
In young, non-athletic patients, a stress fracture without clear mechanical overload may represent the first manifestation of occult systemic inflammatory disease such as Crohn’s disease.
Dr. Mouas Jammal, Department of Orthopaedics and Traumatology, Hôpital Intercantonal de la Broye, Avenue de la Colline 3, 1530 Payerne, Vaud, Switzerland. E-mail: mouas.jammal@hibroye.ch
Abstract
Introduction: Stress fractures (SFs) typically result from repetitive high-impact activities in athletes or military personnel. Their occurrence in young, non-athletic individuals without significant mechanical overload is uncommon and warrants investigation for underlying systemic conditions. Although Crohn’s disease (CD) is associated with increased fracture risk due to chronic inflammation, malabsorption, and nutritional deficiencies, SFs as the initial manifestation of clinically silent CD are rarely documented. To the best of our knowledge, this represents the first reported case of a medial malleolar SF preceding the diagnosis of occult CD. This case is important because it illustrates a SF as a potential sentinel event for hidden inflammatory bowel disease (IBD), prompting orthopedic surgeons to broaden their differential diagnosis in atypical presentations.
Case Report: A 28-year-old Caucasian man presented with a 3-week history of progressive medial left ankle pain without trauma or high-impact sports participation. His only relevant activity was repetitive low-intensity bouncing while caring for his infant child. Clinical examination showed localized supramalleolar tenderness, swelling, and an antalgic gait. Magnetic resonance imaging confirmed a medial malleolar SF. In the absence of adequate mechanical overload, further evaluation revealed systemic inflammation, hypoalbuminemia, and micronutrient deficiencies, with normal standard bone metabolism parameters. Despite no gastrointestinal symptoms, additional investigations confirmed active IBD, with histology diagnostic of CD. Conservative orthopedic management, nutritional support, and targeted anti-inflammatory therapy resulted in complete resolution of musculoskeletal symptoms.
Conclusion: This case highlights that an SF can be the inaugural clinical sign of clinically silent CD. It contributes to the orthopaedic literature by reinforcing the need to consider inflammatory and metabolic causes in young, non-athletic patients with SFs lacking a clear mechanical aetiology. The implications extend beyond orthopaedics, advocating a multidisciplinary approach to unexplained skeletal fragility. Early recognition of underlying systemic disease enables prompt intervention, optimises bone health, and prevents recurrent or severe musculoskeletal issues. This report advances knowledge of CD as a systemic condition capable of compromising bone integrity independently of overt gastrointestinal symptoms.
Keywords: Stress fracture, medial malleolus, Crohn’s disease, bone fragility, extra-intestinal manifestations.
Stress fractures (SFs) are overuse injuries resulting from repetitive mechanical loading on otherwise normal bone, leading to accelerated bone remodeling and microstructural failure. They typically present with insidious pain and are most observed in athletes and military recruits. Crohn’s disease (CD) is a chronic inflammatory bowel disease (IBD) that may affect any segment of the gastrointestinal tract. Beyond its intestinal manifestations, it is increasingly recognised as a systemic disorder with significant extra-intestinal complications. Chronic inflammation, intestinal malabsorption and micronutrient deficiencies – particularly involving calcium and Vitamin D – contribute to reduced bone mineral density (BMD) and an elevated risk of fragility fractures. In addition, corticosteroid therapy further compounds skeletal fragility. While the increased overall fracture risk in patients with CD is well documented, the association between CD and SF remains less clearly defined in the literature, particularly when occurring before the diagnosis of IBD. We report the case of a 28-year-old man presenting with a medial malleolar SF in the absence of typical risk factors such as preceding trauma or high-impact sporting activity. The atypical clinical scenario prompted further investigations, ultimately leading to a new diagnosis of CD. This case is notable in that musculoskeletal symptoms preceded and led to the diagnosis of IBD, rather than the classical gastrointestinal features such as weight loss, chronic diarrhea and abdominal pain. By presenting this case, we aim to highlight a rare but clinically relevant extra-intestinal manifestation of CD and to discuss the potential pathophysiological link between IBD and SF development.
