
Acute calcific periarthritis of the thumb can closely mimic infection, and characteristic imaging findings are essential to avoid unnecessary antibiotics or surgery.
Dr. Konstantinos G. Makiev, Department of Trauma and Orthopedics, University General Hospital of Alexandroupolis, St. Niarhos 1, Dragana, 68100, Alexandroupolis, Greece. E-mail: costasmakiev@gmail.com
Abstract
Introduction: Acute calcific periarthritis (ACP) is a self-limiting inflammatory condition most commonly involving the rotator cuff of the shoulder. Its presentation in the hand is rare and often mimics infectious processes, leading to potential misdiagnosis and inappropriate treatment. Prompt recognition through imaging is crucial for accurate diagnosis and management.
Case Report: We present a case report of a 84-year-old woman who presented with acute pain, swelling, and erythema of the right thumb. Clinical examination suggested an infectious etiology; however, plain radiographs were obtained to further evaluate the condition.
Results: Radiographic imaging revealed a well-defined, amorphous calcific deposit adjacent to the 1st metacarpophalangeal joint, consistent with ACP. No bony erosions or joint space narrowing was noted. Laboratory markers for infection were within normal limits. Under a digital nerve block, the patient underwent an ultrasound-guided barbotage procedure with needle aspiration and lavage, successfully removing most of the calcium deposits. A corticosteroid (triamcinolone) injection was then administered at the site. The patient experienced rapid symptom relief and full resolution within 2 weeks, without the need for antibiotics or surgical intervention.
Conclusion: ACP of the hand, although rare, should be considered in the differential diagnosis of acute monoarticular swelling, especially when infection is suspected but not supported by laboratory findings. Radiographic evaluation is pivotal for diagnosis and can prevent unnecessary interventions. This case highlights the importance of clinical-radiological correlation in recognising atypical presentations of ACP and reinforces its self-limiting nature with conservative management.
Keywords: Calcific tendonitis, hand, wrist, periarthritis, metacarpophalangeal.
Acute calcific periarthritis (ACP) is an inflammatory, self-limiting disorder most commonly found in the shoulder, particularly affecting the rotator cuff, but rarely involving the hand [1]. Also referred to as ‘calcareous periarthritis/tendinitis’ or ‘calcific/calcified tendinitis’, ACP affects men and women equally and typically presents with severe pain of rapid onset, often atraumatic in nature, accompanied by oedema, erythema, and limited range of motion of the affected joint [1,2]. The periarticular deposition of calcium hydroxyapatite crystals can be localised in tendons, peritendinous tissue, joint capsules, or collateral ligaments. Due to the superficial location of calcium deposits in the hand, inflammatory responses are more prominently manifested in the overlying skin and subcutaneous tissue, thus resembling other inflammatory aetiologies and leading to potential misdiagnosis [3]. Lack of familiarity with this condition, due to its rarity, has led to inappropriate management, like irrational use of antibiotics, unnecessary hospital admissions, and surgical procedures [4]. We present a rare case of ACP affecting the 1st metacarpophalangeal (MCP) joint of the thumb. The aim of the present report is to raise awareness of this pathology, emphasise its key characteristics, highlight the challenges associated with diagnosis, and provide insights by reviewing the relevant literature.
An 84-year-old woman presented to the Emergency Department with a three-day history of progressively worsening, excruciating pain in the right hand following exertion from housework. The patient denied any history of trauma, puncture wounds, fever, involvement of other joints, or prior systemic symptoms. Past medical history included hypertension and atrial fibrillation, while her family history was unremarkable. Physical examination revealed oedema and associated erythema extending across the volar and dorsal surfaces of the radial side of the hand and localised sensitivity to the 1st MCP joint (Fig. 1a and b).

Figure 1: (a) Clinical presentation of acute calcific periarthritis, characterized by prominent swelling and redness in the affected area, (b) clinical improvement with resolution of edema and erythema in the affected area.
