
Severe flexion contracture after TKA is rare but profoundly disabling. In selected patients with severe deformity and prolonged immobility, revision arthroplasty may be performed with palliative functional goals, prioritizing restoration of standing ability and basic ambulation rather than complete biomechanical reconstruction.
Dr. Asim Makhdom, Department of Orthopaedic Surgery, King Abdulaziz University, 7441 Al Mortada Street, Jeddah - 22252, Saudi Arabia. E-mail: amakhdom@kau.edu.sa
Abstract
Introduction: Flexion contracture following total knee arthroplasty (TKA) is an uncommon but debilitating complication that can result in profound functional limitation and reduced quality of life. Severe deformities after TKA are particularly challenging to manage, especially when associated with prolonged immobilisation and extensor mechanism disruption. In selected elderly patients with significant disability, the treatment goal may shift from anatomical reconstruction to restoration of basic function. To the best of our knowledge, severe bilateral flexion contractures approaching 75° following primary TKA have rarely been reported. This report highlights the concept of palliative revision arthroplasty aimed at improving function and quality of life rather than restoring normal knee biomechanics.
Case Report: A 78-year-old male presented with severe bilateral knee flexion contractures (75°) and inability to ambulate 8 months after bilateral primary TKA performed elsewhere. The post-operative course was complicated by patellar dislocation on the left side requiring revision surgery and prolonged immobilization. At presentation, the patient was wheelchair-bound with marked muscle atrophy and severe limitations in daily activities. Radiographs demonstrated well-fixed implants without loosening, and infection and neurological etiologies were excluded from the study. The patient underwent staged bilateral revision TKA using rotating hinged prostheses. Surgical correction required extensive synovectomy, posterior capsular release, distal femoral resection, gastrocnemius origin release, and extensor mechanism realignment with vastus medialis obliquus advancement. At 3 months following the second revision procedure, the flexion contractures improved from 75° preoperatively to 10° bilaterally. The patient regained the ability to stand and ambulate with assistance and reported marked improvement in comfort and ability to sleep.
Conclusion: Severe flexion contracture after TKA is rare but profoundly disabling. In selected patients with severe deformity and prolonged immobility, revision arthroplasty may be performed with palliative functional goals, prioritizing restoration of standing ability and basic ambulation rather than complete biomechanical reconstruction. Extensive soft-tissue releases combined with hinged implants can provide meaningful functional recovery and improved quality of life.
Keywords: Total knee arthroplasty, flexion contracture, revision knee arthroplasty, hinged knee arthroplasty.
Primary total knee arthroplasty (TKA) is a highly successful procedure for treating advanced arthritis, providing reliable pain relief and functional improvement [1]. However, complications such as stiffness and extensor mechanism disruption are devastating and can lead to severe functional limitations [2,3]. Flexion contracture following TKA is a challenging complication and may arise from multiple etiologies, including overstuffed implants, arthrofibrosis, prolonged immobilization, or rarely neurological disorders. Severe contractures can significantly impair activities of daily living, including standing and walking. In elderly patients with severe disability after TKA, the risk of surgical treatment may outweigh the benefits, and surgeons likely be hesitant to perform complex procedures without predictable outcomes. In this case report, we present a case of severe bilateral contractures (75°) after TKA, and the surgical goal was shifted from achieving perfect anatomical reconstruction to restoring basic function and improving quality of life. We discuss the concept of palliative revision TKA in select cases.
A 78 year-old male presented with severe bilateral knee flexion contractures and an inability to ambulate. Eight months before his presentation, he underwent bilateral TKA in another country. One month following the index surgery, the left knee was complicated by a patellar dislocation requiring revision TKA. It was revised with primary lateral release and repair by his former surgeon. The knee was subsequently immobilized for approximately 3 months. The patient reported progressive stiffness during the immobilization period, which evolved into severe bilateral flexion contractures. At presentation, he was wheelchair-bound and unable to stand or walk. In addition, he reported an inability to sleep comfortably due to the persistent flexed position of both knees. He also had a difficultly of performing basic hygiene activities independently. Medical history was significant only for well-controlled diabetes. Clinical examination demonstrated severe fixed flexion contractures in both knees. Bilateral muscle atrophy was evident in both lower extremities. Range of motion (ROM) was 75–110° in both knees with identical active and passive motion (Fig. 1).

Figure 1: Pre-operative clinical photographs demonstrating severe fixed flexion contractures of both knees, with the patient unable to achieve knee extension.
A palpable small defect of 1 cm was present over the quadriceps tendon of the left knee. Neurovascular examination was normal with intact distal pulses. Bilateral knee radiographs demonstrated well-fixed primary TKA implants bilaterally without signs of loosening (Fig. 2a,b,c,d).
