
Clinicians should perform adequate techniques to prevent spacer dislocation, and if this occurs, a revision spacer is an option rather than Girdlestone arthroplasty.
Dr. Ibaad Khan, Department of Orthopaedic Surgery, Rothman Orthopaedic Institute at Thomas Jefferson University, Philadelphia, Pennsylvania, USA. E-mail: ibaadkhan0@gmail.com
Abstract
Introduction: Dislocation of an articulating antibiotic spacer is a rare but significant complication following the first stage of revision hip arthroplasty for infection. This report describes a case of posterior dislocation of a right hip articulating with an antibiotic spacer, its management, and subsequent total hip arthroplasty (THA).
Case Report: A 67-year-old man presented with chronic right hip pain and limited mobility. Radiographs and laboratory work confirmed septic arthritis of the native hip, with aspiration cultures positive for methicillin-sensitive Staphylococcus aureus. He initially underwent right hip resection arthroplasty with articulating antibiotic spacer placement, which dislocated shortly thereafter. Closed reduction was unsuccessful. He subsequently underwent revision of the dislocated spacer with a new articulating spacer. Intraoperative cultures were positive for Bacillus species, and intravenous antibiotics were administered. Definitive THA was later performed as a second-stage procedure. At the latest follow-up, he was ambulating independently with minimal pain and no recurrent infection.
Conclusion: Spacer dislocation is a rare yet serious complication that can compromise infection control and mechanical stability. Adequate techniques should be employed to ensure this does not happen, and if it does, a surgeon should consider a revision antibiotic spacer instead of Girdlestone arthroplasty.
Keywords: Periprosthetic joint infection, total hip arthroplasty, two-stage revision, antibiotic spacer.
Periprosthetic joint infection (PJI) remains one of the most devastating complications following total hip arthroplasty (THA) [1]. The gold standard for chronic PJI treatment is two-stage exchange arthroplasty, which involves component explantation and placement of an antibiotic spacer followed by delayed reimplantation [2]. Antibiotic-eluting spacers maintain limb length and soft-tissue tension while delivering high local concentrations of antibiotics [3]. Despite their therapeutic benefit, spacer-related complications, including fracture, mechanical failure, and dislocation, can compromise functional outcomes and prevent infection eradication [4]. Spacer dislocation has previously been identified as the most common overall mechanical complication of these procedures [5]. Reported dislocation rates vary widely, ranging from 6% to 41% depending on spacer design, patient factors, and fixation technique [6,7,8]. Spacer dislocation has been associated with various surgical and patient-specific factors, including insufficient fixation of the spacer, typically due to undersizing; reduced femoral offset; acetabular bone loss; and patient noncompliance with postoperative instructions [9,10]. Spacer design may play a role, with some evidence for higher rates of mechanical complications, including instability in moulded spacers compared to preformed spacers [5]. Interestingly, Bori et al. found no modifiable risk factors for spacer dislocation despite worse clinical outcomes in those patients [11]. Closed reduction may be attempted but with varying success rates; Faschingbauer et al. found that only four of 12 observed spacer dislocations could undergo closed reduction and stable retention [12]. Many cases have therefore traditionally been managed with Girdlestone resection arthroplasty, which sacrifices joint function and soft-tissue tension in order to prevent further mechanical complications or provide further infection control. However, recent evidence suggests that spacer revision can be an effective option with infection eradication and acceptable complication rates while preserving joint function [13]. We present a case of dislocation of an articulating antibiotic hip spacer managed successfully with revision to a semi-constrained design, followed by definitive reimplantation. This case highlights critical surgical decision-making and technical considerations in managing early spacer instability.
A 67-year-old man (body mass index 27.5 kg/m2, the American Society of Anaesthesiologists Physical Status Classification System III, and Charlson Comorbidity Index 3) with a history of chronic obstructive pulmonary disease, left upper-extremity deep vein thrombosis, and degenerative joint disease presented with several months of worsening right native hip pain and limited ambulation. He underwent platelet-rich plasma injection in the hip and subsequently had a significant increase in pain in the days following the injection, concerning for septic arthritis. Hip aspiration indicated native hip septic arthritis with cultures positive for methicillin-sensitive Staphylococcus aureus, and intravenous (IV) nafcillin therapy was initiated.