There was also a restricted and painful range of motion, both active and passive, of the MCP and the interphalangeal (IP) joint of the right thumb. A palpable, soft, nodule-like mass was noted on the ulnar-volar aspect of the MCP joint. Laboratory testing demonstrated normal complete blood count and uric acid levels, while C-reactive protein was slightly elevated. Plain anteroposterior and oblique X-rays of the right hand displayed two well-defined calcified deposits at the volar aspect of the 1st MCP joint (Fig. 2a).
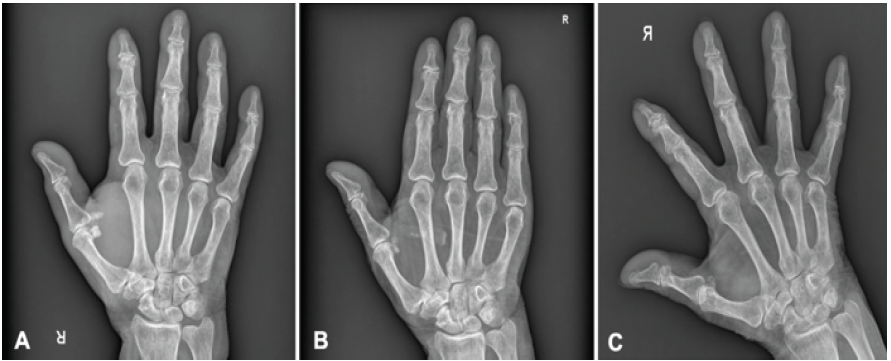
Figure 2: (a) Anteroposterior X-ray of the affected right hand showcasing calcifying deposits at the volar aspect of the metacarpophalangeal (MCP) joint of the thumb, (b) comet-like pattern of calcification spread, aligned with the muscle fibers of the adductor pollicis at 2-weeks follow up (c) no residual calcification at the first MCP joint and complete disappearance of the comet-like calcification pattern at the 6-week follow-up.
The patient was admitted to the orthopaedic department for further investigation and management. On admission, the patient rated her pain as 8 on the visual analogue scale (VAS). Systemic intravenous analgesics and non-steroidal anti-inflammatory drugs were initiated as first-line treatment. On the 1st day post-admission, a musculoskeletal ultrasound of the affected first ray was performed. The ultrasound probe was positioned longitudinally over the ulnar side of the 1st MCP joint to visualise the long axis of the larger calcific deposit according to the X-ray. A hyperechoic, homogeneous, ellipsoid, well-circumscribed peritendinous deposit with posterior acoustic shadowing could be clearly visualised at the insertion of the adductor pollicis muscle (Fig. 3).
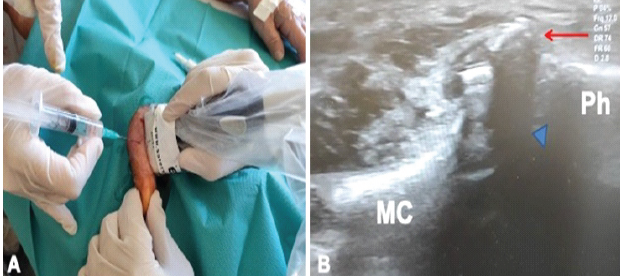
Figure 3: (a) Ultrasound-guided barbotage of the calcific deposits of the 1st metacarpophalangeal (MCP) joint, (b) Ultrasound image-longitudinal axis of the 1st MCP joint, red arrow is demonstrating the calcification, blue arrowhead is depicting the acoustic shadow over the 1st MCP joint. MC: Metacarpal, Ph: Phalanx.
No fluid effusion in the flexor tendon sheaths or intra-articular pathology of the MCP joint was denoted. Under a digital nerve block, an ultrasound-guided barbotage procedure was performed, effectively removing the majority of the calcium deposits through needle aspiration and lavage. Following this, a corticosteroid injection (triamcinolone) was administered to the site of the calcification. After 24 h, the patient’s pain was reassessed and reported as a 3 on the VAS, accompanied by a reduction in oedema and erythema in the affected right hand. Active flexion of the MCP joint of the thumb was possible but painful, limited to 20°. In contrast, flexion of the IP joint was pain-free and exhibited a full range of motion. The patient was discharged with instructions for oral anti-inflammatory medication, elevation of the right upper limb with a sling, and a follow-up appointment at the outpatient clinic. At the 2-week follow-up, oedema and erythema had fully subsided, with only minimal residual sensitivity during the active range of motion of the MCP joint, which remained limited to 20°. A repeat X-ray demonstrated a near-complete resolution of the calcific deposits at the MCP joint but revealed a spread of calcification in a comet-like pattern, aligned with the muscle fibres of the adductor pollicis (Fig. 2b). At the 6-week follow-up, the patient demonstrated a full, symmetrical range of motion in adduction, abduction, flexion, and extension of the 1st MCP joint (Fig. 4), with a VAS pain score of 0.
