
• Multimodal imaging is essential to differentiate mechanical from intrinsic causes of dysphagia • Anterior osteophytectomy effectively restores esophageal patency in cervical DISH • Validated dysphagia metrics (FOIS, EAT-10, MDADI) and PVST improve outcome transparency • Long-term recurrence is rare but should be monitored.
Dr. B M Santhan Kumar Reddy, Department of Orthopaedic Surgery, Ramaiah Medical College and Hospital, Bengaluru, Karnataka, India. E-mail: kumarreddysanthan@gmail.com
Abstract
Introduction: Diffuse idiopathic skeletal hyperostosis (DISH) is a non-inflammatory enthesopathic disorder characterised by flowing ossification along the spine. Cervical involvement may compress the aerodigestive tract, causing dysphagia, aspiration risk, and malnutrition.
Case Report: An 82-year-old male presented with 9 months of progressive dysphagia and odynophagia, eventually intolerant even of liquids, with ~10 kg weight loss. Radiographs demonstrated flowing anterior ossification from C2 to C7; a barium swallow confirmed bolus hold-up at C5–C6; computed tomography (CT) revealed bulky ventral osteophytes; and magnetic resonance imaging (MRI) excluded myelopathy. Following failed conservative management, anterior cervical osteophytectomy (C3–C7) was performed. Objective outcomes measured pre-operative, at 1 month post-operative, and at 2-year follow-up improved from Functional Oral Intake Scale 2 → 6 → 7, Eating Assessment Tool-10 32 → 8 → 2, M.D. Anderson Dysphagia Inventory global 48 → 86, and Prevertebral Soft Tissue 2.6 mm → 5.1 mm → 3.9 mm, with full dietary normalisation and no recurrence at 2-year follow-up.
Discussion: The diagnostic pathway (radiographs → barium swallow → CT ± MRI) aligns with commonly recommended approaches for evaluating mechanical dysphagia. Surgical osteophytectomy is highly effective, with ~95% improvement and ~4% symptomatic recurrence reported in systematic reviews.
Conclusion: Timely recognition and osteophytectomy for severe cervical DISH can restore complete functional swallowing, objectively verified across validated outcome measures, with durable remission at 2 years.
Keywords: Diffuse idiopathic skeletal hyperostosis, dysphagia, cervical osteophyte, osteophytectomy, FOIS, EAT-10, MDADI, PVST.
Diffuse idiopathic skeletal hyperostosis (DISH) is a non-inflammatory condition marked by ligamentous ossification, most prevalent in older males and strongly associated with metabolic syndrome [1,2]. Forestier and Rotes-Querol initially characterised DISH in 1950, referring to it as “ankylosing hyperostosis” [3]. Its classic definition by Resnick–Niwayama describes flowing ossification across ≥4 contiguous vertebrae with preserved disc height [4]. The cause of DISH remains obscure and is suspected to involve a combination of genetic factors, metabolic processes, and inflammatory mechanisms [2,5]. The hallmark of this disease is the development of new bone, partly in entheses The hallmark of this disease is the development of new bone, partly in entheses [5]. Although DISH is relatively common in older adults (global prevalence ≈12%), clinically significant aerodigestive compromise from cervical osteophytes remains uncommon – among patients presenting with dysphagia, ~10.6% have cervical osteophytes, and only ~17% of individuals with cervical osteophytes develop dysphagia [6]. The bone formation associated with DISH may result in alterations to the musculoskeletal system’s biomechanics and the development of obstructive cervical masses. [7,8]. Cervical DISH may cause extrinsic mechanical oesophageal compression and progressive dysphagia. When conservative measures fail, anterior cervical osteophytectomy is the standard surgical treatment and is reported to provide high rates of symptomatic resolution [9].
Chief complaint and presenting illness
An 82-year-old male presented with 9 months of progressive mechanical dysphagia, initially for solids and later for liquids, accompanied by odynophagia and an unintentional 10-kg weight loss. He denied symptoms of reflux, neurological deficits, or respiratory compromise.
Prior conservative management
Before specialty referral, he had undergone trials of diet modification, non-steroidal anti-inflammatory drugs, and swallow therapy, but symptoms continued to worsen, and oral intake declined substantially. His nutritional state deteriorated, with a body mass index of 18.4, albumin of 2.9 g/dL, and pre-albumin of 14 mg/dL, indicating significant malnutrition.
Clinical examination
On examination, he exhibited marked cervical rigidity (range of motion <15°) and paraspinal hypertonicity, whereas the neurological examination remained normal. Speech–language pathology assessment showed severe functional impairment with FOIS 2, EAT-10 score 32, and MDADI global 48/composite 52.