A 28-year-old man presented to the emergency department with a 3-week history of progressively worsening pain localized just proximal to the left medial malleolus. There was no history of trauma. However, he reported performing repetitive bouncing and jumping movements over the preceding 9 months while putting his son to sleep. He also described progressive medial ankle swelling, chronic lumbar pain, and left-sided De Quervain’s tenosynovitis, which had required temporary leave from his work as a hospital receptionist. Apart from increased pain on weight-bearing, he denied impaired mobility, paresthesia, sensory loss, gastrointestinal symptoms, or weight loss. He reported non-specific fatigue, which he attributed to recent fatherhood and irregular working hours. His diet was balanced and omnivorous.
His medical history included:
- Hidradenitis suppurativa (Verneuil’s disease), with one anal fistula and two para-anal abscesses
- Previous Vitamin B12 deficiency, responsive to a 6-month intranasal supplementation
- Pes planus.
He was not on regular prescription medication but self-administered dietary supplements (turmeric, ginger, omega-3 fatty acids). Family history was negative for IBD and gastrointestinal malignancy. His mother had pernicious anemia, and his father ischemic heart disease. Examination revealed physiological hindfoot valgus and moderate limitation of ankle dorsiflexion and plantarflexion. There was marked medial supramalleolar swelling with exquisite tenderness to palpation. No tenderness was noted over the lateral malleoli. The patient demonstrated an antalgic gait, sparing the left lower limb. Plain radiographs demonstrated pes planus with a Djian–Annonier angle of approximately 138°. A subtle supramalleolar radiolucent area was noted medially compared with the contralateral side (Figs. 1 and 2).
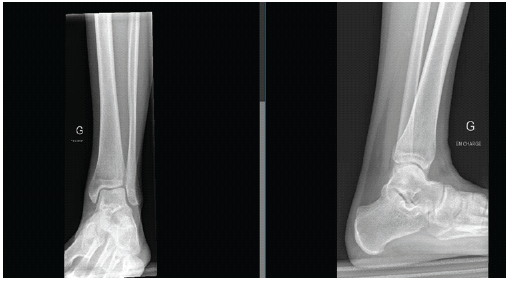
Figure 1: X-ray of the left ankle under weight-bearing: Subtle radiolucent area above the medial malleolus.

Figure 2: X-ray of the left foot under weight-bearing: Pes planus with Djian-Annonier angle of 138°.
Magnetic resonance imaging (MRI) confirmed a medial malleolus SF. Posteromedial bone marrow edema extended laterally across the former growth plate, involving approximately 40% of the tibial width. There was no intra-articular involvement or joint effusion (Fig. 3).
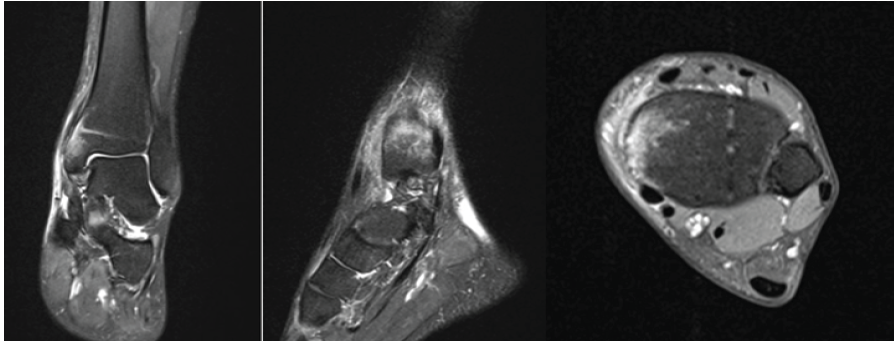
Figure 3: T2-weighted magnetic resonance imaging of the left ankle: Stress fracture of the medial malleolus.