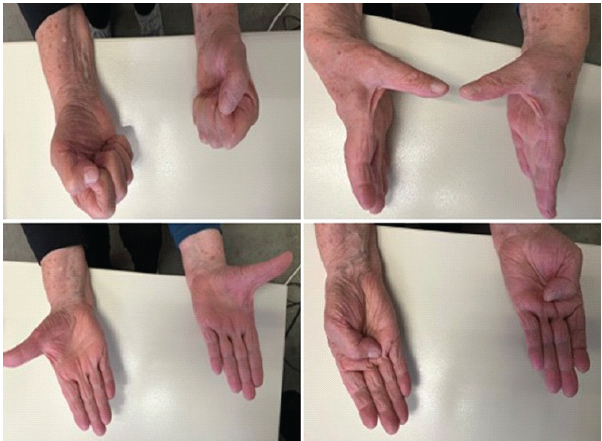
Figure 4: Patient demonstrating full range of motion of the metacarpophalangeal and proximal interphalangeal joint of the thumb at 6 week follow-up.
The final radiograph showed no residual calcification at the 1st MCP joint and complete disappearance of the comet-like calcification pattern that was initially observed immediately after the barbotage procedure (Fig. 2c).
ACP of the hand was first described by Cohen in 1924 [5]. Since then, only a few studies of ACP concerning either the wrist or the hand have been published. Sandstorm, after reviewing 329 cases of calcium deposits, reported that ACP involved the wrist or the hand in 2.4% of these cases [6]. However, the true incidence of this pathology is hard to estimate precisely, due to its self-limiting nature and, more importantly, its rarity. The joints most commonly affected are those adjacent to the insertion site of the flexor carpi ulnaris. Furthermore, ACP of MCP and distal and proximal IP joints of the fingers have also been described (Fig. 5) [1,3].

Figure 5: Illustration showcasing the typical sites of calcific deposits in the hand. Flexor carpi ulnaris is the most common site of calcification in the hand, followed by metacarpophalangeal, proximal interphalangeal and distal interphalangeal joints. Acute calcific periarthritis at the wrist primarily concerns flexor or extensor tendons, whereas in digits, they usually involve the ligamentous structures. Intrinsic muscles are typically affected, when these occur within the palm.
It appears that calcium deposits at the wrist primarily concern flexor or extensor tendons, whereas in digits, they are usually found in the ligamentous structures. In contrast, intrinsic muscles are the most common site of calcification when they occur within the palm [3]. Nevertheless, involvement of the 1st MCP is extremely rare, and none of the available studies concerned the adductor pollicis insertion site, as reported in this case [7,8]. Endocrine disorders such as diabetes mellitus and thyroid dysfunction, as well as genetic predisposition, have been associated with a higher susceptibility for developing calcific tendinopathy [9]. To date, several theories have been proposed regarding its pathophysiology, including reactive calcification, endochondral ossification, and chondral metaplasia. However, the precise mechanism by which the tendon is calcified remains unclear [10]. Reactive calcification, as described by Uthoff et al., describes calcium deposition as a cell-mediated process that can be divided into four phases. The pre-calcific first phase is characterised by fibrocartilaginous metaplasia of the tendon. The formative second phase is represented by the formation of cell-mediated calcific deposits by chondrocytes. In the resorptive third phase, phagocytes penetrate the area and absorb the calcium. When the calcium dissolves, a localised inflammation is generated, causing pain and other clinical features. The final post-calcific fourth phase allows for the restoration of the normal collagen pattern [11]. In endochondral ossification, like in cases of insertional Achilles and patellar tendinopathy, the calcification process mimics physiologic endochondral bone formation, characterised by chondrocyte-like cells, increased types II, III, and X; and reduced type I collagen. Another supported theory is that improper differentiation of tendon-derived stem cells into chondrocytes or osteoblasts rather than tenocytes, under the influence of certain proteins (bone morphogenetic proteins, biglycan/fibromodulin), can lead to chondral metaplasia [12]. ACP in the hand affects males and females equally. While the age of patients at presentation typically ranges from 30 to 60 [3,7], singular paediatric cases have also been