
A staged, well-planned reconstructive approach combining prosthetic replacement, stable fracture fixation, and nerve reconstruction can achieve good functional outcomes even in rare, complex ipsilateral humeral triad injuries.
Dr. S Anandkumar, ARS Hospital, Tiruppur, Tamil Nadu, India. E-mail: sadasanand66@gmail.com
Abstract
Introduction: Ipsilateral humeral shaft and proximal humerus fractures are rare and typically an outcome of high-energy trauma. The coexistence of humeral head avascular necrosis (AVN) and high radial nerve palsy in a delayed presentation makes management particularly challenging and is rarely reported in the literature. This case is important as it highlights a unique combination of bony and neural pathology requiring a carefully staged reconstructive approach.
Case Report: A 39-year-old Indian man arrived 4 months after a road traffic accident with left shoulder and arm discomfort, deformity, and inability to extend wrists and fingers. He had initially undergone traditional splinting by a local bone setter. Clinical examination revealed wrist as well as finger drop suggestive of high radial nerve palsy. Imaging demonstrated a comminuted fracture nonunion of the proximal humerus with AVN of the humeral head and a fracture of the mid-shaft of the humerus. The patient was managed with a staged surgical approach that included radial nerve exploration as well as grafting, fixation of the humeral shaft fracture, and subsequent shoulder hemiarthroplasty.
Conclusion: This case demonstrates that delayed presentation of complex ipsilateral humeral injuries can be successfully managed with a staged approach addressing both skeletal and neural components. The combination of prosthetic replacement, stable fracture fixation, and nerve reconstruction can lead to satisfactory functional outcomes. This report adds to the limited literature on such rare injury patterns. It provides a practical framework for managing similar complex cases, thereby contributing to improved decision-making in orthopaedic trauma care.
Keywords: Proximal humerus fracture, humeral shaft fracture, radial nerve palsy, avascular necrosis, hemiarthroplasty, nerve grafting.
Fractures of the proximal humerus account for approximately 3–5% of all fractures [1]. Although fractures of the proximal humerus and mid-shaft humerus are individually common, their simultaneous occurrence is rare and commonly results from high-energy trauma [2]. The coexistence of radial nerve palsy and avascular necrosis (AVN) further complicates management. Radial nerve injury is commonly related to humeral mid-shaft fractures, and high radial nerve palsy carries a poorer prognosis due to proximal involvement [3]. Osteonecrosis of the humeral head represents a serious consequence of disrupted vascularity, particularly in delayed presentations. Management decisions depend on fracture pattern, chronicity, and bone viability [4]. Reports describing the simultaneous presence of humeral head AVN, shaft fracture, and high radial nerve palsy in delayed presentation are exceedingly scarce, and optimal management strategies remain unclear. This report describes a rare case of ipsilateral proximal humerus fracture with shaft fracture complicated by AVN of the humeral head and high radial nerve palsy, managed successfully with a staged surgical approach.
A 39-year-old male presented with pain and swelling over the proximal and mid-third of the left arm, restricted shoulder movements, and inability to extend the wrist and fingers for 4 months following a road traffic accident. He had initially undergone traditional splinting by a local bone setter. On examination, there was deformity of left midthird arm, crepitus, and restricted left shoulder motion. A wrist and finger drop suggestive of high radial nerve palsy was noted. Radiographs showed a comminuted proximal humerus fracture (AO 11-C.2) with nonunion, where the head was rotated 180°, and a mid-shaft humerus fracture (AO 12-A.3). Magnetic resonance imaging confirmed AVN of the humeral head with collapse (Figs. 1, 2, 3).
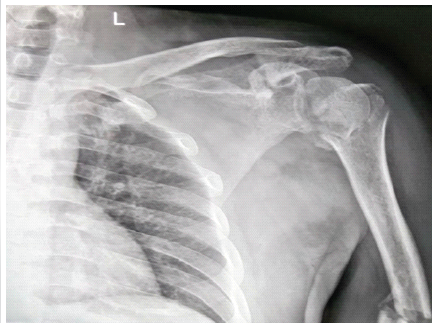
Figure 1: Radiograph showing proximal humerus fracture (AO 11-C.2).