Initial surgery and complication:
Over the course of the next 2 months, the patient underwent multiple irrigations and debridements, with recurrent pain and persistent infection. He then underwent right hip resection arthroplasty with insertion of an articulating antibiotic spacer. Immediately after surgery, he experienced acute right hip pain in the post-anaesthesia care unit. Radiographs demonstrated posterior dislocation of the spacer without fracture (Fig. 1). Closed reduction was attempted but was unsuccessful. He was then transferred from the outside hospital (OSH) and outside surgeon to our tertiary care centre, approximately 1 month after this initial dislocation event, as he was being managed nonoperatively at the OSH.
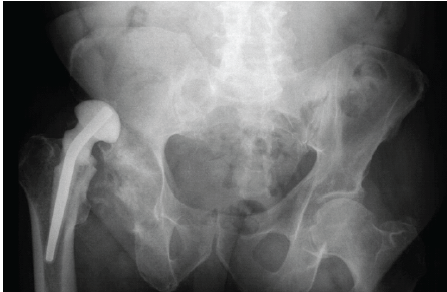
Figure 1: Dislocated antibiotic spacer. AP radiograph of the pelvis demonstrating posterior dislocation of the spacer relative to the acetabulum with no associated fracture evident.
Revision spacer surgery:
The patient returned to the operating room for removal of the dislocated spacer and insertion of a new articulating spacer utilising real components. Our decision was made to proceed with an articulating spacer rather than a Girdlestone due to numerous flaws in the original procedure’s surgical technique, including varus malpositioning, inadequate version, and leg-length discrepancy. Intraoperatively, the femoral stem was well-fixed, and no purulence was noted, but there was significant superolateral acetabular bone loss with formation of a pseudoacetabulum. The stem was approached first and removed with no issue. We then approached the acetabulum. Since the hip was dislocated for nearly 1 month, a pseudoacetabulum was beginning to develop. To find the real acetabulum, the cotyloid fossa was identified, and a cobra retractor was placed inferior to the transverse acetabular ligament. We utilised reamers and an intraoperative X-ray to confirm that the anatomic acetabulum was indeed identified (Fig. 2).
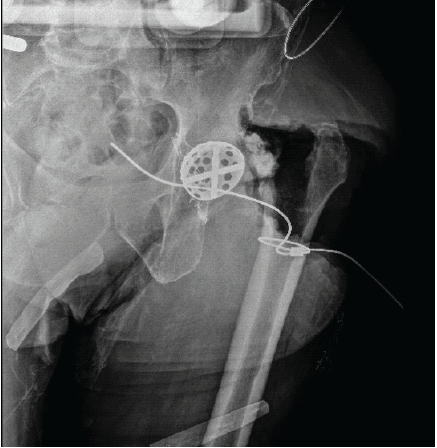
Figure 2: Intraoperative X-ray confirming identification of anatomic acetabulum. Intra-operative AP radiograph utilizing a reamer shell to confirm correct identification of the anatomic acetabulum.
After debridement and identification of the true acetabulum, two 35-mm screws were placed to be used as an augment to our cement fixation. Bone wax was placed in the screw holes for easy removal during the planned second stage. A constrained liner was used to reduce the risk of repeat dislocation. The liner was cemented in place in appropriate anteversion and abduction with 2 bags of cement and methylene blue. The new spacer was fashioned using a size 3 × 150 mm stem moulded with high-viscosity cement containing 3 g of vancomycin and 2.4 g of tobramycin per bag. The real stem was impacted into position and trialled to ensure our ability to relocate the hip. The stem was then loosely cemented proximally and allowed to cure to maintain appropriate anteversion. We then trialled the hip again and identified the correct head size, which provided adequate stability. This head was placed, and the hip was finally reduced. Intraoperative imaging confirmed stable alignment without fracture (Fig. 3). Cultures grew Bacillus species. Postoperatively, the patient was managed with IV nafcillin (2 g every 4 h) and vancomycin (1.5 g every 12 h). The patient was made toe-touch weight-bearing with posterior hip precautions and received apixaban for venous thromboembolism prophylaxis.
