
Kienbock’s Disease remains an often-missed diagnosis requiring early clinical vigilance. Persistent wrist pain in a young adult should raise suspicion beyond a simple sprain. Timely stage-based intervention can preserve wrist mechanics and prevent collapse. Early diagnosis transforms outcome in this silent but progressive disorder.
Dr. Prashanth Kempulraj, Department of Orthopaedics, Govt. Kilpauk Medical College Hospital, Poonamalle High Road, Kilpauk, Chennai-10 . E-mail: prashanthkempulraj@gmail.com
Abstract
Introduction: Kienböck's disease is a rare and progressive condition characterised by avascular necrosis of the lunate, leading to chronic wrist pain, functional impairment, and eventual carpal collapse. Early diagnosis is often challenging due to non-specific clinical presentation and low sensitivity of initial radiographs.
Case Report: A 29-year-old female presented with progressive left wrist pain and restricted movements for 6 months, without any history of trauma or classical risk factors. Clinical examination revealed localised tenderness and significant limitation of wrist mobility. Radiological evaluation with plain radiographs, computed tomography, and magnetic resonance imaging (MRI) confirmed avascular necrosis of the lunate, consistent with Lichtman stage IIIB disease. The patient underwent proximal row carpectomy (PRC) as a motion-preserving salvage procedure. Serial follow-up demonstrated progressive improvement in clinical and functional parameters. The disabilities of the arm, shoulder, and hand score improved from 62 preoperatively to 28 at 3 months, 15 at 6 months, and 8 at 1 year, while the Mayo Wrist Score improved from 45 (poor) to 65 (fair), 75 (good), and 85 (good) over the same period. At the 1-year follow-up, the patient was pain-free at rest, with a satisfactory range of motion and return to daily activities.
Conclusion: Kienbock’s disease should be considered in patients with persistent wrist pain, even in the absence of classical risk factors. Early MRI plays a crucial role in diagnosis and staging. PRC provides reliable pain relief and favourable functional outcomes in advanced stages, as demonstrated by sustained improvement over 1 year.
Keywords: Kienbock’s disease, avascular necrosis, lunate, proximal row carpectomy, wrist pain, and Lichtman classification.
Kienböck’s disease, first described by Robert Kienböck in 1910, represents a progressive osteonecrosis of the lunate, culminating in structural collapse, carpal instability, and degenerative arthritis of the wrist [1,2]. Although uncommon, it remains a clinically significant cause of chronic wrist pain and functional disability, particularly in young, active individuals. The reported prevalence ranges from 0.0066% to 0.27%, with a classical predilection for males in the second to fourth decades of life. The pathogenesis of Kienbock’s disease is complex and multifactorial, involving an interplay of vascular, mechanical, and anatomical factors [2]. Lunate is uniquely predisposed to avascular necrosis due to its variable and often tenuous blood supply. Vascular inflow is derived from dorsal and volar arterial systems, but in a substantial subset of individuals, a single-vessel pattern exists (Gelberman type I), which lacks sufficient intraosseous collateralisation. This limited redundancy renders the lunate highly susceptible to ischaemia following even minor vascular compromise [3]. From a biomechanical standpoint, negative ulnar variance has been strongly associated with increased axial loading of the lunate, resulting in repetitive microtrauma and progressive vascular insufficiency [2]. In addition, alterations in carpal kinematics, including increased radio-scaphoid loading and abnormal force transmission, further contribute to disease progression. These mechanical factors not only initiate but also perpetuate the pathological cascade. Kienböck’s disease should not be viewed solely as a vascular disorder but rather as a failure of the lunate under abnormal biomechanical stress in the setting of compromised perfusion. Early stages are characterised by reversible ischaemia and bone marrow oedema, whereas advanced stages demonstrate trabecular collapse, fragmentation, and carpal instability, particularly dorsal intercalated segment instability (DISI). These structural changes ultimately lead to altered wrist biomechanics and secondary degenerative arthritis. Clinically, the disease presents insidiously with dorsal wrist pain, decreased grip strength, and progressive limitation of motion. Early diagnosis is challenging, as plain radiographs may appear normal in the initial stages. Magnetic resonance imaging (MRI) has emerged as the most sensitive modality, capable of detecting early ischaemic changes before structural collapse occurs. Computed tomography (CT) provides additional detail regarding fragmentation and carpal alignment. The Lichtman classification remains the most widely used staging system, guiding management strategies based on structural progression [4,5]. Treatment options range from conservative measures in early stages to joint-levelling procedures, revascularisation techniques, and salvage procedures such as proximal row carpectomy (PRC) or wrist arthrodesis in advanced disease. Despite numerous surgical options, there remains ongoing debate regarding optimal management, particularly in intermediate stages. This case highlights an atypical presentation of Kienbock’s disease in a young female without classical risk factors and underscores the importance of early MRI-based diagnosis and stage-specific surgical intervention.
