
Intra-articular steroid injections are associated with an increased risk of steroid arthropathy. Repeated intra-articular steroid injections over a long period should be avoided.
Dr Hiroki Kobayashi, Department of Orthopaedic Surgery, National Defence Medical College, Tokorozawa, Saitama 359-8543, Japan. E-mail: supercova0205@gmail.com
Abstract
Introduction: Steroid arthropathy is a relatively rare but serious complication of intra-articular corticosteroid injections, characterised by rapid joint destruction. Although intra-articular steroid injections are widely used for short-term pain relief in osteoarthritis, their potential risks remain under-recognised. We report a rare case of bilateral steroid arthropathy of the hip following repeated intra-articular steroid injections.
Case Report: A 60-year-old woman with bilateral hip osteoarthritis received multiple steroid injections into both hip joints over a 4-month period. Although temporary pain relief was achieved after initial injections, her symptoms progressively worsened. Imaging studies revealed the collapse of both femoral heads. Bilateral total hip arthroplasty was performed with good postoperative outcomes.
Conclusion: To the best of our knowledge, this is the first reported case of simultaneous bilateral steroid arthropathy of the hip. This case highlights the potential risk of repeated intra-articular steroid injections in weight-bearing joints and emphasises the need for cautious indication and adequate patient counselling.
Keywords: Steroid arthropathy, steroid injections, bilateral joint collapse, total hip arthroplasty, rapid joint destruction.
Intra-articular steroid injections were first reported by Hollander et al. in 1951 [1]. This treatment allows direct administration of corticosteroids into painful joints and is expected to provide potent anti-inflammatory effects. Lambert et al. reported that intra-articular injections of triamcinolone hexacetonide into the hip joints of patients with hip osteoarthritis resulted in pain relief lasting up to 3 months [2]. However, among patients who received intra-articular steroid injections of the hip, cases of rapid progression of arthropathy after injections have been reported [3], as well as cases showing sudden collapse of the femoral head resembling osteonecrosis [4]. These serious complications were first described by Sweetnam in 1960 and are referred to as steroid arthropathy [5]. Steroid arthropathy in the hip joint is a rare condition, and to the best of our knowledge, no cases of simultaneous bilateral involvement of the hip joints have been reported. Herein, we report a case of bilateral steroid arthropathy of the hip following repeated intra-articular steroid injections and discuss the possible mechanisms underlying this condition.
A 60-year-old woman presented with gait disturbance caused by severe bilateral hip pain. She had experienced discomfort in both hip joints for approximately 10 years and had been visiting a local clinic. She was diagnosed with bilateral hip osteoarthritis (Fig. 1) and received conservative treatments, including analgesic medication and rehabilitation.

Figure 1: Initial hip radiographs. Radiographs obtained at the initial visit to the previous hospital showed no remarkable degenerative changes in either hip joint.
However, since her symptoms gradually worsened, she was referred to a nearby hospital 1 year before presenting to our hospital. There, she was diagnosed with end-stage bilateral hip osteoarthritis (Fig. 2).

Figure 2: Hip radiographs before initiation of intra-articular injections. Radiographs obtained immediately before initiation of intra-articular injections demonstrated end-stage osteoarthritis in both hip joints (white arrow head).
To alleviate hip pain, she received six intra-articular steroid injections and twelve intra-articular injections of diclofenac etalhyaluronate sodium into each hip over a period of approximately 4 months. After the first intra-articular steroid injection, her pain was alleviated immediately, and her activity level increased. However, with repeated injections, the analgesic effect gradually diminished. Ultimately, she developed gait disturbance due to the worsening pain. Imaging studies performed after completion of all injections revealed a collapse of both femoral heads (Fig. 3).

Figure 3: Hip radiographs after completion of intra-articular injections. Radiographs obtained after completion of intra-articular injections showed collapse of both femoral heads (white arrow head).
She was referred to our hospital in the following year for a consultation. At the initial visit to our hospital, she complained of severe bilateral hip pain. Although she was barely able to walk using two canes, marked limping was observed. The range of motion of both hip joints was severely restricted due to pain. There were no signs of fever, skin redness, or swelling. Joint fluid culture was negative, and active infection was considered unlikely. Radiographs at presentation showed collapse of both femoral heads to approximately half of their original height. Magnetic resonance imaging could not be performed because of her claustrophobia. Based on these findings, the patient was clinically diagnosed with bilateral steroid arthropathy of the hip, and bilateral total hip arthroplasty was planned. Surgery was performed in the supine position using an anterolateral approach. Upon opening the joint capsule, serosanguinous fluid and white fragments thought to be cartilage debris were discharged from the joint. Although diffuse intra-articular hyperaemia was observed, the procedure was completed without difficulty. The acetabular components were implanted in the usual manner, and a cemented stem was used on the femoral side, considering potential bone fragility. The operative time was approximately 2 h, and blood loss was about 300 mL (Fig. 4).