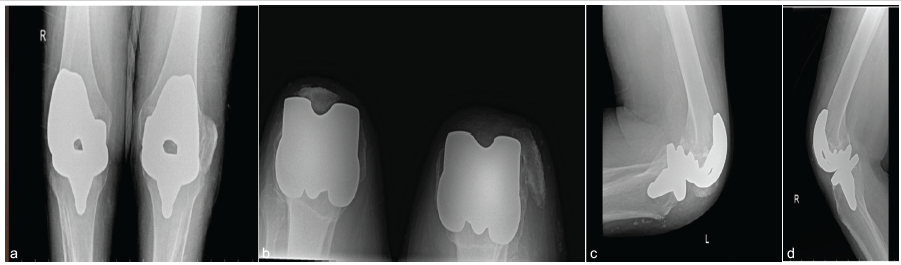
Figure 2: Pre-operative radiographic evaluation. (a) Bilateral anteroposterior radiographs demonstrating well-fixed total knee arthroplasty implants. Both knees in a flexed position. (b) Bilateral skyline views demonstrating dislocation of the left patella. (c) Lateral radiograph of the left knee showing the flexed knee position and patellar malalignment. (d) Lateral radiograph of the right knee demonstrating severe fixed flexion deformity.
The left patella was dislocated and in a distal position. Given the severity of the deformity, a neurological evaluation, including electromyography was obtained and had ruled out neuromuscular etiology of this severe contractures after TKA. In addition, laboratory markers were obtained to rule out possible subclinical infections, and both C-reactive protein and erythrocyte sedimentation rates were within normal. After a long discussion with the patient and his family, surgical revision was suggested while emphasizing that the ability to walk again independently is unlikely due to the severe muscle atrophy in both lower extremities and the prolonged period of immobilization.
Surgical technique:
The patient underwent staged bilateral revision TKA using hinged knee prostheses with an interval of 6 weeks between procedures. The surgical procedures were performed under general anesthesia. After the receiving standardized pre-operative antibiotic prophylaxis, the old incision was utilized. Correction of the severe flexion deformity required several surgical steps. Started with extensive synovectomy and removing scar tissues from the medial and lateral gutters as well as the suprapatellar pouch. This was followed with removing the polyethylene and femoral and tibial components. Extensive posterior capsular release was then carried out to improve extension. Even with that, the extension improved for 20° only. A stepwise distal femoral resection was performed and reached approximately 1 cm on each side to increase the extension gap, and both heads of the gastrocnemius muscle were then released at their femoral origins to achieve extension of 5° intraoperatively. Due to the extensor mechanism deficiency on the left side and dislocated patella, extensive lateral release was carried out, and vastus medialis obliquus (VMO) advancement was performed to improve patellar tracking and to augment extensor function [4]. Given the extensive soft-tissue releases, bilateral rotating hinged knee prostheses were used in these procedures to ensure adequate post-operative stability.
Post-operative care and outcome:
After the 1st revision (right knee), the patient was placed in an extension brace and was locked in full extension. Similarly, this was performed after the left knee revision and VMO advancement. He started progressive ROM and strengthening exercises with the physical therapy team focusing on his core, back, and lower extremity muscles 6 weeks after the second surgery. Post-operative radiographs showed excellent implant positions and marked improvement in knee extension (Fig. 3a,b,c,d).

Figure 3: Post-operative radiographs following staged bilateral revision total knee arthroplasty with rotating hinged prostheses. (a) Anteroposterior radiograph of the right knee. (b) Lateral radiograph of the right knee demonstrating improved knee extension and appropriate implant alignment. (c) Anteroposterior radiograph of the left knee. (d) Lateral radiograph of the left knee demonstrating restoration of knee alignment and correction of the flexion deformity.
At 3 months following the second revision procedure, the flexion contractures improved dramatically from 75° preoperatively to 10° bilaterally (Fig. 4). The patient regained the ability to stand and ambulate with assistance.

Figure 4: Post-operative clinical photographs demonstrating marked improvement in knee extension bilaterally, with significant correction of the pre-operative flexion contractures.
Importantly, he also reported that he could now sleep comfortably, which had not been possible before surgery due to the severe flexion deformities. At 1-year follow-up, the patient maintained functional ambulation with assistance.
Severe flexion contracture after TKA is uncommon but can result in profound disability [5]. Causes include arthrofibrosis, prolonged immobilisation, and occasionally neurological disease. In this patient, prolonged immobilisation likely led to progressive soft-tissue shortening and arthrofibrosis. The functional consequences of severe flexion deformity extend beyond impaired gait. Patients may become wheelchair-bound, and even basic activities such as resting comfortably could not be achieved. The patient was unable to sleep in a comfortable position due to the fixed deformities, highlighting the profound impact on quality of life. Correction of long-standing flexion contracture during revision TKA often requires a stepwise surgical strategy including synovectomy, posterior capsule release, distal femoral resection, gastrocnemius release, and use of constrained implants when stability is compromised. To the best of our knowledge, our case represents the most severe flexion contracture reported in the literature after TKA (75°). A similar case report of an 80-year-old man who had a progressive flexion contracture reached 60° after TKA [6]. It was revised with extensive soft-tissue releases and distal femoral resection up to 1 cm, and the patient has regained mobility. Several reports describe patients with severe flexion deformities who regained ambulation following arthroplasty. Hwang et al. [7] reported a 26-year-old female patient with rheumatoid knees with contractures approaching 90° who regained walking ability after primary TKA combined with extensive releases. Similarly, Abe et al. described rheumatoid patients with severe bilateral flexion contractures who were able to regain mobility following TKA [8]. However, all these reports were for contractures in a native knee and not after primary TKA. Although the posterior capsular release combined with distal femoral recut can substantially improve knee extension in most patients [9,10], in our case, the release of the gastrocnemius origins was necessary to contribute to an extension gain.