Figure 2: Radiograph showing mid-shaft humerus fracture (AO 12-A.3).
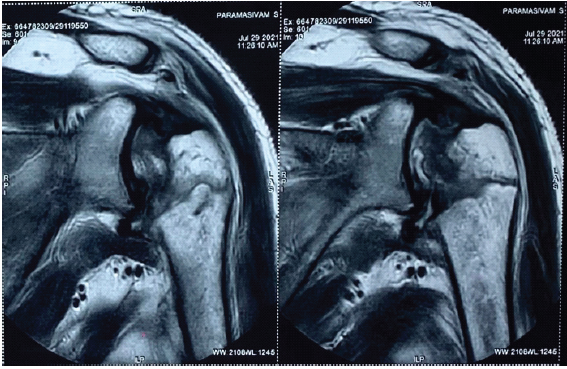
Figure 3: Magnetic resonance imaging avascular necrosis of humeral head.
Management:
A staged surgical approach was undertaken. Despite the complexity of the injury and delayed presentation, a staged surgical approach was planned.
- Stage 1: Radial nerve exploration and shaft fixation
The patient was placed in the right lateral decubitus position under general anaesthesia, with the forearm supported and the elbow flexed. A posterior approach to the humerus was utilised. Intraoperatively, the radial nerve has been found entrapped within the fracture site, surrounded by dense callus and fibrous tissue. Careful neurolysis was performed, revealing a segmental defect of approximately 8 cm, necessitating reconstruction. The humeral shaft fracture was exposed, fibrous tissue was cleared, and fracture ends were freshened. Anatomical reduction was achieved and stabilised using a locking compression plate, supplemented with cerclage control cables. Subsequently, sural nerve grafting was performed to bridge the defect using microsurgical techniques, ensuring a tension-free repair (Figs. 4 and 5).
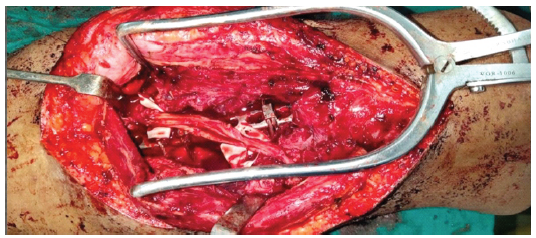
Figure 4: Intraoperative image showing humerus shaft fixation and nerve grafting.
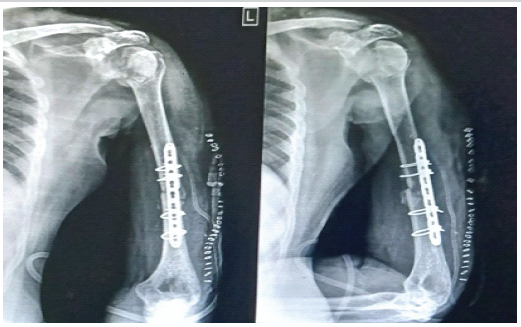
Figure 5: Postoperative radiograph after stage 1.
- Stage 2: Proximal humerus replacement
In the second stage, the patient was positioned in the beach chair position. A transdeltoid lateral method was employed to access the proximal humerus. The humeral head was nonviable with features consistent with advanced AVN. The head was excised, and a long-stem hemiarthroplasty prosthesis was implanted, extending across the fracture site into the distal fragment to provide stable fixation and restore alignment (Fig. 6).
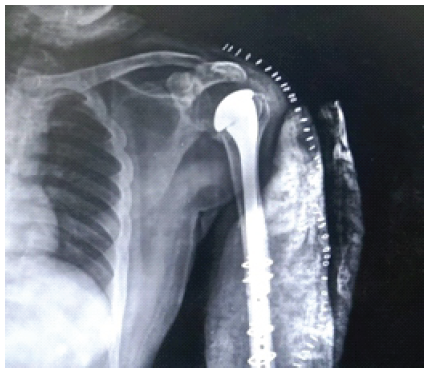
Figure 6: Postoperative radiograph after hemiarthroplasty.