The patient was treated conservatively with 6 weeks of immobilization in a removable boot. Strict non-weight-bearing was advised for the first 2 weeks. Thromboprophylaxis and topical diclofenac were prescribed. However, the treating orthopedic surgeon considered the degree of repetitive mechanical stress insufficient to fully explain the fracture and therefore requested a comprehensive metabolic and inflammatory work-up.
First follow-up:
At 6 weeks, the patient reported no improvement. Pain had migrated to the left knee, with tenderness over the anterior tibial tuberosity. Examination revealed dull pain at rest and on movement approximately 8 cm distal to the medial femorotibial joint line, without swelling or erythema. Laboratory investigations demonstrated:
- Elevated C-reactive protein (29.3 mg/L)
- Raised erythrocyte sedimentation rate
- Hypoalbuminemia
- Normocytic anemia (hemoglobin 130 g/L)
- Mild leukocytosis (11.2 G/L)
- Reduced Vitamin B12
- Folate and vitamin D at the lower limit of normal.
Bone metabolism markers (β-CrossLaps, P1NP, corrected calcium, phosphate, parathyroid hormone), renal and liver function tests were normal. Thyroid-stimulating hormone was normal. HLA-B27 was negative. Coeliac serology (anti-transglutaminase and anti-gliadin antibodies) was negative. Autoimmune screening revealed positive anti-Saccharomyces cerevisiae antibodies (ASCA immunoglobulin G (IgG) 64 U/mL). MRI of the left knee excluded a second SF and instead demonstrated (Fig. 4):
- Bursitis at the distal insertion of the infrapatellar ligament
- Pes anserinus insertional tendinopathy.
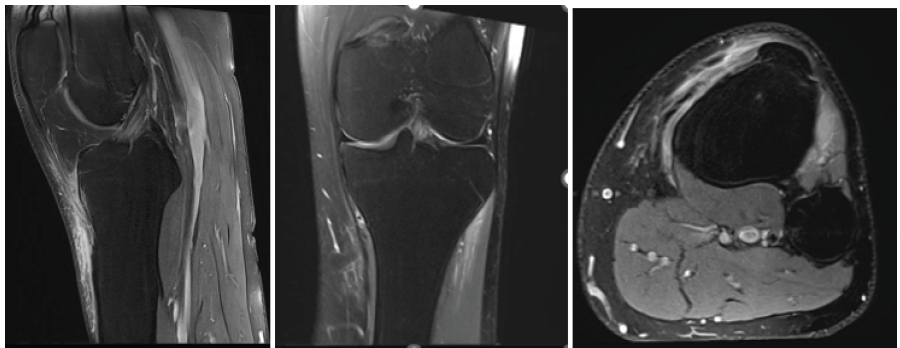
Figure 4: T2-weighted magnetic resonance imaging of the left knee: Bursitis and insertional tendinopathy of the pes anserinus.
Conservative treatment was continued, with additional supplementation of vitamin B12, vitamin D, folate, and calcium.
Second follow-up:
One month later, the patient reported marked clinical improvement. Ankle mobility was restored, with only mild tenderness at the anterior tibial tuberosity. Repeat ankle radiographs showed normal bone structure with no residual fracture line. The removable boot was replaced with a functional ankle brace for 4 weeks. However, persistent systemic inflammation and micronutrient deficiencies prompted referral to gastroenterology and rheumatology. Spinal and pelvic radiographs demonstrated right lumbar scoliosis compensating for pelvic tilt. Whole-spine MRI suggested possible early axial spondyloarthropathy; however, HLA-B27 negativity and clinical findings argued against this diagnosis.
Third follow-up:
Fecal calprotectin returned positive. Subsequent colonoscopy with biopsy revealed severe ileocolitis with ulcerated lesions in the transverse colon. Histopathology confirmed inflammatory changes consistent with CD. The diagnosis was further supported by positive ASCA IgG (64 U/mL). Notably, the patient remained entirely asymptomatic from a gastrointestinal perspective. Micronutrient deficiencies normalized following supplementation, and infliximab therapy was planned.
