
Intralesional triamcinolone injection is more effective than oral bisphosphonates for treating benign cystic bone lesions, providing significantly superior pain relief, faster radiological healing, and better promotion of internal calcification over a 6-month period.
Dr. Balram Kalme, Department of Orthopedics, Nandkumar Singh Chouhan Government Medical College, Khandwa, Madhya Pradesh, India. E-mail: drbalramkalme@gmail.com
Abstract
Introduction: Benign cystic bone lesions, particularly solitary bone cysts and aneurysmal bone cysts, predominantly affect children and adolescents, posing significant orthopaedic challenges. This study was therefore designed to compare intralesional triamcinolone injection and oral bisphosphonate therapy in patients with benign cystic bone lesions, with respect to radiological healing and pain outcomes over a 6-month follow-up period.
Materials and Methods: This prospective study enrolled 60 patients with benign cystic bone lesions at the Department of Orthopaedics and Trauma Centre, J.A. Group of Hospitals, Gwalior, India. Patients were randomly allocated to Group A (intralesional triamcinolone injection, n = 30) or Group B (oral bisphosphonate, n = 30). Radiological outcomes were assessed using Cole’s modification of the Neer grading system, and pain was measured using the Visual Analogue Scale (VAS) at baseline, 1, 3, and 6 months. Statistical analyses included the Mann–Whitney U test and McNemar’s test.
Results: Both groups were comparable at baseline for age, gender, pain duration, and side of involvement. At 6 months, Group A demonstrated significantly superior pain reduction (VAS: 1.48 ± 1.33) compared to Group B (VAS: 5.48 ± 1.50; P < 0.001). Radiological improvement (decrease in Neer grade) occurred in 60% of Group A vs 40% in Group B (P = 0.03). Internal calcification and mineralisation were significantly more frequent in Group A (40%) than Group B (16.7%; P = 0.044). Neer-Cole Grade 1 (complete healing) was achieved in 56.67% of Group A versus 23.33% of Group B.
Conclusion: Intralesional triamcinolone injection demonstrated superior efficacy compared to oral bisphosphonate in managing benign cystic bone lesions with respect to pain reduction, radiological improvement, and promotion of calcification. Bisphosphonates remain valuable as adjunctive or alternative therapy in specific clinical scenarios. Larger randomised controlled trials with long-term follow-up are warranted.
Keywords: Solitary bone cyst, aneurysmal bone cyst, intralesional triamcinolone, bisphosphonate, neer-cole grading, pathological fracture, benign bone lesion.
Benign cystic bone lesions, including solitary (unicameral) bone cysts (SBCs) and aneurysmal bone cysts (ABCs), represent a clinically important group of pediatric bone disorders. SBCs predominantly affect the proximal humerus (approximately 70% of cases) and proximal femur (approximately 25% of cases) in skeletally immature patients [1,2]. These fluid-filled lesions are generally benign but carry a significant risk of pathological fracture, growth disturbance, and, in rare instances, growth arrest [3]. The etiology of SBCs remains incompletely understood. Proposed mechanisms include venous obstruction with resultant increased intra-cystic pressure, active bone resorption mediated by the cyst lining, chronic inflammation, and traumatic events [4,5]. The cyst fluid is typically clear to amber and contains a complex mixture of histiocytes, inflammatory cells, giant cells, and prostaglandins [6]. Management of SBCs encompasses a broad spectrum of modalities: Injection therapies (corticosteroids, bone marrow aspirate, demineralized bone matrix, calcium sulfate pellets), mechanical curettage, flexible intramedullary nailing, and multimodal combinations [7,8]. Despite this range, outcomes remain variable. Traditional curettage and bone grafting carry high recurrence rates, prompting a shift toward minimally invasive approaches. Among these, intralesional injection of triamcinolone acetonide – a synthetic glucocorticoid – has gained wide acceptance, although reported healing rates have varied considerably across studies [9,10,11,12]. Despite the theoretical basis for bisphosphonates (BP) use in bone cysts, comparative data against established treatments such as triamcinolone injection remain scarce. This prospective study was therefore designed to compare intralesional triamcinolone injection and oral bisphosphonate therapy in patients with benign cystic bone lesions, with respect to radiological healing and pain outcomes over a 6-month follow-up period.