Subsequently, the limb was immobilised in an above-elbow plaster slab for 3 weeks. The patient received routine antibiotics, and regular sterile dressings were performed. Sutures were removed at 2 weeks, and there were no postoperative complications. Follow-up radiographs were obtained at 3 weeks and subsequently at monthly intervals. The slab was removed at 3 weeks, following which a structured rehabilitation programme was initiated, including gradual shoulder, elbow, and wrist mobilisation, progressive strengthening exercises, and radial nerve stimulation therapy.
Outcome and follow-up:
At 3 weeks after surgery, the wound had healed well. The immobilisation was discontinued, and the patient was started on a guided rehabilitation programme. By 6 weeks, the patient reported noticeable pain relief. Early signs of fracture healing were seen on radiographs. Shoulder movements were still limited, with abduction and flexion up to 40°, but elbow motion had almost returned to normal. At 3 months, there was clear progression toward fracture union. Elbow movements had fully recovered, while shoulder mobility remained limited but stable, with abduction and flexion up to 40°. Early clinical signs of radial nerve recovery were also observed. At the 6-month follow-up, the patient showed further improvement. Shoulder abduction had increased to 90° and flexion to 110°. There was also partial return of wrist extension, suggesting ongoing nerve recovery. At 1 year, radiographs confirmed a solid union of the mid-shaft humerus fracture and a well-positioned, stable prosthesis without any signs of loosening or subsidence. Neurologically, the radial nerve had partially recovered, with wrist and finger extension graded at 2/5 power, indicating continued regeneration after nerve grafting. Functionally, the patient was able to carry out daily activities independently, with only minimal limitations (Fig. 7, 8, 9).

Figure 7: Follow-up radiograph showing union.

Figure 8: Shoulder abduction at 1 year.
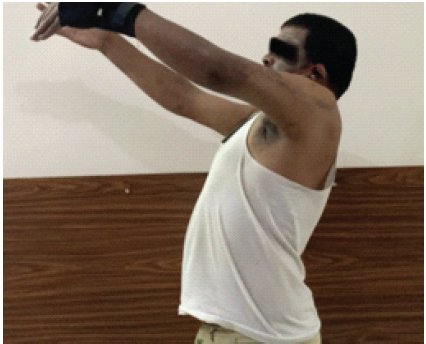
Figure 9: Shoulder flexion at 1 year.
Managing ipsilateral proximal humerus and mid-shaft humerus fractures becomes particularly challenging when patients present late. In most acute cases, proximal humerus fractures were treated with internal fixation, especially in younger individuals, where preserving the native joint is desirable. Locking plate fixation has shown good outcomes when bone quality is adequate and vascularity is intact [1,2]. In our case, however, the situation was quite different. The patient presented 4 months after injury, by which time the comminuted humeral head had already undergone avascular changes. Attempting fixation in such a scenario would likely have resulted in failure or a poor functional outcome. In these circumstances, hemiarthroplasty provides a more predictable option, particularly when the viability of the humeral head is compromised. Boileau et al. have reported more consistent results with arthroplasty in such cases [5]. The presence of a coexisting mid-shaft fracture added another layer of complexity. We were essentially dealing with two problems at the same time: reconstruction of a nonviable proximal humerus as well as stabilisation of the shaft. The use of a long-stem prosthesis helped bridge the fracture, but it also limited the ability to place screws for plate fixation. To address this, we supplemented locking plate fixation with cerclage cables. This hybrid technique provided additional stability in areas where screw purchase was not possible due to the prosthetic stem. Similar strategies have been described in complex humeral and periprosthetic fractures [6]. Another important aspect of this case was the management of high radial nerve palsy with a large segmental defect. While many radial nerve injuries recover spontaneously, cases with nerve discontinuity require surgical intervention. Sural nerve grafting remains a reliable option for bridging large defects. Studies have shown that long segment nerve grafts may still recover function, although outcomes are influenced by timing and defect length [7,8,9,10]. Overall, this case demonstrates the importance of adapting surgical strategies based on fracture biology, chronicity, and mechanical constraints.