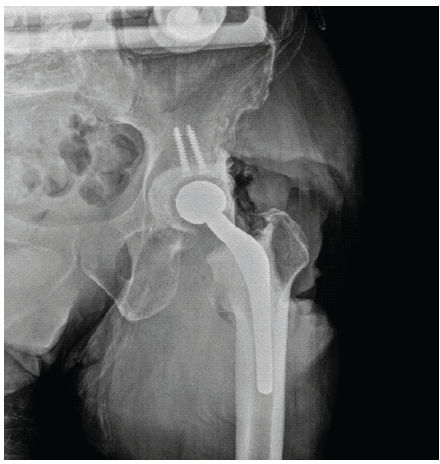
Figure 3: Intraoperative imaging of final spacer construct. Intraoperative AP radiograph of final spacer construct demonstrating stable alignment without fracture.
Definitive reimplantation:
After completion of 6 weeks of IV antibiotics, labs demonstrated a downtrending erythrocyte sedimentation rate and C-reactive protein within normal limits. The patient underwent re-aspiration, which was negative for infection. A total of 4 months after the revision spacer procedure, the patient underwent the second-stage procedure with definitive THA. After removal of the spacer components, a revision multi-hole acetabular component was implanted with multiple screws. A cerclage cable was placed to prevent fracture, then a monoblock diaphyseal-engaging stem was placed, followed by antibiotic-infused beads. Post-operative radiographs demonstrated an anatomically aligned THA with no periprosthetic fracture (Fig. 4). At final follow-up, the patient was ambulating independently with minimal discomfort and no evidence of recurrent infection.
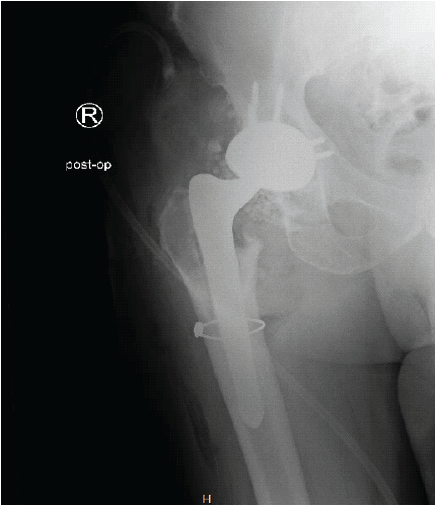
Figure 4: Post-operative radiograph after second-stage definitive THA. Post-operative AP radiograph demonstrating definitive implant including revision multi-hole acetabular component, cerclage cable, and a monoblock diaphyseal engaging stem.
Dislocation of an articulating antibiotic spacer is an uncommon but clinically significant complication during staged management of hip PJI. Articulating spacers are intended to preserve joint motion and have demonstrated higher treatment success rates as compared to static spacers [14]. Static spacers have also been associated with a significantly longer length of hospital stay [15]. Several factors can predispose towards spacer instability. Acetabular bone defects, abductor insufficiency, and history of previous instability events have all been implicated [5]. Spacer design itself is also important, as adequate femoral fixation and appropriate head/neck ratio can reduce the risk of complications [9]. Previous data have demonstrated that articulating spacers using real-component articulations (versus all-cement articulations) provide several advantages, including improved limb length restoration and higher rates of home discharge [16]. Using real-component articulating spacers allows surgeons to better optimize offset and leg length, which may minimize the risk of instability. In our case, significant acetabular deficiency likely played a role in early dislocation of the index spacer construct. Closed reduction has been described but is frequently unsuccessful [12]. Historically, recurrent dislocation has sometimes led surgeons to perform Girdlestone resection arthroplasty to prevent repeat dislocation. However, this approach sacrifices limb length and function. When bone stock allows, revising the dislocated spacer can restore stability while maintaining limb mechanics [13]. In the present case, use of acetabular screw augmentation with a constrained liner and real-component articulation provided sufficient mechanical stability for a successful articulating spacer and eventual reimplantation. Most reports of spacer dislocation involve the knee rather than the hip; thus, data on hip spacer instability remain limited. Mechanical complications across both hip and knee spacers are common, yet these complications do not always negatively impact the likelihood of successful reimplantation [17]. Practical strategies to minimize dislocation risk include appropriate spacer sizing, careful cementation, reinforcement of acetabular bone loss, and the selective use of constrained liners in high-risk settings. Hybrid screw-cement fixation, as described by Patel et al. and Pizzo et al., has shown promise in improving construct