
Solitary osteochondroma can cause progressive bilateral genu valgum necessitating staged surgical intervention; sustained bilateral limb surveillance is essential after unilateral deformity correction.
Dr. Aditya Kekatpure, Department of Orthopaedics, Datta Meghe Medical College, Off-Campus Centre of Datta Meghe Institute of Higher Education and Research, Hingna Road, Wanadongri, Nagpur - 441110, Maharashtra, India. E-mail: adityalkekatpure@gmail.com
Abstract
Introduction: Osteochondromas are among the most frequently encountered benign bone tumours, yet their association with progressive angular deformity in the coronal plane is uncommon. This case is, to our knowledge, not well characterised in the existing literature and highlights the possibility of contralateral deformity progression following unilateral surgical correction of a solitary osteochondroma.
Case Report: We describe the clinical course of a young adult female who presented with a left distal femoral osteochondroma in 2022, managed surgically with concurrent correction of an associated genu valgum deformity. Over the ensuing months, the patient developed progressively worsening valgus deformity on the contralateral right knee, ultimately requiring a separate corrective osteotomy in 2023. This sequential, bilateral progression in a patient with a solitary lesion is exceptionally rare.
Conclusion: Both interventions yielded satisfactory outcomes, with restoration of limb alignment and meaningful functional recovery. This report draws attention to the possibility of contralateral deformity progression in such patients and underscores the value of sustained bilateral post-operative surveillance. The case contributes to the limited literature on deformity progression associated with solitary osteochondroma and has direct clinical impact for orthopaedic surgeons managing similar presentations.
Keywords: Osteochondroma, genu valgum, distal femoral osteotomy, angular deformity, benign bone tumor.
Osteochondroma is the most common benign bone tumour, accounting for roughly 35% (between 20% and 50%) of all benign osseous neoplasms and approximately 9% of all bony neoplasms overall [1,2]. These lesions characteristically arise from the metaphyseal cortex of long bones, with a particular predilection for the region around the knee. In the vast majority of cases, they follow a reassuringly benign course: They are incidentally discovered, asymptomatic, and require nothing more than periodic observation. Angular deformity of the lower limb is a different matter entirely. When limb deformity does complicate an osteochondroma, it may do so by causing increased growth at the involved site of the growth plate [3]. In this case, we found this to result in a rapidly progressing coronal plane deformity. What we encountered in this case was something quite different: A young patient with a solitary distal femoral osteochondroma who developed significant ipsilateral genu valgum underwent successful surgical correction, and post-surgical correction revealed a contralateral valgus deformity. The sequential nature of this presentation, the absence of hereditary exostoses, and the need for staged bilateral intervention across two separate admissions make this case worth reporting. It raises questions about the mechanisms driving such bilateral deformity progression, and it offers a practical reminder that in these patients, the story does not necessarily end with the first surgery.
Patient background:
Our patient was a young adult female who initially came to attention with pain and a visible deformity of the left knee, along with increasing difficulty walking, difficulty in squatting, and impairment of daily life activities. There were no other joints involved, no family history suggestive of hereditary multiple exostoses, and no features consistent with a systemic skeletal dysplasia. This appeared to be a straightforward case of a solitary lesion in an otherwise healthy individual. Clinical assessment with the Knee Society Score (KSS) was performed, revealing a KSS of 66, indicating the patient required prompt management.
First presentation and surgical management:
Radiographic evaluation confirmed a distal femoral osteochondroma on the left side (see Fig. 1), with an associated coronal plane deformity that was mechanically significant.

Figure 1: Pre-operative X-ray
The lateral distal femoral angle (LDFA) measured 79°, reflecting a clear deviation from normal anatomical alignment. Given the degree of deformity and the patient’s symptoms, a decision was made to address both pathologies in a single operative setting. Surgery proceeded with excision of the osteochondroma followed by a distal femoral osteotomy to correct the valgus deformity. The procedure was technically uncomplicated, and the post-operative course was smooth. Alignment improved meaningfully, with the LDFA correcting to 86° (see Table 1).
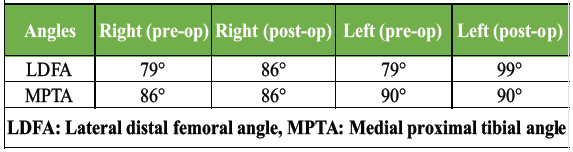
Table 1 : Pre-operative and post-operative LDFA and MPTA measurements
The patient was mobilised with full weight-bearing relatively early, and recovery was satisfactory.