Delayed presentation can significantly alter the management of complex humeral injuries. In this case, AVN and comminution made hemiarthroplasty the more reliable option for the proximal humerus. At the same time, stable fixation of the mid-shaft fracture and reconstruction of the radial nerve were essential for functional recovery. The combination of a long-stem prosthesis with cable-assisted fixation and nerve grafting provided a practical solution. A staged approach, careful surgical planning, and structured rehabilitation can lead to satisfactory outcomes even in complex neglected injuries.
This case highlights the importance of recognising and managing complex, neglected ipsilateral humeral injuries involving both skeletal and neural components. A staged reconstructive strategy combining hemiarthroplasty, stable fracture fixation, and nerve grafting can provide satisfactory functional outcomes even in delayed presentations. It underscores the need for individualised surgical planning in rare and challenging orthopaedic scenarios.
References
- 1. Robinson CM, Court-Brown CM, McQueen MM, Wakefield AE. Estimating the risk of nonunion following nonoperative treatment of a clavicular fracture. J Bone Joint Surg Am 2003;85:1215-23. [Google Scholar] [PubMed]
- 2. Gardner MJ, Boraiah S, Helfet DL, Lorich DG. Indirect medial reduction and strut support of proximal humerus fractures using an endosteal implant. J Orthop Trauma 2008;22:195-200. [Google Scholar] [PubMed]
- 3. Shao YC, Harwood P, Grotz MR, Limb D, Giannoudis PV. Radial nerve palsy associated with fractures of the shaft of the humerus: A systematic review. J Bone Joint Surg Br 2005;87:1647-52. [Google Scholar] [PubMed]
- 4. Hasan SS, Romeo AA. Nontraumatic osteonecrosis of the humeral head. J Am Acad Orthop Surg 2002;10:28-36. [Google Scholar] [PubMed]
- 5. Boileau P, Krishnan SG, Tinsi L, Walch G, Coste JS, Molé D. Tuberosity malposition and migration: Reasons for poor outcomes after hemiarthroplasty for proximal humerus fractures. J Shoulder Elbow Surg 2002;11:401-12. [Google Scholar] [PubMed]
- 6. Wright TW, Cofield RH. Humeral fractures after shoulder arthroplasty. J Bone Joint Surg Am 1995;77:1340-6. [Google Scholar] [PubMed]
- 7. Sunderland S. Nerve injuries and their repair: A critical appraisal. J Bone Joint Surg Br 1991;73:1-7. [Google Scholar] [PubMed]
- 8. Kim DH, Kline DG. Management and results of peroneal nerve lesions. J Hand Surg Am 2001;26:655-62. [Google Scholar] [PubMed]
- 9. Birch R, Bonney G. Surgical Disorders of the Peripheral Nerves. London: Churchill Livingstone; 1998. [Google Scholar] [PubMed]
- 10. Mackinnon SE, Dellon AL. Surgery of the Peripheral Nerve. New York: Thieme; 1988. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 November 1, 2025 A Study on Functional Outcome of Hemiarthroplasty for Proximal Humeral Fractures – An Observational Study
November 1, 2025 A Study on Functional Outcome of Hemiarthroplasty for Proximal Humeral Fractures – An Observational Study July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach
July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach
July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach June 1, 2026 Cemented versus Uncemented Hemiarthroplasty in Femoral Neck Fractures: A Comparative Case Series Using Singh Index for Surgical Decision-Making
June 1, 2026 Cemented versus Uncemented Hemiarthroplasty in Femoral Neck Fractures: A Comparative Case Series Using Singh Index for Surgical Decision-Making