
Bipolar clavicle fractures are rare, often misdiagnosed segmental injuries that require a high index of clinical suspicion, comprehensive imaging including 3D CT for surgical planning, and dual-plate fixation to ensure stable fracture union and restore optimal shoulder biomechanics.
D Naveen Kumar, Department of Orthopaedics, Parvathy Hospital, No. 23, Garden Street, VGN Monte Carlo, Gurusamy Road, Nolambur, Chennai - 600 095, Tamil Nadu, India. E-mail: nknaveenkarthik@gmail.com
Abstract
Introduction: Bipolar clavicle fractures are a simultaneous injury to both ends of the clavicle and represent an exceptionally rare entity with an incidence of <1% of all clavicle fractures. Despite the clavicle being one of the most commonly fractured bones, involvement of both ends is frequently missed or misdiagnosed, leading to complications like persistent pain and compromised function. The rarity of these fractures has also led to a significant gap in established treatment guidelines. We present a case of a bipolar clavicle fracture with sternoclavicular joint dislocation treated successfully with dual-plate surgical fixation.
Case Report: A 65-year-old male presented to the emergency department following a road traffic accident with injury to the left shoulder. Clinical examination revealed diffuse swelling and tenderness over both medial and lateral ends of the clavicle. Radiographic evaluation showed fractures at both ends with sternoclavicular joint dislocation. The patient underwent open reduction and internal fixation with dual-plate osteosynthesis, a lateral end clavicle plate for the lateral fracture, and a double contoured distal fibula locking plate for the medial fracture and joint dislocation. The patient achieved solid bony union at both fracture sites with excellent functional recovery at 12 weeks.
Conclusion: Bipolar clavicle fractures require high clinical suspicion and comprehensive imaging for accurate diagnosis. Surgical management with dual-plate fixation provides superior fracture stability and functional outcomes. This case emphasises the importance of educating orthopaedic surgeons and emergency physicians about this quaint injury pattern to prevent missed diagnoses and associated morbidity.
Keywords: Bipolar clavicle fracture, sternoclavicular dislocation, dual-plate osteosynthesis.
Clavicle fractures are among the most common fractures encountered in orthopaedic practice, accounting for approximately 2.6–4% of all fractures and representing 35–44% of shoulder girdle injuries [1,2]. The middle third of the clavicle is most frequently affected (69–82%), followed by the lateral third (21–28%), and then the medial third (2–3%) [3,4]. Bipolar clavicle fractures are defined as simultaneous fractures and/or dislocations involving both the medial and lateral ends of the clavicle and represent an exceptionally rare injury pattern with an estimated incidence of <1% of all clavicle fractures [5,6]. The first case of bipolar clavicle fracture was described by Porral in 1831, and since then, fewer than 100 cases have been documented in the literature [7,8]. The rarity of this injury, combined with its atypical presentation and the tendency for emergency physicians to focus on the more obvious injuries, frequently results in a missed or delayed diagnosis [9,10]. This diagnostic oversight eventually leads to complications, such as persistent pain, functional impairment, compromised shoulder biomechanics, neurovascular complications, and non-union [11,12]. The mechanism of injury typically involves a high-energy trauma, with forces applied to both ends of the clavicle, either simultaneously or sequentially [13]. Common mechanisms include motor vehicle accidents, falls from height, and direct blows to the shoulder girdle [14,15]. The clavicle acts as a strut connecting the axial skeleton to the upper extremity, and when subjected to extreme forces at both articulations, it can fail at multiple points [16]. Despite increasing recognition of this injury pattern over the past two decades, there remains no established consensus regarding optimal treatment protocols [17]. We present a case of a bipolar clavicle fracture with sternoclavicular joint dislocation treated successfully with dual-plate surgical fixation, highlighting the diagnostic challenges, surgical technique, and the resultant functional outcome at 2-year follow-up. This case contributes to the limited literature on this rare entity and advocates for surgical management to achieve optimal outcomes.
A 65-year-old male, with no known comorbidities, presented to the emergency department following a skid and fall from a two-wheeler. The patient sustained initial impact on the left lateral aspect of the shoulder and the head, followed by a secondary impact when falling to the ground on the medial side of the shoulder. The patient complained of severe left shoulder pain, inability to elevate the arm, and difficulty with any shoulder movement. There was no history of previous shoulder injuries, surgeries, or pre-existing shoulder pathology. Clinical examination revealed diffuse swelling and tenderness over both medial and lateral ends of the left clavicle. There was a visible deformity and prominence over the medial aspect, suggestive of sternoclavicular joint disruption. Skin tenting was noted over the lateral fracture site. The active range of motion was limited due to pain. There were no neurovascular deficits. Plain radiographs of the left shoulder revealed displaced fractures of the medial and lateral ends of the clavicle (Fig. 1).