Study design and setting:
This prospective comparative study was conducted at the Department of Orthopaedics and Trauma Centre, J.A. Group of Hospitals, Gwalior, Madhya Pradesh, India. The study received approval from the Institutional Ethics Committee (No. 1067/IEC-GRMC/2022, dated September 01, 2022), and written informed consent was obtained from all participants or their legal guardians before enrolment.
Participants:
Sixty patients of all age groups diagnosed with benign cystic bone lesions were enrolled and randomly allocated into two equal groups of 30 each. Inclusion criteria comprised patients of any age with a radiologically confirmed benign bone cyst who provided consent for examination and follow-up. Exclusion criteria included refusal to consent, malignant bone tumours, bone marrow diseases, chronic corticosteroid use, ongoing chemotherapy, contraindications to steroid use, pregnancy, and significant medical comorbidities. Sample size was computed using the formula: n = 2s2 (Zα/2 + Z₁−β)2 / (μ₁−μ₂).
Interventions:
Group A patients underwent intralesional injection of triamcinolone acetonide. Pre-operatively, routine blood investigations, serology, chest radiograph, electrocardiogram, and plain radiograph of the affected region were obtained. The injection was administered in the operating theatre under strict aseptic conditions with C-arm fluoroscopic guidance. The cyst was punctured with two needles; its contents were aspirated with one needle while radiological contrast was injected simultaneously with the other needle to confirm the cystic nature and exclude ABCs, followed by instillation of triamcinolone acetonide [7]. Group B patients were prescribed oral bisphosphonates. Patients were instructed to take the medication on an empty stomach with one to two glasses of plain water and to remain upright for at least 30 min post-ingestion to minimise the risk of esophageal irritation.
Outcome measures:
Radiological assessment used Cole’s modification of the Neer grading system [13]: Grade 1: Cyst distinctly visible; Grade 2: Cyst visible but multilocular and opaque; Grade 3: Sclerosis around or within a partially visible cyst; Grade 4: Complete healing with total obliteration. Pain intensity was assessed using the 10-point Visual Analogue Scale (VAS) at baseline and at 1, 3, and 6 months post-treatment. Internal calcification and mineralisation were documented as present or absent on follow-up radiographs.
Statistical analysis:
Data were analysed using the Statistical Package for the Social Sciences v21.0. Continuous variables were compared with the independent samples t-test for normally distributed data and the Mann–Whitney U test for non-parametric data. Categorical variables were analysed using the chi-square or Fisher’s exact test. McNemar’s test was used for paired ordinal data (Neer-Cole grading before and after treatment). Statistical significance was set at P < 0.05.
Demographic and clinical characteristics:
The majority of participants (46.7%) were under 20 years of age, consistent with the known predilection of benign bone cysts for the skeletally immature [1,2]. Group A had a higher proportion of patients aged 20–30 years (53.3%), whereas Group B had a greater proportion under 20 years (60%). Overall, males constituted 63.3% of participants, with a higher male proportion in Group A (70%) than Group B (56.7%); this difference was not statistically significant (P = 0.290). The mean age was 23.44 ± 7.78 years in Group A and 22.52 ± 11.63 years in Group B (P = 0.732). Mean pain duration was 13.76 ± 9.71 months in Group A and 10.48 ± 6.87 months in Group B (P = 0.134), indicating comparable baseline chronicity. Both groups had identical right/left-side distribution (53.3%/46.7%, respectively; P = 1.000) (Tables 1 and 2).