reported [13]. The main complaint is sudden and acute pain in the wrist or the hand. Usually, patients are not able to recall any specific injury or strain, and a history of precipitating trauma is only mentioned in one third of the cases [3,14]. Tenderness is well-localised, often marked by a specific spot of maximal pain. Typical findings are severe oedema with associated erythema and impaired range of motion of the affected joint [15]. Clinical presentation resembles various pathologies such as fracture or dislocation, infections (cellulitis, septic arthritis, and tenosynovitis), and inflammatory arthritis (gout, psoriasis) [1,7]. This overlap complicates the differential diagnosis, contributing to high rates of misdiagnosis, which range from 58% to 70%, and subsequently leads to inappropriate management such as unnecessary surgical exploration, irrational use of antibiotics, and avoidable hospitalisations. High suspicion is imperative for the prompt and accurate diagnosis of ACP in the hand and to avoid further mismanagement, as laboratory findings may resemble those of other pathologies [14]. Radiographic examination plays a crucial role, as the identification of distinct, homogeneous juxta-articular densities without trabeculae or cortex is pathognomonic of ACP [7]. However, care should be taken not to mistake them for an avulsion fracture or accessory ossicle. Moreover, ultrasound can help exclude infective processes such as tenosynovitis and also identify calcifications, which are depicted as hyperechogenic structures with or without acoustic shadow [1]. ACP is a self-limiting condition in which the initial acute pain subsides substantially after 3–4 days, even without treatment [3,16]. Typically, it takes around 3 weeks for both symptoms and calcifications to resolve completely, but in some instances, complaints have persisted for months [1,3]. Carroll, in the largest available series, demonstrated that providing any form of treatment significantly decreases the duration of symptoms. Particularly, after the injection of local anaesthetic with or without corticosteroids, complete cessation of pain was attained within an average of 9 days. In contrast, when no treatment was implemented, 20 days on average were needed for the symptoms to resolve [3]. This can be explained by the fact that fluid injections can help dissolve calcium deposits, facilitate calcium resorption, and thus reduce local inflammation more promptly [15]. However, migration of the calcification within the belly of the affected muscle after aspiration, lavage, and injection, as observed in this case, has never been described before. Even though it did not affect or complicate the course of the condition, clinicians should be aware of this phenomenon as well and closely monitor the patient. Other conservative treatment modalities include warm water soaks, splint immobilisation, and non-steroidal anti-inflammatory drugs. Surgery is rarely indicated and is reserved only for persistent cases of ACP that do not respond to the aforementioned therapeutic options [13,17].
ACP of the 1st MCP joint is an extremely rare condition. Clinical presentation resembles various other pathologies. Therefore, high suspicion is essential for the accurate diagnosis and to avoid unnecessary interventions. Characteristic radiographic findings can assist in confirming the condition. Due to its self-limiting nature, most cases resolve spontaneously with conservative treatment, and surgery is rarely indicated.
Acute calcific periarthritis of the thumb should be considered in patients with acute monoarticular swelling and erythema of the hand, particularly when inflammatory markers do not support infection; early radiographic recognition can prevent unnecessary antibiotics, hospitalisation, or surgery.