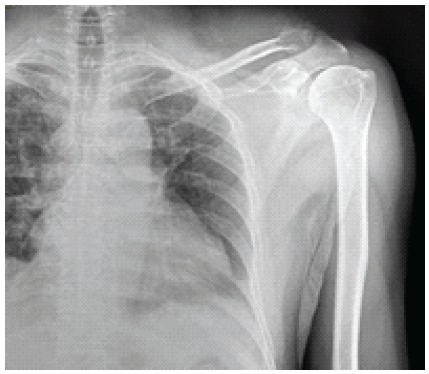
Figure 1: Anteroposterior radiograph of the left shoulder in a 66-year-old male patient demonstrating a bifocal clavicle fracture with sternoclavicular joint dislocation.
Three-dimensional computed tomography (3D CT) confirmed a fracture at the junction of the lateral and middle thirds with superior and posterior displacement of the lateral fragment, along with a medial clavicle fracture with anterior dislocation of the sternoclavicular joint (Figs. 2 and 3).
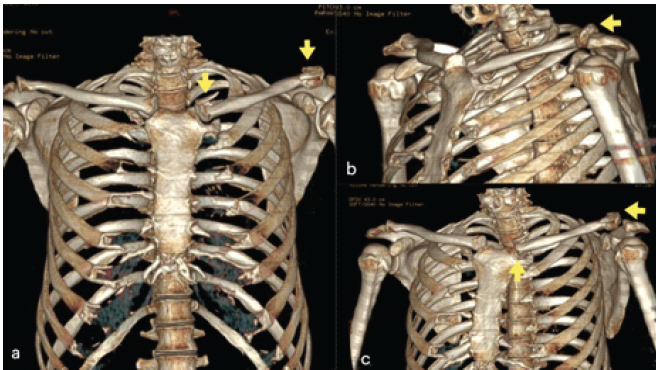
Figure 2: Three-dimensional computed tomography reconstruction demonstrating a bifocal left clavicle fracture with sternoclavicular joint dislocation. (a) Anterior coronal view showing the medial end clavicle fracture with sternoclavicular joint dislocation (thick arrow) and the displaced lateral end clavicle fracture (thin arrow). (b) Oblique superior view of the left shoulder girdle highlighting the displaced lateral end clavicle fracture (arrow) with superior displacement of the fracture fragment. (c) Anterior oblique view illustrating both the lateral clavicle fracture (lateral arrow) and the medial sternoclavicular dislocation (inferior arrow).
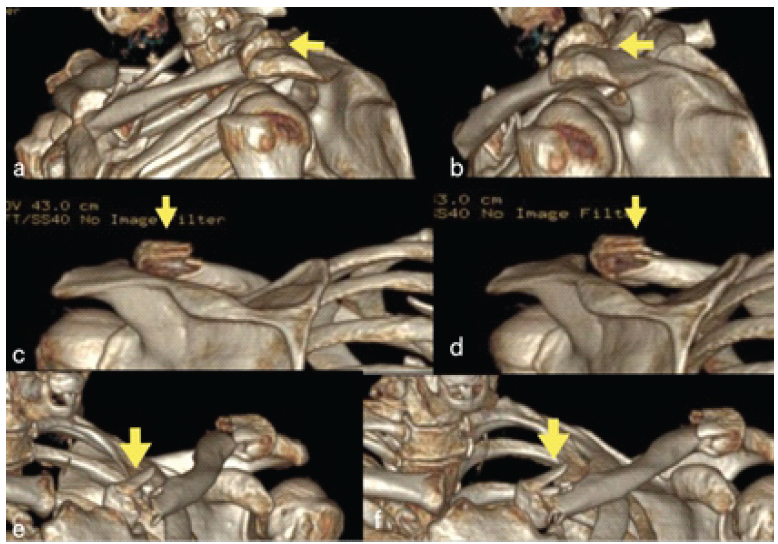
Figure 3: (a) Anterior oblique view showing the displaced lateral end clavicle fracture (arrow). (b) Close-up anterior oblique view further delineating the lateral clavicle fracture fragment (arrow) and its postero-superior displacement. (c) Superior axial view demonstrating the full extent of the clavicular injury with the medial fracture and sternoclavicular disruption (arrow). (d) Superior axial close-up view confirming the medial end displacement (arrow) and the loss of sternoclavicular joint congruity. (e) Inferior oblique view highlighting the medial anterior clavicle fracture-dislocation (arrow). (f) Posterior oblique view showing the sternoclavicular joint dislocation (arrow).