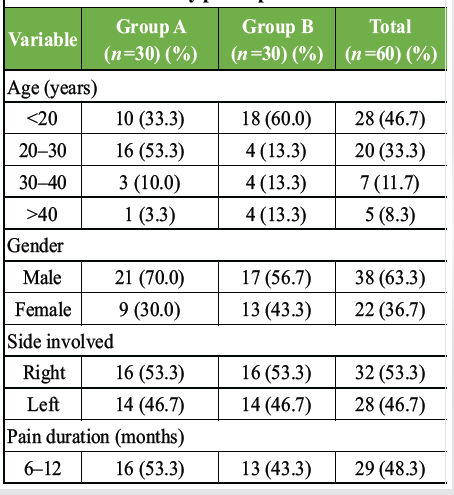 Table 1: Demographic and clinical characteristics of study participants
Table 1: Demographic and clinical characteristics of study participants
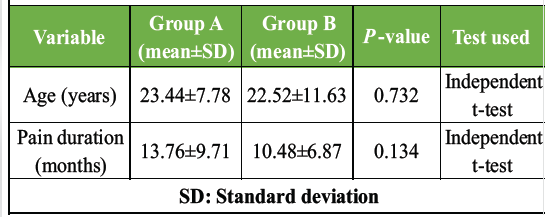 Table 2: Comparison of mean age, pain duration, and continuous variables between groups
Table 2: Comparison of mean age, pain duration, and continuous variables between groups
Tumour site distribution:
Cystic lesions were distributed across multiple long-bone sites. The most common locations were the proximal humerus left side (13% overall), distal femur left side (12%), and proximal tibia left side (12%). Group A had a higher proportion of distal femur left-side and proximal tibia left-side lesions (20% each), while Group B showed a greater concentration in the proximal humerus left side (27%). These site differences are relevant given variations in blood supply and mechanical loading that may influence treatment response (Table 3) [14].
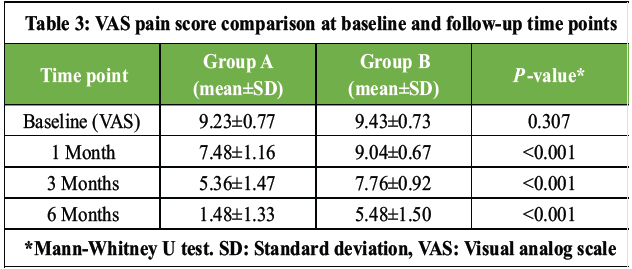 Table 3: VAS pain score comparison at baseline and follow-up time points
Table 3: VAS pain score comparison at baseline and follow-up time points
Radiological outcomes:
A statistically significant difference in radiological outcomes was observed between groups (P = 0.03). In Group A, 60% of patients demonstrated a decrease in radiological grade, compared with 40% in Group B. An increase in radiological grading (worsening) was noted in 10% of Group A and 30% of Group B, while 30% of patients in each group showed stable grades. Internal calcification and mineralisation were present in 40% of Group A patients versus 16.7% in Group B, a statistically significant difference (P = 0.044) (Table 4).
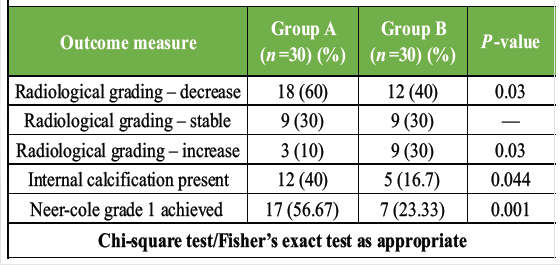 Table 4: Radiological outcomes and internal calcification at 6 months
Table 4: Radiological outcomes and internal calcification at 6 months
Near-cole grading improvement:
McNemar’s test confirmed statistically significant within-group improvements in both Group A (χ2 = 10.57, P = 0.001) and Group B (χ2 = 7.11, P = 0.008). Group A achieved an overall improvement rate of 56.67%, with 66.67% of patients initially at Grade 3 and 50% initially at Grade 4 advancing to Grade 1. Group B demonstrated an overall improvement rate of 23.33%; among those initially at Grade 4, only 11.11% improved to Grade 1, while 55.56% reached Grade 3, suggesting moderate rather than complete healing.