A 29-year-old female presented with complaints of left wrist pain for 6 months. The pain was gradual in onset, progressive, aggravated by activity, and relieved with rest. She reported difficulty performing daily activities, including household work and typing. There was no history of trauma, inflammatory arthritis, steroid use, or smoking. The patient had a history of hypothyroidism on regular medication. On clinical examination, there was no swelling or warmth. Localised dorsal wrist tenderness was present with marked restriction of movements (Table 1).
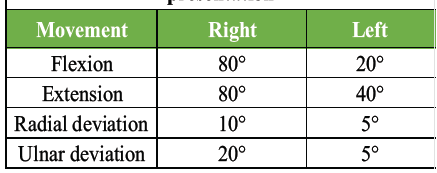
Table 1: Range of motion at the time of presentation
Investigations:
Plain radiographs of the left wrist (anteroposterior and lateral views) demonstrated increased radiodensity of the lunate, suggestive of sclerosis, without obvious fragmentation in early imaging (Fig. 1).

Figure 1: Pre-operative radiograph showing sclerosis of Lunate.
There was no gross evidence of carpal malalignment. CT of the wrist provided better delineation of bony architecture and revealed fragmentation and collapse of the lunate with loss of its normal contour. Subtle alterations in carpal alignment were also appreciated, indicating progression of disease. An MRI was performed for definitive assessment and staging. The lunate appeared hypointense on T1-weighted images with corresponding signal changes on T2-weighted sequences, consistent with avascular necrosis. There was associated bone marrow oedema and evidence of structural compromise without advanced radiocarpal arthritis (Fig. 2).

Figure 2: Hypointense Lunate on T1-weighted image.
Based on the combined radiological findings, the diagnosis of Kienbock’s disease (Lichtman stage IIIB) was established. Considering the advanced stage of disease (Lichtman stage IIIB), persistent symptoms, and functional limitation, a decision was made to proceed with PRC as a motion-preserving salvage procedure.
Surgical technique:
Under regional anaesthesia and tourniquet control, a standard dorsal approach to the wrist was utilised. After careful soft-tissue dissection, the extensor retinaculum was incised, and the wrist joint was exposed through a dorsal capsulotomy. The proximal carpal row was sequentially excised, including the scaphoid, lunate, and triquetrum. Intraoperatively, the lunate was found to be collapsed with areas of fragmentation and loss of structural integrity, confirming advanced avascular necrosis. The articular surface of the capitate and the lunate fossa of the distal radius were inspected and found to be adequately preserved, making the patient a suitable candidate for PRC. The remaining carpal bones were allowed to articulate with the distal radius, thereby maintaining a functional radio capitate joint. Haemostasis was achieved, and the wound was closed in layers (Fig. 3).