Under general anaesthesia, with the patient in the supine position, a 6 cm long incision was made along the lateral end of the clavicle, centring the fracture site. The suprascapular nerve was identified and protected (Fig. 4).
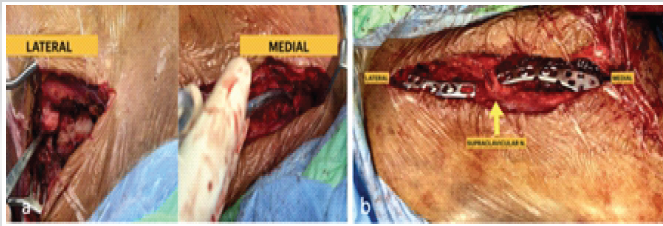
Figure 4: Intraoperative photographs demonstrating (a) Lateral and medial fracture ends. (b) Post-fixation view showing dual plate osteosynthesis with anatomically contoured locking plates applied to both the lateral and medial fracture sites, and isolated supracalvicular nerve.
Once the fracture was reduced, it was provisionally fixed using a 2 mm K-wire. A pre-contoured lateral end clavicle locking plate (6-hole) was used to fix the fracture and was placed along the superior surface of the clavicle. A separate 7 cm medial incision allowed for the reduction of the fracture and the sternoclavicular dislocation. To accommodate the complex anatomy and protect mediastinal structures, a double-contoured distal fibula locking plate was applied to the anterosuperior surface. Intraoperative fluoroscopy confirmed anatomical reduction and safe hardware placement, specifically ensuring no posterior cortex penetration to protect retrosternal structures (Fig. 5).
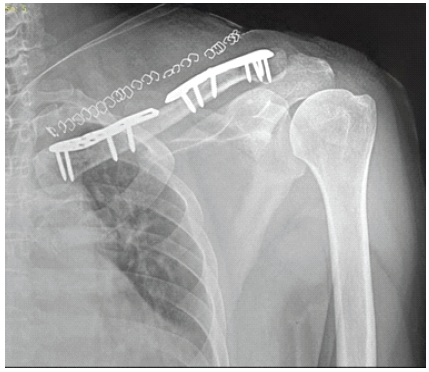
Figure 5: Immediate post-operative anteroposterior radiograph of the left shoulder demonstrating satisfactory open reduction and internal fixation of the bifocal left clavicle fracture with sternoclavicular joint dislocation.
Postoperatively, the patient was immobilized in a sling for 4 weeks while beginning immediate Codman pendulum exercises, followed by progressive functional rehabilitation. Clinical and radiographic follow-ups were conducted at 2 weeks, 6 weeks, 3, 6, 12, and 24 months (Fig. 6). By 6 months, bony union was achieved at both sites, and the patient regained a full range of motion, returning to all pre-injury activities (Fig. 7 and 8).
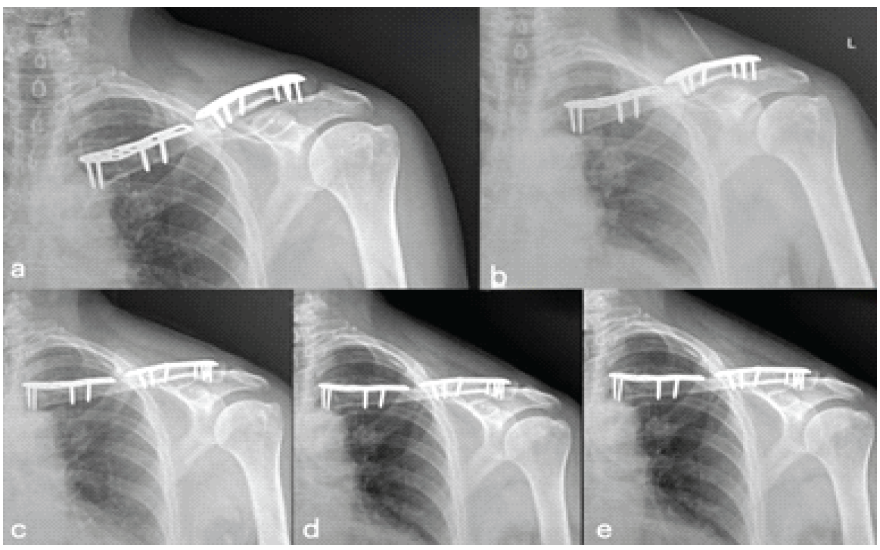
Figure 6: Serial post-operative anteroposterior radiographs of the left shoulder at (a) 1-month follow-up: Early periosteal reaction is noted at the fracture sites. (b) 2-month follow-up: Progressive callus formation visible at both fracture sites. (c) 3-month follow-up: Advancing fracture consolidation with increasing callus density at both medial and lateral fracture sites. (d) 6-month follow-up: Near-complete radiological union at both fracture sites with mature bridging callus. (e) 24-month follow-up: Complete radiological union achieved at both fracture sites. Dual plate construct intact with no signs of implant failure, screw loosening, or osteolysis.