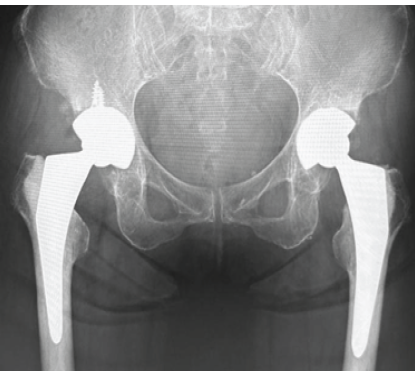
Figure 4: Postoperative radiographs. Total hip arthroplasty was successfully performed without major complications.
Bilateral hip pain resolved the day after surgery, and rehabilitation was initiated with walker-assisted ambulation. Her postoperative recovery was favourable, and she was discharged home 1 week after surgery with stable ambulation using a T-cane. She returned to factory work 1 month postoperatively and resumed jogging 3 months after surgery. After more than a year of follow-up, she has experienced no recurrence of hip pain and has resumed normal daily activities.
The reported incidence of steroid arthropathy ranges from 0.6% to 21% [6,7,8], with substantial variation among studies. This wide variation is likely attributable to the lack of established diagnostic criteria and severity classifications for steroid arthropathy. It is presumed that reported cases include a highly heterogeneous population, ranging from mild joint deformity to severe femoral head collapse. Nevertheless, it is generally accepted that steroid arthropathy is a relatively rare condition. Most reported cases of steroid arthropathy involve the knee or shoulder, and cases limited to the hip are uncommon. The reason for the difference in incidence between joints is unclear, but it is likely because intra-articular injections are performed less frequently in the hip than in the knee or shoulder in everyday clinical practice. In addition, since cases of high-steroid arthropathy are often broadly diagnosed as “rapidly destructive hip disease”, it is also possible that the actual number of cases has been underestimated. These issues make it difficult to ascertain the incidence and clinical characteristics of steroid arthropathy in the hip. Intra-articular steroid injections have been shown to provide superior pain relief compared with intra-articular hyaluronic acid injections, and several guidelines recommend their use [9]. In particular, their efficacy in short-term pain relief over approximately 8–12 weeks has been reported [2,10]. However, evidence supporting sustained analgesic effects with long-term administration is limited, and no studies have demonstrated clear long-term benefits. While some reports suggest no association between disease progression and steroid dosage or injection frequency, other studies indicate that repeated or high-dose intra-articular steroid injections may increase the risk of femoral head collapse [11]. Taken together, these findings suggest that repeated long-term intra-articular steroid injections offer little benefit while potentially increasing the risk of severe joint destruction. In the present case, triamcinolone acetonide was administered 6 times over 4 months, representing a clinical situation with limited benefit and an increased risk of joint destruction. Ultimately, the collapse of both femoral heads occurred, supporting the idea that repeated intra-articular steroid injections should be avoided. The pathophysiology of steroid arthropathy warrants further consideration. Previous studies have reported that intra-articular steroid injections were not associated with adverse effects on articular cartilage in patients with juvenile idiopathic arthritis [12] and that steroid injection alone under non-weight-bearing conditions did not induce cartilage degeneration [13]. These studies suggest that steroid arthropathy is unlikely to result solely from the pharmacological effects of corticosteroids on joint cartilage. In contrast, there are reports of rapid joint collapse following intra-articular steroid injections in joints with pre-existing advanced cartilage degeneration [2,3]. Furthermore, Murray et al. have suggested that cartilage degeneration accelerates when intra-articular steroid injections are combined with mechanical loading or exercise [13]. These observations indicate that steroid arthropathy is primarily caused by increased mechanical stress resulting from temporary pain relief following corticosteroid injections. In accordance, it is becoming increasingly accepted that pain serves as a protective signal to prevent excessive mechanical stress on the joints. This concept is further illustrated by studies investigating the aetiology of Charcot arthropathy and patients who developed joint destruction following treatment with anti-nerve growth factor monoclonal antibodies [14,15]. In the present case, immediate pain relief and increased activity were observed following initial steroid injections. However, the pain relief was temporary, and the symptoms progressively worsened afterward, ultimately leading to gait disturbance. This clinical course is consistent with the proposed mechanism whereby joint pain relief is associated with accelerated joint damage. Although intra-articular steroid injections are effective at alleviating pain, physicians treating patients with osteoarthritis should be aware that the effect is only temporary and that repeated treatments can increase the risk of joint destruction.
We reported a case of bilateral steroid arthropathy of the hip following repeated intra-articular steroid injections. Although intra-articular steroid injections can provide effective short-term pain relief in patients with osteoarthritis, their repeated or prolonged use can increase the risk of joint destruction. Since there is no established method of preventing rapid joint destruction in steroid arthropathy, physicians treating patients with osteoarthritis should avoid repeated intra-articular steroid injections.