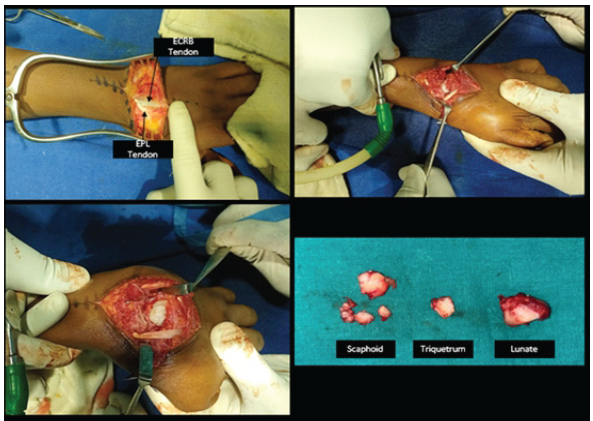
Figure 3: Intraoperative pictures.
A below-elbow splint was applied with the wrist maintained in slight extension. Postoperatively, the wrist was immobilised for 4 weeks. Early active finger mobilisation was encouraged from post-operative day 1. Gradual wrist mobilisation initiated at 6 weeks. The immediate post-operative radiograph showed complete removal of the proximal carpal bone and good radio-capitate articulation (Fig. 4).

Figure 4: Immediate post-operative radiograph.
The rehabilitation protocol included supervised wrist mobilisation exercises followed by progressive strengthening exercises under physiotherapy guidance.
Follow-up:
The patient was followed up at regular intervals of 1 month, 3 months, 6 months, and 1 year postoperatively to assess pain relief, range of motion, functional recovery, and radiological outcomes. Wrist range of motion was assessed clinically using goniometric measurements and compared with the contralateral wrist during serial follow-up visits. At 1 month, the patient reported mild pain during wrist movements, with no pain at rest. The surgical wound had healed well without complications. Wrist immobilisation was discontinued, and supervised physiotherapy focusing on gradual mobilisation was initiated. At 3 months, there was a marked reduction in pain and improvement in functional capacity. The patient was able to perform most routine daily activities with minimal discomfort. Radiographs demonstrated maintained alignment of the radiocapitate articulation without evidence of instability. At 6 months, the patient showed further functional improvement and reported only occasional discomfort during strenuous activities. Clinically assessed grip strength improved progressively to approximately 65–70% of the contralateral side when compared with the unaffected wrist. At 1 year, the patient was pain-free at rest and experienced only minimal discomfort with heavy loading (Fig. 5).

Figure 5: Patient having near normal range of motion and good functional outcome at the end of 1 year
The patient was also able to resume household activities, typing, and routine functional tasks without significant limitation. Radiographs demonstrated preserved radiocapitate joint congruity, with no evidence of progressive degenerative changes or carpal instability (Fig. 6 and Table 2).

Figure 6: X-ray at 1-year follow-up with preserved radiocapitate joint congruity, with no evidence of degenerative changes.
