
Antiphospholipid syndrome–associated Livedoid vasculopathy can produce sterile synovitis that fulfills published diagnostic criteria for periprosthetic joint infection, including markedly elevated synovial white blood cell count and a positive α-defensin; recognition of this non-infectious mimic may prevent unnecessary surgery and prolonged antimicrobial therapy.
Dr. Michael Booth, Department of Orthopaedics, Ohio State University, 543 Taylor Ave, Columbus - 43203, Ohio, United States. E-mail: booth.411@osu.edu
Abstract
Introduction: Periprosthetic joint infection (PJI) after total knee arthroplasty (TKA) is a serious complication whose diagnosis relies on a combination of serum and synovial biomarkers. Inflammatory non-infectious conditions can fulfil these same diagnostic criteria, creating a diagnostic and therapeutic challenge. We report the first case, to our knowledge, of antiphospholipid syndrome (APS)–associated livedoid vasculopathy (LV) mimicking recurrent PJI.
Case Report: A 74-year-old White male with a remote history of uncomplicated right TKA presented with two discrete episodes of presumed PJI (November 2025 and January 2026), each coinciding with a new right ankle lesion. Synovial fluid analysis on both occasions demonstrated markedly elevated white blood cell counts (WBC) (20,688 and 28,900 cells/µL; >93% neutrophils) and a positive synovasure α-defensin, yielding a 2018 International Consensus Meeting score of 10 on each presentation. Cultures and next-generation sequencing (NGS) were uniformly negative. The ankle lesions were ultimately biopsied and confirmed histologically as LV. Serology subsequently established a double-positive APS profile (positive lupus anticoagulant and anti-β2-glycoprotein I antibodies). All antimicrobials were discontinued; the patient declined two-stage revision arthroplasty. Repeat aspiration 3 weeks later showed completely normal synovial fluid (WBC 28 cells/µL, synovial C-reactive protein 0.01 mg/L). At 12 weeks off all therapy, the patient remains asymptomatic.
Conclusion: APS-associated LV can produce a thrombo-inflammatory sterile synovitis that satisfies established PJI diagnostic criteria, including a positive α-defensin. This case underscores the importance of evaluating concomitant dermatologic lesions, pursuing advanced microbiologic testing (NGS) before committing to surgical intervention, and considering hypercoagulable states in PJI workups with persistently negative cultures.
Keywords: Antiphospholipid syndrome, livedoid vasculopathy, periprosthetic joint infection, alpha-defensin, sterile synovitis, total knee arthroplasty, next-generation sequencing.
Periprosthetic joint infection (PJI) is among the most feared complications of total joint arthroplasty, affecting approximately 1–2% of primary total knee arthroplasty (TKA) procedures and carrying significant morbidity [1]. Diagnosis is guided by the 2018 International Consensus Meeting (ICM) scoring system, which integrates serum inflammatory markers, synovial fluid analysis (including white blood cell count [WBC], differential, and leukocyte esterase), culture results, and the synovial biomarker α-defensin [2,3]. Although highly sensitive for true infection, synovial α-defensin can yield false-positive results in the context of non-infectious inflammatory arthropathies, including rheumatoid arthritis, crystal arthropathy, and adverse local tissue reactions [4,5]. Livedoid vasculopathy (LV) is a rare thrombo-occlusive disorder of small dermal vessels manifesting as recurrent, painful purpuric ulcers on the lower extremities. It is frequently associated with underlying hypercoagulable states, most notably antiphospholipid syndrome (APS) [6]. APS is a systemic autoimmune condition defined by persistent antiphospholipid antibodies (aPLs) coupled with thrombotic events or pregnancy morbidity [7]. Its microvascular thrombotic–inflammatory pathophysiology has been documented across multiple organ systems, yet to date, no report has described APS-associated LV as a mimic of PJI in a patient with TKA. We describe a 74-year-old male who experienced two successive episodes of presumed PJI, each temporally linked to a new ankle lesion and each fulfilling formal PJI diagnostic criteria – while all cultures and next-generation sequencing (NGS) remained negative. Biopsy-proven LV and a subsequently confirmed double-positive APS profile, combined with rapid resolution of synovitis after aspiration alone, support a non-infectious, APS-driven thrombo-inflammatory mechanism. This case broadens the differential diagnosis of culture-negative PJI and highlights the diagnostic relevance of concurrent cutaneous findings.