Diagnostic Assessment
Plain cervical radiographs demonstrated flowing anterior ossification from C2 to C7, consistent with DISH. (Figure 1)
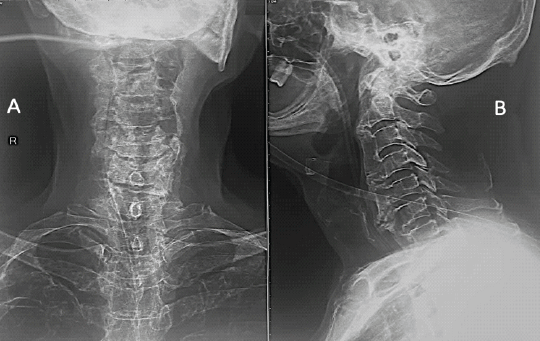
Figure 1: (a and b) Anteroposterior and lateral radiographs of the cervical spine demonstrating exuberant anterior osteophyte formation along the anterior longitudinal ligament extending from C2 to C7.
Barium swallow revealed contrast hold-up at C5–C6 with proximal esophageal dilatation.(Figure 2)
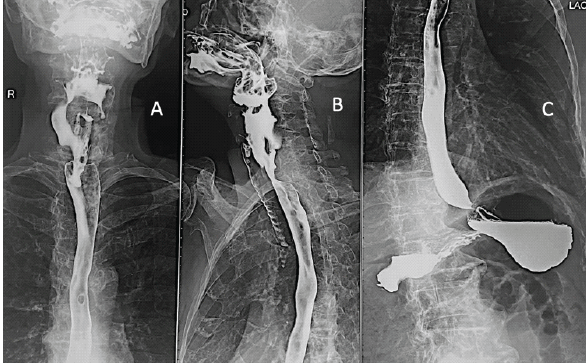
Figure 2: (a-c) Barium swallow radiographs demonstrating reduced passage of contrast at the level of C5–C6 with proximal esophageal hold-up.
CT cervical spine confirmed bulky ventral osteophyte formation projecting ~12 mm anteroposterior at C5–C6, causing significant esophageal indentation. Magnetic resonance imaging (MRI) ruled out cervical myelopathy or mass lesions. No significant MRI abnormality – images omitted for brevity. There was no clinical or endoscopic evidence of malignancy. (Figure 3)
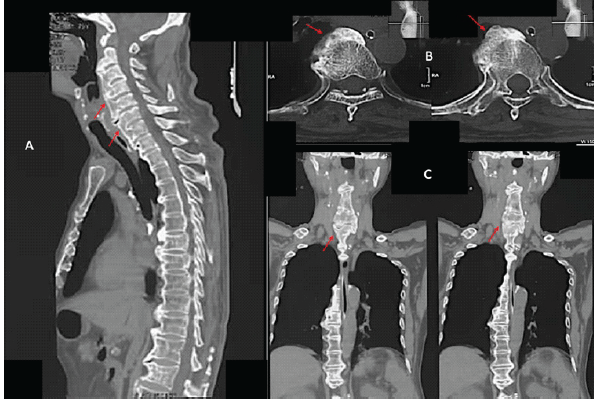
Figure 3: (a-c) Computed tomography images of the cervical spine. Sagittal reconstruction (a) demonstrates continuous ossification and anterior osteophyte formation along the anterior longitudinal ligament from C2 to C7. Axial (b) and coronal (c) views show prominent ventral osteophytes projecting anterior to the vertebral bodies.
Imaging rationale
This diagnostic sequence is consistent with commonly recommended approaches for evaluating mechanical dysphagia.
Therapeutic Intervention
Given progressive obstructive dysphagia, failure of adequate conservative therapy, severe nutritional compromise, and imaging confirming mechanical obstruction, a multidisciplinary team recommended anterior cervical osteophytectomy.
Procedure
A standard anterior cervical osteophytectomy allowed exposure of a thinned tracheoesophageal complex. With recurrent laryngeal nerve protection, osteophytes from C3 to C7 were excised using Kerrison rongeurs and fine osteotomes. Estimated blood loss <50 mL. No complications occurred.
No segmental instability was identified, and fusion was not required.
Post-operative Rehabilitation and Outcomes
A staged swallow rehabilitation protocol was followed: Clear liquids post operative day 2 → semisolids week 3 → full solid diet week 4.
Interpretation
- FOIS improvement from 2 → 7 indicates full dietary normalization
- EAT-10 reduction from 32 → 2 shows near-complete resolution of symptoms
- MDADI global/composite scores show major quality of life (QOL) gains
- PVST increase reflects restored retropharyngeal space after osteophytectomy. Normal PVST at C5–C6 is approximately 3–7 mm.