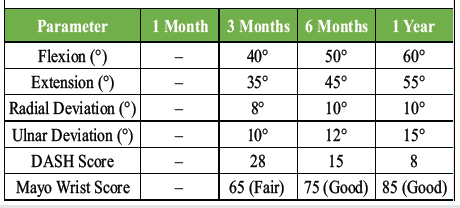
Table 2 – Post operative follow-up and outcome measures
Kienböck’s disease represents a complex interplay between vascular insufficiency and biomechanical overload, with ongoing debate regarding its primary aetiology [2]. Contemporary understanding suggests that both factors act synergistically, with vascular compromise rendering the lunate vulnerable and mechanical stress precipitating structural failure. The vascular hypothesis centres on the limited and variable intraosseous blood supply of the lunate. The presence of a single-vessel supply pattern in a significant proportion of individuals reduces the capacity for collateral perfusion, predisposing the bone to ischaemia. However, vascular insufficiency alone does not fully explain disease progression, as not all individuals with compromised vascular patterns develop osteonecrosis [3]. Biomechanical factors play a critical role in disease initiation and progression. Negative ulnar variance leads to increased compressive forces across the radiolunate joint, subjecting the lunate to repetitive microtrauma. Over time, this results in trabecular microfractures, vascular compromise, and eventual collapse [2]. Importantly, recent biomechanical studies suggest that abnormal load transmission may precede overt vascular failure, indicating that Kienböck’s disease may, in part, represent a mechanical failure syndrome of the lunate. Collapse of the lunate disrupts the normal carpal architecture, leading to scaphoid flexion and DISI. This altered alignment increases radioscaphoid contact pressures, accelerating degenerative changes and further compromising wrist function. The present case is notable for the absence of classical risk factors such as negative ulnar variance, repetitive trauma, or systemic disease, highlighting the heterogeneity of disease presentation. Increasing recognition of such atypical cases suggests that additional, yet unidentified, factors may contribute to disease pathogenesis. Imaging plays a pivotal role in diagnosis and staging. While plain radiographs are useful in advanced stages, MRI remains the gold standard for early detection, with high sensitivity for bone marrow oedema and ischaemia. CT imaging complements MRI by providing a detailed assessment of bony architecture, fragmentation, and carpal alignment, which are critical for surgical planning. Management of Kienböck’s disease is stage-dependent. Early stages may be managed conservatively or with joint-levelling procedures aimed at reducing load across the lunate. In advanced stages, salvage procedures are indicated. PRC is a well-established surgical option for Stage IIIB disease, particularly in the presence of preserved capitate cartilage [6,7]. Alternative surgical options for Lichtman stage IIIB disease include vascularised bone grafting, radial shortening osteotomy, limited intercarpal fusion, and wrist arthrodesis. The choice of procedure depends on disease stage, cartilage preservation, patient age, and functional demand. In the present case, PRC was preferred because of advanced lunate collapse with preserved radiocapitate articulation and the need for a motion-preserving salvage procedure. In the present case, PRC resulted in significant functional improvement, as evidenced by a reduction in disabilities of the arm, shoulder, and hand (DASH) score from 62 preoperatively to 8 at 1 year, and improvement in Mayo Wrist Score from 45 (poor) to 85 (good). These findings are consistent with published literature, which reports pain relief in approximately 80–90% of patients and preservation of 60–70% of wrist motion following PRC [6, 8–10]. The stepwise improvement observed at 3, 6, and 12 months further supports the predictable recovery trajectory associated with this procedure, with most functional gains occurring within the first 6 months and continued improvement up to 1 year. The absence of radiocapitate degenerative changes at 1-year follow-up in this case is encouraging, although long-term surveillance is necessary, as radiographic arthritis may develop over time. However, it is well established that such changes do not always correlate with clinical symptoms. Long-term studies have similarly demonstrated sustained pain relief and functional preservation following PRC despite radiographic degenerative progression in some patients [8–10]. The patient continues under periodic clinical and radiological follow-up, which is needed to monitor for late degenerative changes and long-term functional outcomes.
Limitations:
This report has certain limitations inherent to a single-patient case report design, thereby limiting the generalisability of the findings to the broader population. Functional outcomes were assessed using validated scoring systems, including DASH and Mayo Wrist Score, along with serial clinical assessment of grip strength and goniometric evaluation of wrist range of motion during follow-up. However, standardised dynamometric measurements and formal biomechanical or kinematic analyses were not performed. Advanced vascular imaging modalities such as contrast-enhanced MRI or angiographic assessment of lunate vascularity were not utilised in this case. As with all case reports, selection bias remains unavoidable. Nevertheless, this case remains clinically relevant because of its atypical presentation in a young female without classical predisposing factors and the favourable short-term functional recovery following proximal row carpectomy.