Intra-articular steroid injections are associated with an increased risk of steroid arthropathy. Repeated intra-articular steroid injections over a long period should be avoided.
References
- 1. Hollander JL, Brown EM Jr., Jessar RA, Brown CY. Hydrocortisone and cortisone injected into arthritic joints; comparative effects of and use of hydrocortisone as a local antiarthritic agent. J Am Med Assoc 1951;147:1629-35. [Google Scholar] [PubMed]
- 2. Lambert RG, Hutchings EJ, Grace MG, Jhangri GS, Conner-Spady B, Maksymowych WP. Steroid injection for osteoarthritis of the hip: A randomized, double-blind, placebo-controlled trial. Arthritis Rheum 2007;56:2278-87. [Google Scholar] [PubMed]
- 3. Tiwari A, Karkhur Y, Keeney JA, Aggarwal A. Rapid destructive osteoarthritis of the hip after intra-articular steroid injection. Arthroplast Today 2018;4:184-6. [Google Scholar] [PubMed]
- 4. Ahmed AF, Hammad M, Salameh M, Ahmed GO. Destructive osteonecrosis of the femoral head after a single intra-articular corticosteroid injection: A report of two cases. Int J Surg Case Rep 2020;77:711-5. [Google Scholar] [PubMed]
- 5. Sweetnam DR, Mason RM, Murray RO. Steroid arthropathy of the hip. Br Med J 1960;1:1392-4. [Google Scholar] [PubMed]
- 6. Sanguino RA, Sood V, Santiago KA, Cheng J, Casey E, Mintz D, et al. Prevalence of rapidly progressive osteoarthritis of the hip following intra-articular steroid injections. PM R 2023;15:259-64. [Google Scholar] [PubMed]
- 7. Hess SR, O’Connell RS, Bednarz CP, Waligora AC 4th, Golladay GJ, Jiranek WA. Association of rapidly destructive osteoarthritis of the hip with intra-articular steroid injections. Arthroplast Today 2018;4:205-9. [Google Scholar] [PubMed]
- 8. Kolasinski SL, Neogi T, Hochberg MC, Oatis C, Guyatt G, Block J, et al. 2019 American college of rheumatology/arthritis foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis Rheumatol 2020;72:220-33. [Google Scholar] [PubMed]
- 9. McCabe PS, Maricar N, Parkes MJ, Felson DT, O’Neill TW. The efficacy of intra-articular steroids in hip osteoarthritis: A systematic review. Osteoarthritis Cartilage 2016;24:1509-17. [Google Scholar] [PubMed]
- 10. Okike K, King RK, Merchant JC, Toney EA, Lee GY, Yoon HC. Rapidly destructive hip disease following intra-articular corticosteroid injection of the hip. J Bone Joint Surg Am 2021;103:2070-9. [Google Scholar] [PubMed]
- 11. Sahin N, Ozdemir Cicek S, Pac Kisaarslan A, Dursun I, Poyrazoglu MH, Dusunsel R. The effect of intra-articular steroid injection on the cartilage and tendon thicknesses in juvenile idiopathic arthritis. Mod Rheumatol 2024;34:791-7. [Google Scholar] [PubMed]
- 12. Gogia PP, Brown M, Al-Obaidi S. Hydrocortisone and exercise effects on articular cartilage in rats. Arch Phys Med Rehabil 1993;74:463-7. [Google Scholar] [PubMed]
- 13. Murray RC, DeBowes RM, Gaughan EM, Zhu CF, Athanasiou KA. The effects of intra-articular methylprednisolone and exercise on the mechanical properties of articular cartilage in the horse. Osteoarthritis Cartilage 1998;6:106-14. [Google Scholar] [PubMed]
- 14. Hochberg MC. Serious joint-related adverse events in randomized controlled trials of anti-nerve growth factor monoclonal antibodies. Osteoarthritis Cartilage 2015;23 Suppl 1:S18-21. [Google Scholar] [PubMed]
- 15. Chan RL, Chan CH, Chan HF, Pan NY. The many facets of neuropathic arthropathy. BJR Open 2019;1:20180039. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report
August 1, 2026 Total Hip Arthroplasty without Subtrochanteric Shortening Osteotomy in a Neglected Posterior Hip Dislocation: A Case Report August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections
August 1, 2026 Case Report of Rapidly Destructive Osteoarthritis of the Hip following Multiple High-dose Intra-articular Steroid Injections August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips
August 1, 2026 Total Hip Arthroplasty in Bilateral Ankylosed Hip by Direct Anterior Approach: A Case Report with Technical Tips August 1, 2026 Metallosis Following Total Hip Arthroplasty: A Case Report
August 1, 2026 Metallosis Following Total Hip Arthroplasty: A Case Report