Figure 7: Clinical photographs at 24-month follow-up demonstrating (a) well-healed, mature surgical scar along the clavicular incision with no signs of wound dehiscence, implant prominence, or keloid formation. (b) excellent functional outcome with full bilateral shoulder range of motion with symmetric overhead elevation.
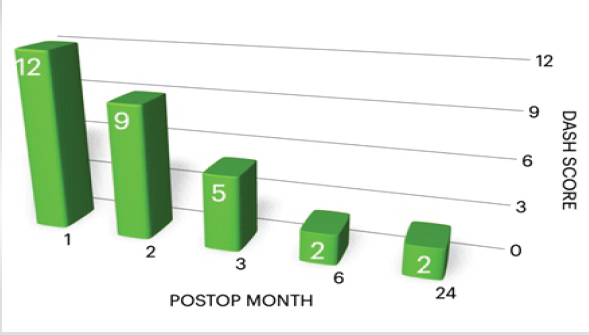
Figure 8: Bar graph illustrating the serial disabilities of the arm, shoulder, and hand scores at post-operative follow-up intervals of 1, 2, 3, 6, and 24 months
Since the first description of bipolar clavicle fractures by Porral in 1831 as “double luxation de la clavicule”, the literature has remained sparse. These injuries are prone to being missed or misdiagnosed. Data from Kumar AS et al. show that the rarity of these cases, often representing less than 1% of clavicle injuries, contributes to diagnostic oversight in emergency departments [18]. A comprehensive review by Thuan et al. updated the historical context of these documented cases, spanning from the 19th century to the modern era [8]. This rarity has also led to a lack of consensus regarding the optimal treatment protocol. The mechanism of injury in our patient, with initial lateral impact followed by medial ground impact, is consistent with high-energy trauma patterns recently analysed by Bakir et al. and Sandler et al., where sequential forces lead to multi-segmental failure [13,15].
- In our case, both injuries were identified on radiographs due to a high index of suspicion, which was supported by 3D CT. This is consistent with current recommendations advocating for advanced imaging in all complex shoulder girdle injuries to ensure accurate surgical planning and avoid the “missed” bipolar fracture described by Xiong J et al. [9,10].
- The optimal management of bipolar clavicle fractures remains controversial. While some earlier reports suggested success with non-operative management for minimally displaced fractures [19,20], evidence from Scalise JJ et al. acknowledges that significant displacement or risk of non-union necessitates surgical intervention to avoid long-term functional impairment [11,21].
To restore biomechanical function and allow early mobilisation, several authors advocate for dual-plate fixation. Sono et al. have reported improved outcomes using operative approaches for complex fractures [21]. Regarding hardware, while some studies utilised standard reconstruction plates, newer literature suggests specialised, clavicle-specific plates to better match the bone’s unique anatomy and provide robust stability [22,23]. In our case, we achieved stable fixation by using a lateral end clavicle plate for the lateral fracture. For the medial fracture and anterior sternoclavicular dislocation, we innovatively employed a double-contoured distal fibula locking plate. This provided robust stability while respecting the complex medial anatomy. We directed screws anterolaterally to avoid the retrosternal risks associated with the vital structures located posterior to the medial clavicle. [24,25] Our patient achieved excellent functional outcomes with a disabilities of the arm, shoulder, and hand score of 0 at the final follow-up, mirroring the high satisfaction rates reported in recent surgical series [26,27]. While conservative management can lead to higher non-union rates (up to 15–20% in some series), our patient achieved complete radiological union by 6 months [12,28]. This recovery timeline is similar to the rapid union seen in other recent case studies of surgical fixation in older populations [29,30]. We were successful in avoiding complications like hardware failure or the chronic pain often described in missed cases [10,11]. Our complication-free 24-month follow-up highlights the benefits of anatomical reduction in these rare segmental injuries.