Pain outcomes (VAS scores):
Both groups exhibited comparable baseline pain levels (VAS: Group A 9.23 ± 0.77, Group B 9.43 ± 0.73; P = 0.307). At 1 month, Group A already showed significantly lower VAS scores (7.48 ± 1.16) compared to Group B (9.04 ± 0.67; P < 0.001). This divergence progressively widened: At 3 months, scores were 5.36 ± 1.47 versus 7.76 ± 0.92 (P < 0.001), and at 6 months, 1.48 ± 1.33 versus 5.48 ± 1.50 (P < 0.001) in Group A and Group B, respectively. By 6 months, the triamcinolone group had achieved near-complete pain resolution, while the bisphosphonate group retained clinically significant pain.
This study compared intralesional triamcinolone injection and oral bisphosphonate therapy for benign cystic bone lesions and found that triamcinolone was significantly superior with respect to pain reduction, radiological improvement, and promotion of internal calcification. These findings contribute to the ongoing discourse on optimal management of these lesions, for which no universally accepted standard of care exists [3,14]. The predominance of young patients (46.7% under 20 years) in our cohort is consistent with established epidemiology showing that SBCs account for approximately 3% of all primary bone tumours, with 85% of cases arising in children and adolescents [14]. The male predominance observed (63.3%) mirrors previously reported gender distribution patterns in SBCs [1,2]. The equal distribution of side involvement and comparable baseline pain duration across groups strengthened the internal validity of our comparisons. The significant reduction in VAS pain scores in the triamcinolone group at all-time points corroborates the well-established anti-inflammatory mechanism of corticosteroids. Triamcinolone inhibits the cyclooxygenase pathway and suppresses pro-inflammatory cytokines and prostaglandins, which are known to be elevated in the cyst fluid of SBCs [6,15]. A randomised controlled trial by Wright et al. similarly demonstrated the superiority of methylprednisolone acetate over bone marrow injection, with a 42% versus 23% healing rate, respectively, using the same Neer radiographic grading criteria employed in our study [13]. The significantly higher rate of internal calcification and mineralisation in Group A (40% vs. 16.7%, P = 0.044) supports the hypothesis that triamcinolone promotes osteoblast differentiation and stimulates deposition of bone matrix proteins, contributing to cyst stabilisation and healing [10,15]. Pavone et al. reported an 82.6% good response rate with corticosteroid injection in unicameral bone cysts over long-term follow-up, further supporting the utility of this approach [9]. BP primarily inhibits osteoclast-mediated bone resorption through the mevalonate pathway, preventing prenylation of essential small GTPases in osteoclasts [11,12]. Third-generation nitrogen-containing BP additionally exhibits anti-proliferative, pro-apoptotic, and angiostatic effects, which are relevant to the pathophysiology of cystic bone lesions [12,16]. Cornelis et al. reported pain relief within 6 weeks and ossification in nearly all patients with unresectable benign bone tumours treated with BP, suggesting a role particularly where corticosteroids are contraindicated [16]. In terms of radiological Neer-Cole grading, Group A achieved Neer Grade 1 (complete healing) in 56.67% of patients versus 23.33% in Group B. Interestingly, Group B patients initially at Grade 4 tended to improve to Grade 3 rather than achieving complete resolution, suggesting BP facilitates partial, rather than complete, healing. Deslivia et al.’s systematic review and meta-analysis on bisphosphonate use in giant cell tumours similarly found lower recurrence rates with BP therapy (odds ratio 0.15; 95% confidence interval 0.05–0.43), indicating their capacity to stabilise but not necessarily fully resolve bone lesions [17]. While triamcinolone demonstrated superior outcomes, the potential adverse effects of corticosteroids – including immunosuppression, glucocorticoid-induced osteoporosis, and adrenal suppression with repeated injections – must be carefully weighed, particularly in paediatric populations [15,18]. BP, by contrast, has a favourable safety profile in young patients when administered according to evidence-based consensus guidelines [18]. This makes BP a viable alternative for patients with corticosteroid contraindications or for long-term bone stabilisation. The combination of the two modalities represents an interesting avenue for future investigation: triamcinolone for rapid pain relief and calcification promotion, with BP providing longer-term antiresorptive support. Sclerotherapy approaches, such as that evaluated by Purnomo using triamcinolone acetonide as a single sclerosing agent for ABC with full lesion resolution over 3 years, also deserve further systematic study [19].