First episode (November 2025):
A 74-year-old White male in excellent baseline health (maintaining a daily regimen of 9,000 stair steps) presented with a right posterior ankle lesion first noted on November 14, 2025. The lesion was initially attributed to a minor cat bite and self-treated with a single dose of amoxicillin-clavulanate. The following day, the patient developed systemic malaise, chills, fingertip blanching, and rapidly progressive stiffness and pain in the right knee. He presented to the emergency department on November 16, 2025. Initial laboratory evaluation revealed a serum C-reactive protein (CRP) of 43 mg/L, an erythrocyte sedimentation rate (ESR) of 10 mm/h, and a WBC of 4.8 × 109/L. Knee aspiration yielded synovial fluid with 20,688 WBC/µL (97% neutrophils) and a positive synovasure α-defensin lateral flow test, generating a 2018 ICM minor-criteria score of 10 points, consistent with PJI. The posterior ankle lesion at this time demonstrated a central ulcer with a shallow, crusted base surrounded by purpura and erythema characteristic of LV (Fig. 1).

Figure 1: Right posterior ankle lesion photographed the night before the first admission, demonstrating livedoid vasculopathy: Central ulcer with shallow, crusted base surrounded by purpura and erythema.
The patient underwent debridement, antibiotics, irrigation, and retention of the TKA on November 17, 2025. Intraoperative tissue analysis revealed Gram-positive cocci on stain in one of five specimens, considered a probable contaminant, with no growth on culture from any specimen. Blood and synovial fluid cultures were likewise negative. A peripherally inserted central catheter was placed, and the patient received 6 weeks of intravenous piperacillin-tazobactam plus daptomycin, followed by a planned 6-week course of oral amoxicillin-clavulanate plus doxycycline. Serum CRP normalised to 2 mg/L within 2 weeks of initiating intravenous therapy.
Second episode (January 2026):
On January 24th, 2026, while still completing the planned oral antibiotic course (week 10 of therapy), the patient developed identical prodromal symptoms and knee stiffness. He returned to the emergency department. Synovial fluid aspiration demonstrated 28,900 WBC/µL (93% neutrophils) and again yielded a positive α-defensin, with a 2018 ICM score of 10. Serum CRP rose to 53 mg/L, doubling by the following day, whereas ESR remained low at 7 mm/h. A new right ankle lesion was identified at this visit. NGS of synovial fluid performed at the University of Washington was negative for bacterial and fungal pathogens. Three punch biopsies of the new ankle lesion demonstrated the histologic hallmarks of LV: intraluminal fibrin deposition, segmental hyalinisation of small vessel walls, and lymphocytic perivascular infiltration without evidence of organisms. Rheumatology consultation was obtained, and all antimicrobials were discontinued per infectious disease guidance. Symptoms improved markedly following therapeutic aspiration. The patient declined the recommended two-stage revision arthroplasty and was discharged without antimicrobials. A clinical timeline is provided in Fig. 2.

Figure 2: Timeline of clinical events. Key milestones include initial ankle lesion appearance, debridement, antibiotics, irrigation, and retention, antimicrobial courses, second episode with biopsy-proven livedoid vasculopathy, aspiration-only management, serologic antiphospholipid syndrome confirmation, and sustained remission.
Follow-up and serologic confirmation:
At a routine 3-week follow-up on February 16, 2026, repeat aspiration using a MicroGenDX PJI Ortho kit revealed completely normal synovial parameters: WBC 28 cells/µL, 3.6% polymorphonuclear cells, and synovial CRP 0.01 mg/L. Serum CRP was 2.91 mg/L, ESR 5 mm/h, and systemic WBC 4.1 × 109/L, yielding a Musculoskeletal Infection Society score of 0. NGS from this aspiration was negative. Serologic evaluation performed 10 weeks after the second hospitalisation confirmed lupus anticoagulant positivity and positive anti-β2-glycoprotein I antibodies, establishing a double-positive APS profile under the 2023 American College of Rheumatology/European Alliance of Associations for Rheumatology (ACR/EULAR) classification criteria [7]. As of mid-April 2026 (12 weeks off all antimicrobial and anticoagulant therapy, on low-dose aspirin only), the patient remains entirely asymptomatic and has returned to his pre-morbid high-activity lifestyle.