Kienbock’s disease is an uncommon yet clinically significant cause of chronic wrist pain that may present even in the absence of classical risk factors. This case highlights the importance of maintaining a high index of suspicion and utilising early MRI for accurate diagnosis and staging. Stage-based surgical intervention remains the cornerstone of management in advanced disease. PRC serves as an effective motion-preserving salvage procedure, providing reliable pain relief and meaningful functional recovery, as demonstrated by progressive improvement in objective outcome scores over a 1-year follow-up. Early recognition and appropriate surgical decision-making are critical in optimising outcomes and preventing long-term disability in patients with Kienböck’s disease.
In advanced stages of Kienbock’s Disease with lunate collapse and secondary degenerative changes, Proximal Row Carpectomy remains a reliable motion-preserving salvage procedure. Timely surgical decision-making provides effective pain relief, improves functional range of motion, and restores useful hand function.
References
- 1. Kienböck R. Über traumatische malazie des mondbeins. Fortschr Geb Röntgenstr 1910;16:77-103. [Google Scholar] [PubMed]
- 2. Schuind F, Eslami S, Ledoux P. Kienbock’s disease. J Bone Joint Surg Br 2008;90:133-9. [Google Scholar] [PubMed]
- 3. Gelberman RH, Bauman TD, Menon J, Akeson WH. The vascularity of the lunate bone and Kienböck’s disease. J Hand Surg Am 1980;5:272-8. [Google Scholar] [PubMed]
- 4. Lichtman DM, Mack GR, MacDonald RI, Gunther SF, Wilson JN. Kienböck’s disease: The role of silicone replacement arthroplasty. J Bone Joint Surg Am 1977;59:899-908. [Google Scholar] [PubMed]
- 5. Allan CH, Joshi A, Lichtman DM. Kienbock’s disease: Diagnosis and treatment. J Am Acad Orthop Surg 2001;9:128-36. [Google Scholar] [PubMed]
- 6. Stahl S, Stahl AS, Meisner C, Rahmanian-Schwarz A, Schaller HE, Lotter O. Correction: A systematic review of the etiopathogenesis of Kienböck’s disease and a critical appraisal of its recognition as an occupational disease related to hand-arm vibration. BMC Musculoskelet Disord 2024;25:215. Erratum in: BMC Musculoskelet Disord 2012;13:225. [Google Scholar] [PubMed]
- 7. Chim H, Moran SL. Long-term outcomes of proximal row carpectomy: A systematic review of the literature. J Wrist Surg 2012;1:141-8. [Google Scholar] [PubMed]
- 8. Ali MH, Rizzo M, Shin AY, Moran SL. Long-term outcomes of proximal row carpectomy: a minimum of 15-year follow-up. Hand (N Y). 2012 Mar;7(1):72-8. doi: 10.1007/s11552-011-9368-y. Epub 2011 Nov 4. PMID: 23449142; PMCID: PMC3280369. [Google Scholar] [PubMed] [CrossRef]
- 9. Croog AS, Stern PJ. Proximal row carpectomy for advanced Kienböck’s disease: average 10-year follow-up. J Hand Surg Am. 2008 Sep;33(7):1122-30. doi: 10.1016/j.jhsa.2008.02.031. PMID: 18762108. [Google Scholar] [PubMed] [CrossRef]
- 10. Jebson PJ, Hayes EP, Engber WD. Proximal row carpectomy: a minimum 10-year follow-up study. J Hand Surg Am. 2003 Jul;28(4):561-9. doi: 10.1016/s0363-5023(03)00248-x. PMID: 12877841. [Google Scholar] [PubMed] [CrossRef]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach
July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach
July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study
June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study June 1, 2026 A Rare Neglected Ipsilateral Humeral Triad: Comminuted Proximal Humerus Nonunion with Avascular Necrosis, Mid-Shaft Fracture, and High Radial Nerve Palsy Managed with Staged Reconstruction
June 1, 2026 A Rare Neglected Ipsilateral Humeral Triad: Comminuted Proximal Humerus Nonunion with Avascular Necrosis, Mid-Shaft Fracture, and High Radial Nerve Palsy Managed with Staged Reconstruction