At 2 years:
- No dysphagia, no aspiration, full unrestricted diet, stable weight gain, normal QOL.
- No recurrence of symptoms (consistent with low recurrence rates in literature).
The slight reduction in PVST at final follow-up remained within normal limits and was not associated with symptom recurrence.
- Table 1 summarizes the timeline of events
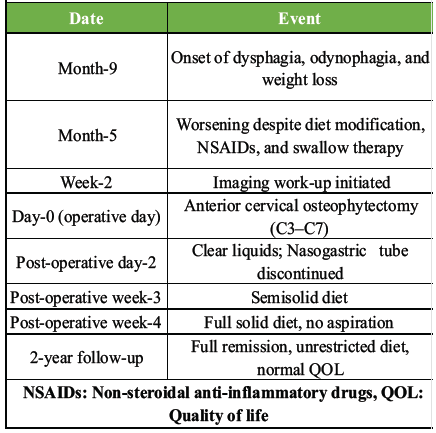 Table 1: Timeline of events
Table 1: Timeline of events
- Table 2 shows prospectively tracked objective outcome measures.
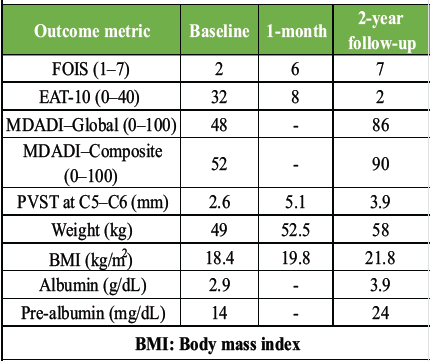 Table 2: Objective outcomes (Baseline→1-month→2-year follow-up)
Table 2: Objective outcomes (Baseline→1-month→2-year follow-up)
This patient’s presentation – progressive dysphagia with marked weight loss – illustrates a classic but relatively uncommon symptomatic manifestation of cervical DISH, as most individuals with radiographic DISH remain asymptomatic. Diagnosis required correlating functional swallow imaging with anatomical definition on computed tomography (CT), in line with commonly recommended approaches for evaluating mechanical dysphagia.
When conservative treatment fails, anterior cervical osteophytectomy is well established, with systematic reviews reporting approximately 95% symptom improvement and ~4% symptomatic recurrence after surgery. The outcomes in our case were consistent with these data, demonstrating complete resolution of dysphagia, restoration of normal diet, and sustained recovery at 2 years [9].
Comparison with major published case series
Findings from this case parallel trends described in the largest updated systematic review by Harlianto et al. (2022), which analyzed 419 patients with cervical DISH-related dysphagia and airway compromise. The review highlighted that symptomatic cases typically involve older males and frequently demonstrate multilevel ventral ossification – patterns reflected in the extensive C2–C7 involvement observed here. Moreover, post-operative improvement was reported in 95.5% of patients, with a 4% recurrence rate, again matching the durable remission in this case. Complementary epidemiologic summaries, including the synthesis presented in the American Academy of Otolaryngology–Head and Neck Surgery review, emphasize that only a small proportion of individuals with cervical osteophytes develop clinically significant dysphagia, situating this case within the recognized but infrequent severe end of the spectrum [10,11].
Unique strength of this case
A key distinguishing feature of this report is the comprehensive use of multiple validated dysphagia outcome measures – FOIS, EAT-10, MDADI, and PVST – captured both preoperatively and longitudinally. Such a structured functional assessment is rarely reported together in DISH literature, which traditionally relies on subjective symptomatic descriptions. By integrating quantitative swallow metrics with imaging and long-term follow-up, this case provides one of the more detailed quantifiable functional outcome profiles published for cervical DISH.
Differential diagnosis
Differential considerations for obstructive dysphagia include neoplastic pharyngo‑esophageal or thyroid masses, cricopharyngeal bar or upper esophageal sphincter dysfunction, Zenker diverticulum, retropharyngeal inflammatory or infectious processes, and neuromuscular causes such as stroke or Parkinson’s disease. In this patient, the combination of flowing anterior ossification from C2 to C7 on radiographs, ventral indentation at C5–C6 on barium swallow, and bulky anterior osteophytes on CT without any soft-tissue mass, together with failed conservative therapy, strongly supported mechanical obstruction from cervical DISH over alternative diagnoses.
Cervical DISH can cause severe, progressive dysphagia with the risk of malnutrition. Comprehensive imaging and timely surgical osteophytectomy led to full, objectively documented functional recovery, with complete remission maintained at 2 years.