Final follow-up:
At final review, the patient demonstrated complete resolution of musculoskeletal symptoms. There was no tenderness over the medial malleolus or medial tibial border. Ankle range of motion was restored. He returned to full-time employment and required no further orthopedic or rheumatological follow-up.
This case highlights a significant aspect of IBD: The possibility of an SF representing the initial manifestation of clinically silent CD.
SFs:
SF are traditionally described as overuse injuries resulting from repetitive mechanical loading exceeding the bone’s adaptive capacity. They are most reported in athletes and military recruits; however, they may also develop in non-athletic individuals when physiological loading acts on bone with reduced resistance or impaired remodelling capacity [1,2]. In such cases, the distinction between excessive load and reduced bone strength becomes less clear, and SF may represent the final common pathway of heterogeneous pathogenic mechanisms. The medial malleolus represents a typical high-risk location for SF, owing to its limited vascular supply and exposure to repetitive axial and torsional forces during normal gait. Although medial malleolar SFs are classically described in running athletes, their occurrence in non-sporting individuals should prompt consideration of underlying systemic or metabolic contributors rather than purely biomechanical overload [2,3]. Delayed diagnosis is frequent, as early radiographs may appear normal, and symptoms often mimic soft tissue pathology. In the present case, the reported repetitive bouncing movements were unlikely to constitute excessive mechanical loading in a young adult. This discrepancy raised suspicion of an underlying disturbance in bone integrity.
Bone metabolism:
Bone is a metabolically active tissue undergoing continuous remodelling through the coordinated activity of osteoclasts, osteoblasts, and osteocytes. This tightly regulated process allows the skeleton to adapt to mechanical stress while repairing microdamage. However, disruption of this balance – whether due to altered hormonal signalling, chronic inflammation, or nutritional deficiencies – may transiently weaken bone and predispose it to stress injury [3,4]. Targeted remodelling plays a central role in SF pathophysiology. Microdamage accumulation induces osteocyte apoptosis and local activation of osteoclastic resorption before new bone formation occurs. During this transient phase of increased cortical porosity and reduced mechanical competence, continued loading may paradoxically increase fracture susceptibility [1]. This mechanism may be clinically relevant even in individuals not exposed to high-impact activity. Reduced bone quality, rather than low BMD alone, appears to be a critical determinant of fracture risk [4]. Emerging evidence suggests that skeletal fragility depends not only on BMD but also on microarchitectural integrity, turnover dynamics, and mineralisation quality [5]. Consequently, normal conventional bone markers do not exclude impaired bone resilience. Vitamin D plays a fundamental role in calcium-phosphate homeostasis and skeletal mineralisation. Its deficiency has been consistently associated with impaired bone strength and increased fracture risk. Inadequate vitamin D levels may lead to secondary hyperparathyroidism, increased bone turnover, and delayed mineralisation, thereby reducing the bone’s capacity to withstand repetitive mechanical stress [6,7]. While vitamin D deficiency alone is rarely sufficient to cause fracture, it may act as a permissive factor lowering the threshold for microdamage accumulation [6,8]. Identification of vitamin D deficiency following an SF should therefore not be regarded as incidental but rather as a potentially modifiable contributor to skeletal vulnerability [4,7]. The traditional distinction between fatigue fractures (normal bone exposed to abnormal load) and insufficiency fractures (abnormal bone exposed to normal load) is increasingly recognised as a continuum rather than a rigid dichotomy [2]. In non-athletic individuals, SF may occupy an intermediate position in which physiological loading acts on bone with subtly compromised material properties [4]. Recognising this overlap is clinically important, as exclusive attribution to mechanical overload may delay appropriate metabolic evaluation [1].