Second presentation and surgical management:
When the patient returned for routine follow-up, the clinical picture was clear. There was marked valgus deformity at the right knee, a compensatory alteration in gait, pain on weight-bearing, and measurable mechanical axis deviation on standing radiographs (see Fig. 2).
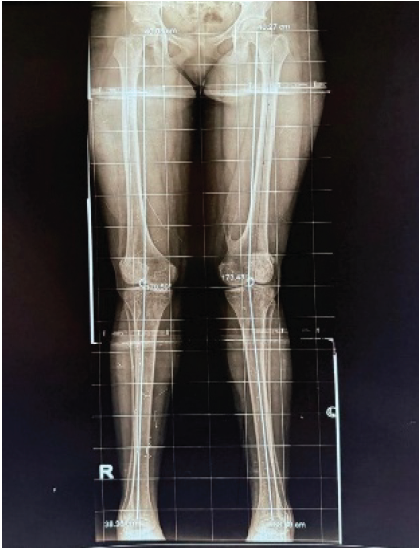
Figure 2: Post-operative X-ray (4 years post operative)
The decision to proceed with surgical correction was straightforward, given the degree of deformity and the patient’s functional limitations. A closing wedge distal femoral varus osteotomy was performed, with fixation achieved using a distal femoral locking plate. Correction was confirmed intraoperatively. The post-operative course mirrored that of the first surgery: the patient tolerated the procedure well, was mobilised with progressive weight-bearing, and recovered without incident.
Follow-up and outcomes:
At follow-up review, the patient had achieved bilateral restoration of limb alignment. Pain had resolved significantly on both sides, gait had normalised, and there were no complications to report: No wound issues, no implant failure, no evidence of tumour recurrence on the left, and no new lesions on the right (see Fig. 3).

Figure 3: Post-operative X-ray (1 year after 2nd Operative management – Right side)
Functional improvement was assessed using the KSS, which improved to 92, an excellent indicator of functional recovery. The overall trajectory was one of progressive improvement on both sides following their respective interventions. The patient remained under surveillance, with the understanding that continued monitoring was warranted given the unusual bilateral nature of the deformity.
This case is unusual on several levels, and it is worth unpacking each of those elements separately before considering what they might mean together. The first point of interest is simply the coexistence of a solitary distal femoral osteochondroma with a clinically significant genu valgum. This association, while not impossible, is not what one typically expects from a solitary lesion. Most osteochondromas in this location are mechanically inert from a deformity standpoint. The literature on angular deformity complicating solitary osteochondromas is sparse; the bulk of the deformity literature in this context pertains to multiple hereditary exostoses, where physeal disruption by multiple lesions is a well-recognised mechanism of growth disturbance [1,3,4,5,6,7,8,9]. In our patient, no such multiplicity was present. The second, and more puzzling, element is the subsequent genu valgum on the contralateral side. By the time the right-sided deformity became apparent, the left had already been surgically corrected with a satisfactory result. There was no tumour on the right side, no metabolic abnormality to explain a bilateral process, and no family history to suggest a hereditary condition [7,8,10,11]. One could speculate that a subtle underlying predisposition to physeal or periarticular growth imbalance exists in this patient, potentially made manifest by altered biomechanics following the first surgery, though we acknowledge this remains speculative. Gait adaptation following unilateral limb realignment can alter loading patterns across the contralateral knee, and while such changes are not typically sufficient to produce osteotomy-level deformity, they cannot be entirely discounted. What this case illustrates practically is the importance of not treating the contralateral limb as a passive bystander after a unilateral deformity correction. In most orthopaedic practices, post-operative surveillance is appropriately focused on the operated side. This case suggests that in patients with unusual presentations, active monitoring of contralateral limb alignment should be part of the follow-up protocol, at least for a defined period. From a surgical standpoint, both interventions were executed with standard techniques. Distal femoral osteotomy for genu valgum is a well-established procedure with a reliable track record, and the use of a locking plate for fixation provides stable, predictable outcomes [4,5]. What made this case instructive was less about the technical aspects of each surgery and more about the clinical decision-making framework required to recognize the second problem and act on it appropriately. Cases like the one presented here are rare enough that they are unlikely to appear in large series, which is precisely why individual case reports retain value. They serve as prompts to ask questions that population-level data cannot address.