Limitations:
This study’s limitations include the relatively small sample size (n = 60), a 6-month follow-up period that may not capture late recurrence, the absence of quality-of-life metrics, and non-blinded outcome assessment. Differences in tumour site distribution between groups – though not statistically controlled – may have introduced site-specific confounding. The oral route of bisphosphonate administration, compared to the direct intralesional delivery of triamcinolone, represents an inherent pharmacokinetic disparity. Future randomised controlled trials with larger samples, longer follow-up, intralesional bisphosphonate arms, and patient-reported outcomes are warranted.
Intralesional triamcinolone showed superior pain relief and radiological healing compared with oral BP in benign cystic bone lesions. Intralesional steroids are preferable for accessible lesions where image-guided injection can be performed effectively, although technical difficulty may arise in deep or anatomically complex locations. Oral BP remains a useful non-invasive alternative for inaccessible lesions or patients unsuitable for corticosteroid therapy, despite a comparatively slower response. Further long-term multicenter studies are required to define optimal treatment selection.
Intralesional triamcinolone injection is significantly more effective than oral bisphosphonates for the management of benign cystic bone lesions, offering superior pain relief and more robust radiological healing. Patients treated with triamcinolone achieved a 56.67% complete healing rate compared to only 23.33% in the bisphosphonate group, while also demonstrating significantly higher rates of internal calcification. Although bisphosphonates remain a viable alternative for patients with corticosteroid contraindications, triamcinolone’s rapid anti-inflammatory and osteogenic effects make it the preferred primary intervention. Consequently, for paediatric and adolescent patients with symptomatic bone cysts, triamcinolone should be considered the first-line treatment to optimise clinical and structural outcomes.
References
- 1. Campanacci M, Capanna R, Picci P. Unicameral and aneurysmal bone cysts. Clin Orthop Relat Res 1986;204:25-36. [Google Scholar] [PubMed]
- 2. Wilkins RM. Unicameral bone cysts. J Am Acad Orthop Surg 2000;8:217-24. [Google Scholar] [PubMed]
- 3. Neer CS 2nd, Francis KC, Marcove RC, Terz J, Carbonara PN. Treatment of unicameral bone cyst. A follow-up study of one hundred seventy-five cases. J Bone Joint Surg Am 1966;48:731-45. [Google Scholar] [PubMed]
- 4. Chigira M, Maehara S, Arita S, Udagawa E. The aetiology and treatment of simple bone cysts. J Bone Joint Surg Br 1983;65:633-7. [Google Scholar] [PubMed]
- 5. Komiya S, Tsuzuki K, Mangham DC, Sugiyama M, Inoue A. Oxygen scavengers in simple bone cysts. Clin Orthop Relat Res 1994;308:199-206. [Google Scholar] [PubMed]
- 6. Jaffe HL, Lichtenstein L. Solitary unicameral bone cyst with emphasis on the roentgen picture, the pathologic appearance and the pathogenesis. Arch Surg 1942;44:1004-25. [Google Scholar] [PubMed]
- 7. Scaglietti O, Marchetti PG, Bartolozzi P. Final results obtained in the treatment of bone cysts with methylprednisolone acetate (depo-medrol) and a discussion of results achieved in other bone lesions. Clin Orthop Relat Res 1982;165:33-42. [Google Scholar] [PubMed]