CD and bone manifestations:
In this context, CD represents a systemic inflammatory condition with recognised skeletal implications. CD is a chronic IBD that may affect the entire digestive tract and is increasingly understood as a systemic illness [9,10,11,12,13]. Some patients exhibit minimal or no gastrointestinal symptoms despite active inflammation, a condition referred to as ‘silent IBD’ [14,15]. Such silent forms may delay diagnosis while systemic complications continue to evolve. Bone manifestations in CD commonly include osteopenia and osteoporosis, particularly in patients exposed to corticosteroids [16]. However, chronic inflammation itself contributes to bone degradation by disrupting bone metabolism and inhibiting bone formation [16]. CD-related inflammation affects the OPG-RANK-RANKL system, promoting osteoclast activation and increasing bone resorption [9,17]. Proinflammatory cytokines (tumour necrosis factor-alpha, interleukin [IL]-1, IL-6, and interferon gamma) further enhance bone turnover and skeletal fragility, even in corticosteroid-naïve patients [18]. Evidence suggests that newly diagnosed CD patients may demonstrate reduced BMD independent of steroid therapy [19]. Malabsorption of calcium and vitamin D, along with other micronutrient deficiencies, further exacerbates skeletal compromise [12,13]. In addition to quantitative bone loss, qualitative alterations in bone microarchitecture may occur before measurable reductions in BMD become apparent.
CD and SFs:
Although SF in CD is uncommon, isolated cases have been described. Bartley reported a metatarsal SF in a patient with CD without significant trauma, attributed to nutritional deficiencies and reduced BMD [10]. Marshall described a superior pubic ramus SF in a young athlete with CD who had never received corticosteroids [19]. These reports support the concept that inflammatory and metabolic factors may predispose to stress injury independently of steroid exposure. The present case is distinctive in that the SF preceded any gastrointestinal manifestation, ultimately leading to the diagnosis of silent CD. The combination of systemic inflammation, normocytic anaemia, hypoalbuminaemia, and micronutrient deficiency likely reflected ongoing inflammatory activity contributing to impaired bone resilience. Despite normal conventional markers of bone metabolism, the patient exhibited clinical evidence of skeletal vulnerability. This case, therefore, supports the interpretation of SF as a potential sentinel event of systemic bone fragility. In young non-athletic individuals without clear mechanical overload, an SF should prompt a comprehensive metabolic and inflammatory evaluation. Recognition of underlying conditions such as CD may allow early intervention aimed at controlling inflammation, correcting nutritional deficiencies, and preventing recurrent skeletal complications.
CD should be regarded as a systemic inflammatory disorder with clinically relevant skeletal implications. Beyond its gastrointestinal manifestations, chronic inflammation and associated micronutrient deficiencies may compromise bone quality and predispose patients to SF, even in the absence of corticosteroid exposure.
This case illustrates that CD may remain clinically silent while systemic inflammatory effects are already sufficient to impair skeletal resilience. In such contexts, an SF may represent the first detectable manifestation of underlying inflammatory bone vulnerability rather than an isolated mechanical injury. Clinicians should therefore consider metabolic and inflammatory causes when evaluating SF in young, non-athletic individuals without clear overload mechanisms. Early recognition of occult systemic disease allows timely intervention, nutritional optimisation, and appropriate control of further skeletal complications.
SFs in young, non-athletic individuals without clear mechanical overload should prompt evaluation for underlying metabolic or inflammatory disease. CD may remain clinically silent while already impairing bone resilience. Early recognition of systemic causes allows timely treatment and may prevent recurrent skeletal complications.