stability in similar situations [18,19]. Proper techniques to provide stability cannot be ignored: surgeons must avoid placing the spacer in varus, restore appropriate leg lengths, and place both the femoral and acetabular components with appropriate anteversion. Adequate reaming of the acetabulum and use of an acetabular component within the spacer construct are also key considerations in order to achieve stability. In infection cases with early or persistent instability, surgeons must consider persistent infection, which may occur with inadequate initial debridement, lack of acetabular reaming, insufficient use of irrigation, and incorrectly tailored antibiotics. Ultimately, infection control remains the foundation of successful two-stage exchange. The combination of nafcillin and vancomycin used in this case provided broad Gram-positive coverage, consistent with current recommendations for culture-directed therapy in PJI [3]. The absence of recurrent infection at follow-up highlights the value of combining stable mechanical reconstruction with effective antimicrobial management. This case demonstrates that prompt recognition and revision of a dislocated spacer can preserve joint mechanics and enable successful second-stage reimplantation. Surgeons should maintain a high index of suspicion for early post-operative pain or instability, particularly in patients with poor bone stock or chronic infection, as timely intervention can lead to excellent functional outcomes and infection control.
Dislocation following hip-articulating antibiotic spacer placement, though rare, is a serious complication that can jeopardise infection control and mechanical stability. Early recognition, surgical revision, and culture-directed antibiotics can restore joint integrity and allow for successful second-stage reimplantation. Attention to spacer design and acetabular support is critical to preventing recurrence.
Hip articulating spacer dislocation is uncommon but should be suspected in patients with chronic infection or acetabular bone loss who develop acute pain or clinical signs of instability. Early diagnosis, timely revision, and appropriate antibiotic therapy can prevent morbidity and facilitate successful two-stage reconstruction.
References
- 1. Blanco JF, Díaz A, Melchor FR, Da Casa C, Pescador D. Risk factors for periprosthetic joint infection after total knee arthroplasty. Arch Orthop Trauma Surg 2020;140:239-45. [Google Scholar] [PubMed]
- 2. Lazic I, Scheele C, Pohlig F, Von Eisenhart-Rothe R, Suren C. Treatment options in PJI – is two-stage still gold standard? J Orthop 2021;23:180-4. [Google Scholar] [PubMed]
- 3. Naoum S, Koutserimpas C, Pantekidis I, Giovanoulis V, Veizi E, Piagkou M, et al. Antimicrobial regimens in cement spacers for periprosthetic joint infections: A critical review. Antibiotics (Basel) 2024;13:772. [Google Scholar] [PubMed]
- 4. Jung J, Schmid NV, Kelm J, Schmitt E, Anagnostakos K. Complications after spacer implantation in the treatment of hip joint infections. Int J Med Sci 2009;6:265-73. [Google Scholar] [PubMed]
- 5. Sambri A, Fiore M, Rondinella C, Morante L, Paolucci A, Giannini C, et al. Mechanical complications of hip spacers: A systematic review of the literature. Arch Orthop Trauma Surg 2023;143:2341-53. [Google Scholar] [PubMed]
- 6. Jacobs C, Christensen CP, Berend ME. Static and mobile antibiotic-impregnated cement spacers for the management of prosthetic joint infection. J Am Acad Orthop Surg 2009;17:356-68. [Google Scholar] [PubMed]
- 7. Romanò CL, Romanò D, Logoluso N, Meani E. Long-stem versus short-stem preformed antibiotic-loaded cement spacers for two-stage revision of infected total hip arthroplasty. Hip Int 2010;20:26-33. [Google Scholar] [PubMed]