The case described here represents an unusual clinical trajectory: A young patient with a solitary distal femoral osteochondroma who required staged bilateral surgical intervention for progressive genu valgum. Both procedures achieved good outcomes, and the patient recovered satisfactory alignment and function. The exact mechanism driving the contralateral deformity remains uncertain, and the association between a solitary osteochondroma and progressive bilateral valgus is, to our knowledge, not well documented in the literature [6,9]. For the practising orthopaedic surgeon, the key takeaway is straightforward: in patients presenting with unusual deformity patterns, follow-up should extend beyond the operated limb. Long-term, bilateral surveillance of alignment is a low-cost, high-yield strategy that can allow early identification of contralateral progression before it becomes severe. Timely intervention, when indicated, leads to good outcomes. This case is offered as a contribution to the limited literature on deformity progression associated with solitary osteochondroma and as a reminder that in orthopaedics, the clinical story sometimes has a second chapter.
A solitary osteochondroma can drive progressive, bilateral genu valgum requiring staged surgical correction. Orthopaedic surgeons should maintain active bilateral limb surveillance after unilateral deformity correction, as contralateral progression – even without a structural lesion – may occur and benefit from early intervention.
References
- 1. Murphey MD, Choi JJ, Kransdorf MJ, Flemming DJ, Gannon FH. Imaging of osteochondroma: Variants and complications with radiologic-pathologic correlation. Radiographics 2000;20:1407-34. [Google Scholar] [PubMed]
- 2. Brien EW, Mirra JM, Luck JV Jr. Benign and malignant cartilage tumors of bone and joint: Their anatomic and theoretical basis with an emphasis on radiology, pathology and clinical biology. II. Juxtacortical cartilage tumors. Skeletal Radiol 1999;28:1-20. [Google Scholar] [PubMed]
- 3. Aitchison AH, Alcoloumbre D, Belzarena AC, Blanco JS. Rapidly acquired valgus deformity of the knee after osteochondroma resection in multiple hereditary exostoses pediatric patients: A report of two cases. Radiol Case Rep 2022;17:201-7. [Google Scholar] [PubMed]
- 4. Kitsoulis P, Galani V, Stefanaki K, Paraskevas G, Karatzias G, Agnantis NJ, et al. Osteochondromas: Review of the clinical, radiological and pathological features. In Vivo 2008;22:633-46. [Google Scholar] [PubMed]
- 5. Unni KK. Dahlin’s Bone Tumors: General Aspects and Data on 11,087 Cases. 5th ed. Philadelphia, PA: Lippincott-Raven; 1996. [Google Scholar] [PubMed]
- 6. Paley D. Principles of Deformity Correction. Berlin: Springer; 2002. [Google Scholar] [PubMed]
- 7. Stevens PM. Guided growth for angular correction: A preliminary series using a tension band plate. J Pediatr Orthop 2007;27:253-9. [Google Scholar] [PubMed]
- 8. Park H, Kim HW, Park KB, Kim JH, Chang WJ, Park BK. Effect of solitary osteochondroma on alignment and length in the lower extremities. J Pediatr Orthop 2024;44:e351-6. [Google Scholar] [PubMed]
- 9. Bram JT, Li DT, Tracey OC, Lijesen E, Chipman DE, Widmann RF, et al. Hemiepiphysiodesis for genu valgum in patients with multiple hereditary exostoses. J Pediatr Orthop 2024;44:e406-10. [Google Scholar] [PubMed]
- 10. King EA, Hanauer DA, Choi SW, Jong N, Hamstra DA, Li Y, et al. Osteochondromas after radiation for pediatric malignancies: A role for expanded counseling for skeletal side effects. J Pediatr Orthop 2014;34:331-5. [Google Scholar] [PubMed]
- 11. Denduluri SK, Lu M, Bielski RJ. Development of genu valgum after removal of osteochondromas from the proximal tibia. J Pediatr Orthop B 2016;25:582-6. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report
August 1, 2026 Vanishing Osteochondromas of the Distal Femur and Proximal Humerus: A Two-Case Report February 1, 2026 A Rare Case of Calcaneal Osteochondroma: Case Report
February 1, 2026 A Rare Case of Calcaneal Osteochondroma: Case Report November 1, 2025 Distal Fibula Osteochondroma with Peroneal Tendon Subluxation – A Case Report
November 1, 2025 Distal Fibula Osteochondroma with Peroneal Tendon Subluxation – A Case Report December 1, 2024 Challenges and Solutions in Managing Recurrent Distal Tibia Interosseous Osteochondroma: A Case Study and Review of Literature
December 1, 2024 Challenges and Solutions in Managing Recurrent Distal Tibia Interosseous Osteochondroma: A Case Study and Review of Literature