The use of hinged implants is particularly useful in complex revision scenarios where extensive soft-tissue releases compromise stability. Hinged prostheses provide intrinsic stability and allow safe correction of severe deformities [11]. The concept of palliative arthroplasty is relevant in these extremely rare situations. The goal may not be complete restoration of normal knee mechanics (e.g., restoration of joint line) but rather improvement of basic function and quality of life. In this case, the patient improved from being wheelchair bound with severe contractures to being able to walk with assistance and sleep comfortably, representing a significant functional benefit.
In this case with severe flexion contracture (> 75 degrees ) after TKA. Extensive soft tissues releases along with revision knee arthroplasty the use of hinged knee implants have achieved satisfactory outcome. The goal was not complete restoration of normal knee mechanics but rather improvement of basic function and quality of life.
Severe flexion contracture after TKA is rare but profoundly disabling. In selected patients with severe deformity and prolonged immobility, revision arthroplasty may be performed with palliative functional goals, prioritizing restoration of standing ability and basic ambulation rather than complete biomechanical reconstruction.
References
- 1. Tanzer M, Makhdom AM. Preoperative planning in primary total knee arthroplasty. J Am Acad Orthop Surg 2016;24:220-30. [Google Scholar] [PubMed]
- 2. Ritter MA, Lutgring JD, Davis KE, Berend ME, Pierson JL, Meneghini RM. The role of flexion contracture on outcomes in primary total knee arthroplasty. J Arthroplasty 2007;22:1092-6. [Google Scholar] [PubMed]
- 3. Vaishya R, Agarwal AK, Vijay V. Extensor mechanism disruption after total knee arthroplasty: A case series and review of literature. Cureus 2016;8:e479. [Google Scholar] [PubMed]
- 4. Matar HE, Illanes FL, Gollish JD. Extensive proximal extensor mechanism realignment for chronic patella dislocations in revision knee arthroplasty: Surgical technique. Knee 2020;27:1821-32. [Google Scholar] [PubMed]
- 5. Scuderi GR, Kochhar T. Management of flexion contracture in total knee arthroplasty. J Arthroplasty 2007;22 4 Suppl 1:20-4. [Google Scholar] [PubMed]
- 6. Kawashima SN, Yoshioka S, Toki S, Kashima M, Nakamura M, Chikaw T. Severe flexion contracture after total knee arthroplasty [Orthopaedic Proceedings] Boneandjointorguk; 2016. [Google Scholar] [PubMed]
- 7. Hwang YS, Moon KP, Kim KT, Kim JW, Park WS. Total knee arthroplasty for severe flexion contracture in rheumatoid arthritis knees. Knee Surg Relat Res 2016;28:325-9. [Google Scholar] [PubMed]
- 8. Abe S, Kohyama K, Yokoyama H, Matsuda S, Terashima Y, Nakagawa N, et al. Total knee arthroplasty for rheumatoid knee with bilateral, severe flexion contracture: Report of three cases. Mod Rheumatol 2008;18:499-506. [Google Scholar] [PubMed]
- 9. Kinoshita T, Hino K, Kutsuna T, Watamori K, Tsuda T, Horita Y, et al. Posterior capsular release improves intraoperative flexion contracture without affecting knee kinematics in posterior-stabilized total knee arthroplasty. J ISAKOS 2025;12:100848. [Google Scholar] [PubMed]
- 10. Sappey-Marinier E, Fernandez A, Shatrov J, Batailler C, Servien E, Huten D, et al. Management of fixed flexion contracture in primary total knee arthroplasty: Recent systematic review. SICOT J 2024;10:11. [Google Scholar] [PubMed]
- 11. Pasquier G, Ehlinger M, Mainard D. The role of rotating hinge implants in revision total knee arthroplasty. EFORT Open Rev 2019;4:269-78. [Google Scholar] [PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report
August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty
August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty July 1, 2026 Lipoma Arborescens of the Knee: An Intraoperative Mimicker of Pigmented Villonodular Synovitis in Bilateral Knee Osteoarthritis – A Case Report
July 1, 2026 Lipoma Arborescens of the Knee: An Intraoperative Mimicker of Pigmented Villonodular Synovitis in Bilateral Knee Osteoarthritis – A Case Report July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report
July 1, 2026 Megaprosthetic Total Knee Arthroplasty for Supracondylar Refracture in a Post-traumatic Osteoarthritic Knee: A Case Report