- 8. Leunig M, Chosa E, Speck M, Ganz R. A cement spacer for two-stage revision of infected implants of the hip joint. Int Orthop 1998;22:209-14. [Google Scholar] [PubMed]
- 9. Jones CW, Selemon N, Nocon A, Bostrom M, Westrich G, Sculco PK. The influence of spacer design on the rate of complications in two-stage revision hip arthroplasty. J Arthroplasty 2019;34:1201-6. [Google Scholar] [PubMed]
- 10. Anagnostakos K, Fürst O, Kelm J. Antibiotic-impregnated PMMA hip spacers: Current status. Acta Orthop 2006;77:628-37. [Google Scholar] [PubMed]
- 11. Bori G, García-Oltra E, Soriano A, Rios J, Gallart X, Garcia S. Dislocation of preformed antibiotic-loaded cement spacers (Spacer-G): Etiological factors and clinical prognosis. J Arthroplasty 2014;29:883-8. [Google Scholar] [PubMed]
- 12. Faschingbauer M, Reichel H, Bieger R, Kappe T. Mechanical complications with one hundred and thirty eight (antibiotic-laden) cement spacers in the treatment of periprosthetic infection after total hip arthroplasty. Int Orthop (SICOT) 2015;39:989-94. [Google Scholar] [PubMed]
- 13. Clemente A, Cavagnaro L, Russo A, Chiarlone F, Massè A, Burastero G. Spacer exchange in persistent periprosthetic joint infection: Microbiological evaluation and survivorship analysis. Arch Orthop Trauma Surg 2023;143:1361-70. [Google Scholar] [PubMed]
- 14. Warwick HS, Tan TL, Weiser L, Shau DN, Barry JJ, Hansen EN. Comparison of static and articulating spacers after periprosthetic joint infection. J Am Acad Orthop Surg Glob Res Rev 2023;7:e22.00284. [Google Scholar] [PubMed]
- 15. Nahhas CR, Chalmers PN, Parvizi J, Sporer SM, Deirmengian GK, Chen AF, et al. Randomized trial of static and articulating spacers for treatment of the infected total hip arthroplasty. J Arthroplasty 2021;36:2171-7. [Google Scholar] [PubMed]
- 16. Kugelman D, Roof M, Egol A, Guanche I, Chen AF, Schwarzkopf R, et al. Comparing articulating spacers for periprosthetic joint infection after primary total hip arthroplasty: All-cement versus real-component articulating spacers. J Arthroplasty 2022;37:S657-63. [Google Scholar] [PubMed]
- 17. Costanzo J, McCahon J, Tokarski AT, Deirmengian C, Bridges T, Fliegel BE, et al. Mechanical complications of hip and knee spacers are common. Cureus 2023;15:e38496. [Google Scholar] [PubMed]
- 18. Patel JN, Pizzo RA, Yoon RS, Liporace FA. Addressing antibiotic hip spacer instability via hybrid screw-cement fixation of a constrained liner and cement-rebar interface techniques: A technical narrative. J Am Acad Orthop Surg 2020;28:166-70. [Google Scholar] [PubMed]
- 19. Pizzo RA, Patel JN, Viola A, Keller DM, Yoon RS, Liporace FA. Reducing dislocations of antibiotic hip spacers via hybrid cement-screw constrained liner fixation: A case series. Hip Pelvis 2020;32:207-13. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2025 A Rare Case of Staphylococcus Caprae Periprosthetic Hip Infection with Unusual Clinical Presentation
January 1, 2025 A Rare Case of Staphylococcus Caprae Periprosthetic Hip Infection with Unusual Clinical Presentation July 1, 2026 Bone Morphogenetic Proteins-2–Augmented Acetabular Bone Stock Restoration During Two-stage Revision for Periprosthetic Joint Infection: A Case Report
July 1, 2026 Bone Morphogenetic Proteins-2–Augmented Acetabular Bone Stock Restoration During Two-stage Revision for Periprosthetic Joint Infection: A Case Report June 1, 2026 Sequential Multi-organism Periprosthetic Joint Infection after Total Hip Arthroplasty: A Case Report
June 1, 2026 Sequential Multi-organism Periprosthetic Joint Infection after Total Hip Arthroplasty: A Case Report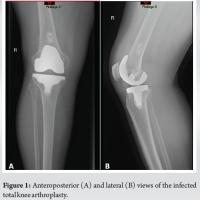 September 1, 2024 Case Reports: Periprosthetic Joint Infection after Total Joint Arthroplasty Following Swimming Activity
September 1, 2024 Case Reports: Periprosthetic Joint Infection after Total Joint Arthroplasty Following Swimming Activity