This case presents the first documented instance, to our knowledge, of APS-associated LV fulfilling formal criteria for PJI on two separate occasions following TKA. Several features collectively point to a sterile, thrombo-inflammatory mechanism rather than true prosthetic infection. LV is a rare, relapsing thrombo-occlusive disorder of small dermal vessels that preferentially affects the lower extremities [6]. Its hallmark histologic findings (intraluminal fibrin deposition, hyalinization, and endothelial proliferation without vasculitic changes) distinguish it from infectious or inflammatory vasculitis. LV is strongly associated with prothrombotic states, with aPLs identified as the most frequent coagulation abnormality in several published series [6]. Under the 2023 ACR/EULAR APS classification criteria, biopsy-proven LV with small-vessel thrombosis qualifies as an established microvascular domain manifestation [7]. The thrombo-inflammatory pathophysiology of APS provides a mechanistic framework for the synovitis observed here. aPLs promote microvascular thrombosis and trigger a secondary neutrophil-mediated inflammatory cascade [8]. The synovial membrane, with its rich capillary network, is particularly susceptible to ischemic and inflammatory injury. Focal ischemia and cellular necrosis could account for the pronounced elevation in synovial WBC (>20,000 cells/µL, >93% neutrophils) and the positive α-defensin – a neutrophil-derived antimicrobial peptide – despite repeatedly negative cultures and NGS. Supporting this hypothesis, a 2024 proteomic study identified significantly elevated serum neutrophil defensin 1 in APS patients compared with controls [9]. A previous retrospective database study further documented that APS patients undergoing TKA face a significantly increased risk of thrombotic complications, underscoring the systemic vascular impact of this condition in the periarticular environment [10]. The α-defensin false-positive observed here is not without precedent. Plate et al. demonstrated that inflammatory rheumatic diseases, including crystal arthropathies, can yield false-positive α-defensin results, leading the authors to recommend its interpretation always in conjunction with clinical and microbiologic data [11]. Similarly, Jones et al. recently reported two cases of sterile inflammatory synovitis in rheumatoid arthritis patients after TKA that resolved without antimicrobials once infection was excluded [5]. The parallel in our case is notable: APS-driven thrombo-inflammatory synovitis, like rheumatoid arthritis flares, can generate neutrophil activation sufficient to trigger a positive α-defensin in the absence of any pathogen. The musculoskeletal manifestations of APS are broader than commonly recognized and include arthralgia, arthritis, avascular necrosis, and secondary erosive arthritis [12]. Secondary erosive arthritis has been reported in a patient with primary APS undergoing TKA, emphasizing that this syndrome can directly involve the joint [10,12]. Against this background, the recurrent inflammatory synovial responses documented here represent a distinct, and previously unreported, form of APS-mediated articular involvement that closely mimics PJI. The rapid and complete normalization of all synovial parameters following aspiration alone without antimicrobials provides compelling evidence against a persistent prosthetic infection. The sustained clinical remission at 12 weeks off therapy, while on low-dose aspirin, is consistent with observational data showing favorable responses to antiplatelet therapy in some LV patients, though anticoagulation remains guideline-directed therapy for thrombotic APS manifestations [13]. From a clinical standpoint, this case highlights several lessons. First, concurrent dermatologic lesions in PJI workups should never be dismissed. The ankle lesions present on both admissions provided the critical diagnostic clue. Second, persistent culture and NGS negativity should prompt active consideration of sterile inflammatory mimics before committing to repeat surgical intervention. Third, hypercoagulable and autoimmune serologies, including aPLs, warrant consideration in culture-negative PJI, particularly when concomitant thrombotic or skin manifestations are present.
APS–associated LV can produce recurrent thrombo-inflammatory sterile synovitis that satisfies published criteria for PJI, including markedly elevated synovial WBC and a positive α-defensin. Thorough evaluation of concomitant skin lesions, pursuit of advanced microbiologic testing (NGS), and serologic screening for hypercoagulable states are essential in culture-negative PJI cases. Recognition of this rare non-infectious mimic may spare patients from unnecessary revision surgery and prolonged antimicrobial exposure.
When culture-negative presumed PJI coincides with recurrent lower-extremity skin lesions, clinicians should consider biopsy of those lesions and screen for APS; a thrombo-inflammatory sterile mimic may be the unifying diagnosis and may resolve without surgical intervention.