- 8. Rougraff BT, Kling TJ. Treatment of active unicameral bone cysts with percutaneous injection of demineralized bone matrix and autogenous bone marrow. J Bone Joint Surg Am 2002;84:921-9. [Google Scholar] [PubMed]
- 9. Pavone V, Caff G, Di Silvestri C, Avondo S, Sessa G. Steroid injections in the treatment of humeral unicameral bone cysts: Long-term follow-up and review of the literature. Eur J Orthop Surg Traumatol 2014;24:497-503. [Google Scholar] [PubMed]
- 10. Cho HS, Oh JH, Kim HS, Kang HG, Lee SH. Unicameral bone cysts: A comparison of injection of steroid and grafting with autologous bone marrow. J Bone Joint Surg Br 2007;89:222-6. [Google Scholar] [PubMed]
- 11. Russell RG, Watts NB, Ebetino FH, Rogers MJ. Mechanisms of action of bisphosphonates: Similarities and differences and their potential influence on clinical efficacy. Osteoporos Int 2008;19:733-59. [Google Scholar] [PubMed]
- 12. Rogers MJ, Crockett JC, Coxon FP, Mönkkönen J. Biochemical and molecular mechanisms of action of bisphosphonates. Bone 2011;49:34-41. [Google Scholar] [PubMed]
- 13. Wright JG, Yandow S, Donaldson S, Marley L, Simple Bone Cyst Trial Group. A randomized clinical trial comparing intralesional bone marrow and steroid injections for simple bone cysts. J Bone Joint Surg Am 2008;90:722-30. [Google Scholar] [PubMed]
- 14. Rajasekaran RB, Krishnamoorthy V, Gulia A. Unicameral bone cysts: Review of etiopathogenesis and current concepts in diagnosis and management. Indian J Orthop 2022;56:741-51. [Google Scholar] [PubMed]
- 15. Weinstein RS. Glucocorticoid-induced osteoporosis and osteonecrosis. Endocrinol Metab Clin North Am 2012;41:595-611. [Google Scholar] [PubMed]
- 16. Cornelis F, Truchetet ME, Amoretti N, Verdier D, Fournier C, Pillet O, et al. Bisphosphonate therapy for unresectable symptomatic benign bone tumors: A long-term prospective study of tolerance and efficacy. Bone 2014;58:11-6. [Google Scholar] [PubMed]
- 17. Deslivia MF, Savio SD, Wiratnaya IG, Astawa P, Sandiwidayat KS, Bimantara NG. The efficacy of bisphosphonate in the treatment of giant cell tumour of the bone: A systematic review and meta-analysis. Malays Orthop J 2023;17:98-110. [Google Scholar] [PubMed]
- 18. Simm PJ, Biggin A, Zacharin MR, Rodda CP, Tham E, Siafarikas A, et al. Consensus guidelines on the use of bisphosphonate therapy in children and adolescents. J Paediatr Child Health 2018;54:223-33. [Google Scholar] [PubMed]
- 19. Purnomo G. Triamcinolone acetonide as a single sclerosing agent for aneurysmal bone cyst: A case report. Int J Surg Case Rep 2019;65:13-6. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Aneurysmal Bone Cyst of Lateral Cuneiform: Challenge in Diagnosis and Management
May 1, 2026 Aneurysmal Bone Cyst of Lateral Cuneiform: Challenge in Diagnosis and Management September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report
September 1, 2025 Aneurysmal Bone Cyst of Talus: A Case Report November 1, 2024 Ipsilateral Fibula Grafting in a Case of Aneurysmal Bone Cyst in Tibia Diaphysis: A Case Report
November 1, 2024 Ipsilateral Fibula Grafting in a Case of Aneurysmal Bone Cyst in Tibia Diaphysis: A Case Report February 10, 2023 An Uncommon Case Report: Pathologic Fracture in a Proximal Femur Aneurysmal Bone Cyst in a Child
February 10, 2023 An Uncommon Case Report: Pathologic Fracture in a Proximal Femur Aneurysmal Bone Cyst in a Child