| Pronation (°) | 73.5±6.09 | 68.25±7.66 | 6 months | 0.0217 |
References
- 1. Varma N, Anand G, James B. A comparative study of outcome of radial head fracture treated with radial head replacement and radial head excision alone. Indian J Orthop Surg 2023;8:244-51. [Google Scholar] [PubMed]
- 2. Mebouinz FN, Kasse A, Habib Sy M. Results of radial head resection after Mason type 3 or 4 fracture of the elbow. Clin Shoulder Elb 2020;23:131-5. [Google Scholar] [PubMed]
- 3. Kumar M, Nagakumar JS, Agrawal A. Clinico-radiological outcomes of radial head excision versus replacement: A retrospective comparative study. Int J Adv Res 2025;13:628-33. [Google Scholar] [PubMed]
- 4. Singh AK, Jidge A, Ramteke U, Venkateswaran N, Rokade H, Mulje SM, et al. Functional outcome of elbow kinematics in radial head excision versus radial head replacement: A comparative study. Open Access Maced J Med Sci 2019;7:1505-8. [Google Scholar] [PubMed]
- 5. Catellani F, De Caro F, De Biase CF, Perrino VR, Usai L, Triolo V, et al. Radial head resection versus arthroplasty in unrepairable comminuted fractures Mason type III and type IV: A systematic review. BioMed Res Int 2018;2018:4020625. [Google Scholar] [PubMed]
- 6. Sinha S, Sarkar S, Singh A, Saraf SK, Rastogi A, Singh T. Radial head arthroplasty, excision and osteosynthesis in complex elbow fracture-dislocations in young adults: What is preferred? Indian J Orthop 2020;54 Suppl 2:260-9. [Google Scholar] [PubMed]
- 7. Lópiz Y, González A, García-Fernández C, García-Coiradas J, Marco F. Comminuted fractures of the radial head: Resection or prosthesis? Injury 2016;47 Suppl 3:S29-34. [Google Scholar] [PubMed]
- 8. Kumar P, Jindal K, Rajnish RK, Patel S, Sharma S, Kumar V, et al. Excision versus replacement in unrepairable comminuted fractures of the radial head: A systematic review of outcomes and complications. Indian J Orthop 2022;56:1305-15. [Google Scholar] [PubMed]
- 9. Herbertsson P, Josefsson PO, Hasserius R, Besjakov J, Nyqvist F. Fractures of the radial head and neck treated with radial head excision. J Bone Joint Surg Am 2004;86:1925-30. [Google Scholar] [PubMed]
- 10. Harrington IJ, Sekyi-Otu A, Barrington TW, Evans DC, Tuli V. The functional outcome with metallic radial head implants in the treatment of unstable elbow fractures: A long-term review. J Trauma 2001;50:46-52. [Google Scholar] [PubMed]
- 11. Kim BS, Cho CH. Radial head resection versus replacement for unreconstructable radial head fractures. Clin Shoulder Elb 2020;23:117-8. [Google Scholar] [PubMed]
- 12. Ganai MR, Khan SS, Rahim I, Maajid S, Dar TA. Short term outcome of radial head arthroplasty in Mason type 3 and 4 fractures. Int J Res Orthop 2021;7:830-3. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2024 Terrible Triad Injuries around the Elbow: It is Still a Puzzle? Prospective Study
October 1, 2024 Terrible Triad Injuries around the Elbow: It is Still a Puzzle? Prospective Study August 1, 2026 Intramuscular Glomus Tumor of Foot Presenting as Neuroma of Sural Nerve: A Case Report
August 1, 2026 Intramuscular Glomus Tumor of Foot Presenting as Neuroma of Sural Nerve: A Case Report August 1, 2026 Outcome of Retrograde Titanium Elastic Nailing System in Shaft of Humerus Fractures: A Case Series
August 1, 2026 Outcome of Retrograde Titanium Elastic Nailing System in Shaft of Humerus Fractures: A Case Series August 1, 2026 A Prospective Analysis of Physeal-Sparing Intramedullary Interlocking Nail for Adolescent Tibial Shaft Fractures
August 1, 2026 A Prospective Analysis of Physeal-Sparing Intramedullary Interlocking Nail for Adolescent Tibial Shaft Fractures