Bipolar clavicle fractures are rare injuries requiring high clinical suspicion and 3D CT for diagnosis. To avoid morbidity, the entire clavicle must be evaluated whenever a single fracture is identified. Based on our experience and current literature, we conclude that surgical management with dual-plate fixation is superior to conservative or single-site approaches. This technique restores the clavicle’s biomechanical strut function, providing the stability necessary for early mobilisation and excellent functional recovery. Ultimately, early recognition combined with individualised internal fixation remains the cornerstone for successful outcomes and the prevention of chronic instability.
Suspect “quaint” or subtle bipolar injuries in high-energy shoulder trauma. Early surgical intervention with stable dual-plate fixation leads to excellent functional recovery and restores shoulder biomechanics.
References
- 1. Robinson CM. Fractures of the clavicle in the adult: epidemiology and classification. J Bone Joint Surg Br. 1998;80(3):476-484. [Google Scholar] [PubMed]
- 2. Gottschalk HP, Browne RH, Starr AJ. Shoulder girdle: patterns of trauma and associated injuries. J Orthop Trauma. 2011 May;25(5):266-71. [Google Scholar] [PubMed]
- 3. Bartosz K, Aleksander J, Konrad K, Aleksandra H, Łukasz M, Maciej Z, et al. Clavicle fractures – epidemiology, biomechanics of injury and treatment methods. Journal of Education, Health and Sport.2023;14:216-232. [Google Scholar] [PubMed]
- 4. Kumar ASA, Bidhu B, Kumar GR, Harikrishnan V. Bipolar Clavicle Fracture in Elderly: A Rare Case Report. J Orthop Case Rep. 2026 Feb;16(2):58-62. [Google Scholar] [PubMed]
- 5. Feng D, Jiang W, Kang X, Jiang Y, Zhu Y, Zhang J. Simultaneous bilateral traumatic clavicle fractures: incidence, characteristics, and surgical outcomes. BMC Musculoskelet Disord. 2023 Feb 10;24(1):112. [Google Scholar] [PubMed]
- 6. Grossi EA. SEGMENTAL CLAVICLE FRACTURE. Rev Bras Ortop. 2015 Nov 16;46(6):733-5. [Google Scholar] [PubMed]
- 7. Porral, A. (1831) Case Report of a Double Dislocation of the Right Clavicule Bone. Medical and Practical Surgery Journal, 2, 78-82. [Google Scholar] [PubMed]
- 8. Thuan Ly AM, Beall MS 3rd, Sraj SA. Bipolar clavicular fractures and treatment options. Eur J Trauma Emerg Surg. 2021;47(5):1407-1410. [Google Scholar] [PubMed]
- 9. Xiong J, Huang Z, Rui Y. Delayed diagnosis of a combined medial and lateral clavicle fracture: case report and review of literature. BMC Musculoskelet Disord. 2020;21(1):541. [Google Scholar] [PubMed]
- 10. Heinz SM, ElKhouly AS, Marwan Y, Al-Arabi AA, Esmaeel AA. Delayed presentation of bipolar clavicle fracture: a case report and review of literature. Case Rep Orthop. 2018;2018:7245914. [Google Scholar] [PubMed]
- 11. Scalise JJ, Iannotti JP, Marra G, Kilicoglu O, Rosenberg RE. Nonoperative treatment of bipolar clavicle fractures. J Shoulder Elbow Surg. 2008;17(4):551-554. [Google Scholar] [PubMed]
- 12. Goudie EB, Clement ND, Murray IR, Lawrence CR, Brooksbank AJ, Robinson CM. The changing pattern of clavicle fractures in adults: a 20-year study of a single center. J Orthop Trauma. 2017;31(11):565-571. [Google Scholar] [PubMed]
- 13. Bakir MS, Carbon R, Ekkernkamp A, Schulz-Drost S. Monopolar and bipolar combination injuries of the clavicle: retrospective incidence analysis and proposal of a new classification system. J Clin Med. 2021;10(24):5764. [Google Scholar] [PubMed]
- 14. Orecchia LM, Giordano MB, Giordano M. Epidemiology and management of shoulder girdle injuries in polytrauma patients. Injury. 2024;55(2):111241. [Google Scholar] [PubMed]