Severe mechanical dysphagia and aerodigestive compromise secondary to cervical diffuse idiopathic skeletal hyperostosis (DISH) can be effectively managed with anterior cervical osteophytectomy, yielding durable functional recovery that is best evaluated through multimodal imaging and validated swallow metrics.
References
- 1. Kaur J, Virk JS. Dysphagia due to DISH-related anterior osteophytes: DISHphagia!! BMJ Case Rep 2017;2017:bcr-2017-222512. [Google Scholar] [PubMed]
- 2. Mader R, Verlaan JJ, Buskila Diffuse idiopathic skeletal hyperostosis: clinical features and pathogenic mechanisms. Nat Rev Rheumatol 2013;9:741–50. [Google Scholar] [PubMed]
- 3. Forestier J, Rotes-Quero Senile vertebral ankylosing hyperostosis. Rev Rhum Mal Osteoartic. 1950;17:525–34. [Google Scholar] [PubMed]
- 4. Resnick D, Niwayama G. Radiographic and pathologic features of spinal involvement in diffuse idiopathic skeletal hyperostosis (DISH). Radiology 1976;119:559-68. [Google Scholar] [PubMed]
- 5. Nascimento FA, Gatto LA, Lages RO, Mello Neto H, Demartini Junior Z, Koppe GL, et al. Diffuse idiopathic skeletal hyperostosis: A review. Surg Neurol Int. 2014;5:S122–5. [Google Scholar] [PubMed]
- 6. Weng R, Guo H, Ma L, Lin T, Han W, Zhong X, et al. Global prevalence estimates of diffuse idiopathic skeletal hyperostosis: A systematic review and meta-analysis. Front Endocrinol (Lausanne) 2025;16:1517168. [Google Scholar] [PubMed]
- 7. Harlianto NI, Kuperus JS, Mohamed Hoesein FA, Ade Jong PA, de Ru JA Öner FC, et al. Diffuse idiopathic skeletal hyperostosis of the cervical spine causing dysphagia and airway obstruction: an updated systematic review. Spine J. 2022;22:1490–503. [Google Scholar] [PubMed]
- 8. Verlaan JJ, Boswijk PF, de Ru JA, Dhert WJ, AÖner Diffuse idiopathic skeletal hyperostosis of the cervical spine: an underestimated cause of dysphagia and airway obstruction. Spine J 2011;11:1058–67. [Google Scholar] [PubMed]
- 9. Choi HY, Jo DJ. Surgical treatment of dysphagia secondary to anterior cervical osteophytes due to diffuse idiopathic skeletal hyperostosis. Medicina (Kaunas) 2022;58:928. [Google Scholar] [PubMed]
- 10. Harlianto NI, Kuperus JS, Mohamed Hoesein FA, De Jong PA, De Ru JA, Öner FC, et al. Diffuse idiopathic skeletal hyperostosis of the cervical spine causing dysphagia and airway obstruction: An updated systematic review. Spine J 2022;22:1490-503. [Google Scholar] [PubMed]
- 11. Belanger TA, Rowe DE. Diffuse idiopathic skeletal hyperostosis: Musculoskeletal manifestations. J Am Acad Orthop Surg 2001;9:258-67. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Anterior Cervical Discectomy and Fusion with Polyetheretherketone Cage or Anterior Cervical Plate: A Comparative Evaluation of Short-term Outcomes
April 1, 2026 Anterior Cervical Discectomy and Fusion with Polyetheretherketone Cage or Anterior Cervical Plate: A Comparative Evaluation of Short-term Outcomes September 10, 2021 Treatment of Unstable Sacral Fracture with Minimally Invasive Spinopelvic Posterior Fixation and an Internal Anterior Fixator in a 95-Year-Old Patient with Diffuse Idiopathic Skeletal Hyperostosis: A Case Report
September 10, 2021 Treatment of Unstable Sacral Fracture with Minimally Invasive Spinopelvic Posterior Fixation and an Internal Anterior Fixator in a 95-Year-Old Patient with Diffuse Idiopathic Skeletal Hyperostosis: A Case Report July 30, 2019 Non-Identical Bilateral Rupture of the Extensor Mechanism of the Knee in a Patient with Hyperlipidemia: A Case Study
July 30, 2019 Non-Identical Bilateral Rupture of the Extensor Mechanism of the Knee in a Patient with Hyperlipidemia: A Case Study November 1, 2024 Minimally Invasive Percutaneous Plate Osteosynthesis with Proximal Humerus Locking Plate for Pediatric Comminuted Subtrochanteric Femur Fracture: A Case Report
November 1, 2024 Minimally Invasive Percutaneous Plate Osteosynthesis with Proximal Humerus Locking Plate for Pediatric Comminuted Subtrochanteric Femur Fracture: A Case Report