References
- 1. Saunier J, Chapurlat R. Stress fracture in athletes. Joint Bone Spine 2018;85(3):307-10. [Google Scholar] [PubMed]
- 2. Matcuk GR Jr., Mahanty SR, Skalski MR, Patel DB, White EA, Gottsegen CJ. Stress fractures: Pathophysiology, clinical presentation, imaging features, and treatment options. Emerg Radiol 2016;23:365-75. [Google Scholar] [PubMed]
- 3. Welck MJ, Hayes T, Pastides P, Khan W, Rudge B. Stress fractures of the foot and ankle. Injury 2017;48:1722-6. [Google Scholar] [PubMed]
- 4. Moreira CA, Bilezikian JP. Stress fractures: Concepts and therapeutics. J Clin Endocrinol Metab 2017;102:525-34. [Google Scholar] [PubMed]
- 5. Merlotti D, Mingiano C, Valenti R, Cavati G, Calabrese M, Pirrotta F, et al. Bone fragility in gastrointestinal disorders. Int J Mol Sci 2022;23:2713. [Google Scholar] [PubMed]
- 6. Knechtle B, Jastrzębski Z, Hill L, Nikolaidis PT. Vitamin D and stress fractures in sport: Preventive and therapeutic measures-a narrative review. Medicina (Kaunas) 2021;57:223. [Google Scholar] [PubMed]
- 7. Wesner ML. Nutrient effects on stress reaction to bone. Can Fam Physician 2012;58:1226-30. [Google Scholar] [PubMed]
- 8. Patel DS, Roth M, Kapil N. Stress fractures: Diagnosis, treatment, and prevention. Am Fam Physician 2011;83:39-46. [Google Scholar] [PubMed]
- 9. Wei H, Zhao Y, Xiang L. Bone health in inflammatory bowel disease. Expert Rev Gastroenterol Hepatol 2023;17:921-35. [Google Scholar] [PubMed]
- 10. Bartley JJ Jr. Crohn’s disease. History and case report of associated metatarsal stress fracture. J Am Podiatr Med Assoc 1989;79:82-3. [Google Scholar] [PubMed]
- 11. Veauthier B, Hornecker JR. Crohn’s disease: Diagnosis and management. Am Fam Physician 2018;98:661-9. [Google Scholar] [PubMed]
- 12. Héla S, Nihel M, Faten L, Monia F, Jalel B, Azza F, et al. Osteoporosis and crohn’s disease. Joint Bone Spine 2005;72:403-7. [Google Scholar] [PubMed]
- 13. Bernstein CN, Leslie WD. Review article: Osteoporosis and inflammatory bowel disease. Aliment Pharmacol Ther 2004;19:941-52. [Google Scholar] [PubMed]
- 14. Coates MG, Binion DG. Silent inflammatory bowel disease. Crohns Colitis 2021;360:otab059. [Google Scholar] [PubMed]
- 15. Grinman A, Ungar B, Lahat A, Kopylov U, Eliakim R, Ben-Horin S. Incidentally diagnosed asymptomatic crohn’s disease: A retrospective cohort study of long-term clinical outcomes. Crohns Colitis 2022;360:otac034. [Google Scholar] [PubMed]
- 16. Bernstein CN. Limiting fracture risk in Crohn’s disease: Is there anything better than calcium and vitamin D? Clin Gastroenterol Hepatol 2005;3:110-2. [Google Scholar] [PubMed]
- 17. Rogler G, Singh A, Kavanaugh A, Rubin DT. Extraintestinal manifestations of inflammatory bowel disease: Current concepts, treatment, and implications for disease management. Gastroenterology 2021;161:1118-32. [Google Scholar] [PubMed]
- 18. Van Hogezand RA, Hamdy NA. Skeletal morbidity in inflammatory bowel disease. Scand J Gastroenterol Suppl 2006;243:59-64. [Google Scholar] [PubMed]
- 19. Marshall C, Gringmuth R. Pubic stress fracture presenting as a strain of adductor longus in a 16-year-old elite soccer player with Crohn’s disease: A case report. J Can Chiropr Assoc 2019;63:197-204. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Incidental Osteopoikilosis in an Ankle Fracture Patient: Case Report and Literature Review
January 1, 2026 Incidental Osteopoikilosis in an Ankle Fracture Patient: Case Report and Literature Review December 1, 2025 Adult-Onset Fanconi Syndrome Presenting as Stress Fractures: A Case Report
December 1, 2025 Adult-Onset Fanconi Syndrome Presenting as Stress Fractures: A Case Report September 1, 2025 Calcaneus and Traumatic Stress Fracture
September 1, 2025 Calcaneus and Traumatic Stress Fracture July 10, 2024 Return to Sports in Stress Reaction and Stress Fractures in Indian Athletes: A Case Series
July 10, 2024 Return to Sports in Stress Reaction and Stress Fractures in Indian Athletes: A Case Series