References
- 1. Schneider D, Hirsch M. Acute calcific tendonitis of dorsal interosseous muscles of the hand: Uncommon site of a frequent disease. Reumatismo 2017;69:43-6. [Google Scholar] [PubMed]
- 2. Selby CL. Acute calcific tendinitis of the hand: An infrequently recognized and frequently misdiagnosed form of periarthritis. Arthritis Rheum 1984;27:337-40. [Google Scholar] [PubMed]
- 3. Carroll RE, Sinton W, Garcia A. Acute calcium deposits in the hand. J Am Med Assoc 1955;157:422-6. [Google Scholar] [PubMed]
- 4. Nikci V, Doumas C. Calcium deposits in the hand and wrist. J Am Acad Orthop Surg 2015;23:87-94. [Google Scholar] [PubMed]
- 5. Cohen I. Calcareous deposit at the insertion of flexor carpi ulnaris tendon following trauma. Trauma Am J Surg 1924;38:172-3. [Google Scholar] [PubMed]
- 6. Sandstrom C. Peritendinitis calcarea; A common disease of middle life: Its diagnosis, pathology and treatment. Am J Roentgenol Radium Ther 1939;40:1-21. [Google Scholar] [PubMed]
- 7. Zribi W, Jmal MM, Abid A, Ben Jemaa M, Krid N, Zribi M, et al. Apatite calcific periarthritis of the radial collateral ligament of the thumb: A case report and review of the literature. Case Reports Plast Surg Hand Surg 2019;6:92. [Google Scholar] [PubMed]
- 8. Friedman SN, Margau R, Friedman L. Acute calcific periarthritis of the thumb: Correlated sonographic and radiographic findings. Radiol Case Rep 2017;13:205-7. [Google Scholar] [PubMed]
- 9. Senthilkumaran S, Ledingham WM. Enveloping calcification of flexor digitorum profundus tendon: A diagnosis easily missed. BMJ Case Rep 2020;13:e233510. [Google Scholar] [PubMed]
- 10. Oliva F, Via AG, Maffulli N. Calcific tendinopathy of the rotator cuff tendons. Sports Med Arthrosc Rev 2011;19:237-43. [Google Scholar] [PubMed]
- 11. Uhthoff HK, Loehr JW. Calcific tendinopathy of the rotator cuff: Pathogenesis, diagnosis, and management. J Am Acad Orthop Surg 1997;5:183-91. [Google Scholar] [PubMed]
- 12. Oliva F, Via AG, Maffulli N. Physiopathology of intratendinous calcific deposition. BMC Med 2012;10:95. [Google Scholar] [PubMed]
- 13. Walocko FM, Sando IC, Haase SC, Kozlow JH. Acute calcific tendinitis of the index finger in a child. Hand (N Y) 2016;12:NP84. [Google Scholar] [PubMed]
- 14. Dimmick S, Hayter C, Linklater J. Acute calcific periarthritis-a commonly misdiagnosed pathology. Skeletal Radiol 2022;51:1553-61. [Google Scholar] [PubMed]
- 15. Torbati SS, Bral D, Geiderman JM. Acute calcific tendinitis of the wrist. J Emerg Med 2013;44:352-4. [Google Scholar] [PubMed]
- 16. Munjal A, Munjal P, Mahajan A. Diagnostic dilemma: Acute calcific tendinitis of flexor digitorum profundus. Hand (N Y) 2013;8:352-3. [Google Scholar] [PubMed]
- 17. Harris AR, McNamara TR, Brault JS, Rizzo M. An unusual presentation of acute calcific tendinitis in the hand. Hand (N Y) 2008;4:81-3. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2025 Induced Membrane Wrist Fusion with Ring External Fixator Assistance in a Mangled Upper Extremity: A Case Report
May 1, 2025 Induced Membrane Wrist Fusion with Ring External Fixator Assistance in a Mangled Upper Extremity: A Case Report May 1, 2026 Reawakening of a Giant Cell Bone Tumor after 40 Years of Silence: A Rare Case Report
May 1, 2026 Reawakening of a Giant Cell Bone Tumor after 40 Years of Silence: A Rare Case Report February 1, 2026 A Rare Case: Septic Arthritis of The Wrist
February 1, 2026 A Rare Case: Septic Arthritis of The Wrist January 1, 2026 Enhancing Functional Outcomes in Distal End Radius Fracture Rehabilitation
January 1, 2026 Enhancing Functional Outcomes in Distal End Radius Fracture Rehabilitation