- 15. Sandler B, Baird MD, Scanaliato JP. Incidence of sports-related sternoclavicular joint dislocations in the United States over the last two decades. World J Orthop. 2023;14(6):427-435. [Google Scholar] [PubMed]
- 16. Huang JI, Toogood P, Chen MR, Wilber JH, Cooperman DR. Clavicular anatomy and the applicability of precontoured plates. J Bone Joint Surg Am. 2007;89(10):2260-2265 [Google Scholar] [PubMed]
- 17. McKee MD, Wild LM, Schemitsch EH. Midshaft malunions of the clavicle. J Bone Joint Surg Am. 2003;85(5):790-797. [Google Scholar] [PubMed]
- 18. Liang L, Chen XL, Chen Y, Zhang NN. Surgical treatment of bipolar segmental clavicle fracture: A case report. World J Clin Cases. 2022;10(29):10529-10534. [Google Scholar] [PubMed]
- 19. Sethi K, Somasundaram K, Shorthouse M, Gidwani S. An unusual case of bipolar segmental clavicle fracture. J Orthop Surg Res. 2012;7:31. [Google Scholar] [PubMed]
- 20. Gouse M, Jacob KM, Poonnoose PM. Traumatic floating clavicle: a case report and literature review. Case Rep Orthop. 2013;2013:386089. [Google Scholar] [PubMed]
- 21. Sono T, Sagami A, Takatsuka K. Dual plating for bipolar clavicle fractures: A case report. Trauma Case Rep. 2021;34:100494. [Google Scholar] [PubMed]
- 22. Huang JI, Toogood P, Chen MR, Wilber JH, Cooperman DR. Clavicular anatomy and the applicability of precontoured plates. J Bone Joint Surg Am. 2007;89(10):2260-2265. [Google Scholar] [PubMed]
- 23. Song HS, Joh Y, Kim H. Conformity of three pre-contoured clavicular plates compared using personalized 3D-printed models of clavicles from patients. Life. 2024;14(7):888. [Google Scholar] [PubMed]
- 24. Ponce BA, Inman AJ, Satorice AM. Retrosternal anatomy with respect to the medial clavicle: An MRI study with surgical relevance. J Shoulder Elbow Surg. 2011;20(6):963-970. [Google Scholar] [PubMed]
- 25. Worman LW, Leagus C. Intrathoracic injury following retrosternal dislocation of the clavicle. J Trauma 1967;7:416-23. [Google Scholar] [PubMed]
- 26. Xing H, Cao C, Chen X, Gao Y, Huang G, Zhu J, Wang G. Bipolar clavicle fractures treatment using medial and lateral double plates: A case report. Medicine (Baltimore). 2022;101(4):e28590. [Google Scholar] [PubMed]
- 27. Robinson CM, Goudie EB, Murray IR. Open reduction and plate fixation versus nonoperative treatment for displaced midshaft clavicular fractures: a multicenter, randomized, controlled trial. J Bone Joint Surg Am. 2013;95(17):1576-1584. [Google Scholar] [PubMed]
- 28. Jain S. Bipolar fracture of clavicle-a rare injury. Bull Emerg Trauma 2017;5:136-9. [Google Scholar] [PubMed]
- 29. Panigrahi R. Bipolar clavicle fracture: A case report. J Orthop Case Rep 2015;5:33-5. [Google Scholar] [PubMed]
- 30. Park KJ, Sohn HS, Baek KY. Simultaneous fractures of the ipsilateral distal and proximal clavicle: double clavicle fracture – a case report. J Korean Fract Soc. 2011;24(1):92-95. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Bipolar Clavicle Fracture in Elderly: A Rare Case Report
February 1, 2026 Bipolar Clavicle Fracture in Elderly: A Rare Case Report December 10, 2023 Posterior Sternoclavicular Dislocation in Children: A Case Report
December 10, 2023 Posterior Sternoclavicular Dislocation in Children: A Case Report March 10, 2017 Acute Compartment Syndrome after an Olecranon Fracture in a Patient with Mild Hemophilia B
March 10, 2017 Acute Compartment Syndrome after an Olecranon Fracture in a Patient with Mild Hemophilia B June 1, 2026 Acute Post-operative Lumbar Paraspinal Compartment Syndrome Following Revision Total Joint Arthroplasty: A Case Report
June 1, 2026 Acute Post-operative Lumbar Paraspinal Compartment Syndrome Following Revision Total Joint Arthroplasty: A Case Report