References
- 1. Parvizi J, Gehrke T, Chen AF. Proceedings of the international consensus on periprosthetic joint infection. Bone Joint J 2013;95-B:1450-2. [Google Scholar] [PubMed]
- 2. Parvizi J, Tan TL, Goswami K, Higuera C, Della Valle C, Chen AF, et al. The 2018 definition of periprosthetic hip and knee infection: An evidence-based and validated criteria. J Arthroplasty 2018;33:1309-14.e2. [Google Scholar] [PubMed]
- 3. Parvizi J, Zmistowski B, Berbari EF, Bauer TW, Springer BD, Della Valle CJ, et al. New definition for periprosthetic joint infection: From the workgroup of the musculoskeletal infection society. Clin Orthop Relat Res 2011;469:2992-4. [Google Scholar] [PubMed]
- 4. Bonanzinga T, Ferrari MC, Tanzi G, Vandenbulcke F, Zahar A, Marcacci M. Inflammatory disorders mimicking periprosthetic joint infections may result in false-positive α-defensin. Int Orthop 2018;42:2271-5. [Google Scholar] [PubMed]
- 5. Jones C, Debenedetti A, Della Valle CJ. Sterile inflammatory synovitis as a mimic for prosthetic joint infection in patients with rheumatoid arthritis following total knee arthroplasty: A report of two cases. Cureus 2025;17:e78766. [Google Scholar] [PubMed]
- 6. Seguí M, Llamas-Velasco M. A comprehensive review on pathogenesis, associations, clinical findings, and treatment of livedoid vasculopathy. Front Med (Lausanne) 2022;9:993515. [Google Scholar] [PubMed]
- 7. Barbhaiya M, Zuily S, Naden R, Hendry A, Manneville F, Amigo MC, et al. The 2023 ACR/EULAR antiphospholipid syndrome classification criteria. Ann Rheum Dis 2023;82:1258-70. [Google Scholar] [PubMed]
- 8. Erkan D. Expert perspective: Management of microvascular and catastrophic antiphospholipid syndrome. Arthritis Rheumatol 2021;73:1780-90. [Google Scholar] [PubMed]
- 9. Wang Y, Li C. Proteomic analysis identifies neutrophil defensin 1 as a biological marker for antiphospholipid syndrome. Arthritis Rheumatol 2024;76 Suppl 9. (No page number) [Google Scholar] [PubMed]
- 10. Hirpara A, Carpenter M, Dayton M, Hogan C. Antiphospholipid syndrome increases postoperative complications after total hip and knee arthroplasty. Orthopedics 2024;47:301-7. [Google Scholar] [PubMed]
- 11. Plate A, Stadler L, Sutter R, Anagnostopoulos A, Frustaci D, Zbinden R, et al. Inflammatory disorders mimicking periprosthetic joint infections may result in false-positive α-defensin. Clin Microbiol Infect 2018;24:11. [Google Scholar] [PubMed]
- 12. Soltész P, Veres K, Lakos G, Kiss E, Muszbek L, Szegedi G. Plasma homocysteine and antiphospholipid antibodies as risk factors for thrombosis in patients with systemic autoimmune diseases. Lupus 2003;12:106-12. [Google Scholar] [PubMed]
- 13. Eswaran H, Googe P, Vedak P, Marston WA, Moll S. Livedoid vasculopathy: A review with focus on terminology and pathogenesis. Vasc Med 2022;27:593-603. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 One-Stage Revision for Low-Grade Periprosthetic Infection with Staphylococcus hominis Following Cruciate-Retaining Total Knee Arthroplasty: Case Report and Literature Review
June 1, 2026 One-Stage Revision for Low-Grade Periprosthetic Infection with Staphylococcus hominis Following Cruciate-Retaining Total Knee Arthroplasty: Case Report and Literature Review May 1, 2026 Diagnostic Accuracy of Synovial Alpha-Defensin and Histopathology for Periprosthetic Joint Infection: A Validation Study
May 1, 2026 Diagnostic Accuracy of Synovial Alpha-Defensin and Histopathology for Periprosthetic Joint Infection: A Validation Study January 1, 2026 A Step Beyond Convention: Three-Stage Revision with Limb Reconstruction System Fixator for Chronic Infected Total Knee Arthroplasty – A Case Report
January 1, 2026 A Step Beyond Convention: Three-Stage Revision with Limb Reconstruction System Fixator for Chronic Infected Total Knee Arthroplasty – A Case Report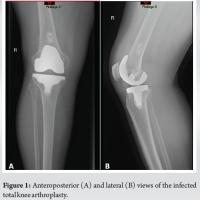 September 1, 2024 Case Reports: Periprosthetic Joint Infection after Total Joint Arthroplasty Following Swimming Activity
September 1, 2024 Case Reports: Periprosthetic Joint Infection after Total Joint Arthroplasty Following Swimming Activity