
A vascularized first dorsal metacarpal artery-based adipofascial flap may reduce adhesions after multiple zone VII extensor tendon repairs
Dr Raghavendra R. Vyas, Department of Orthopaedics, Hand and Microvascular Surgery, Sanjeevani Vyas Hospital and Anusandhan Kendra Pvt. Ltd, Jhalawar, Rajasthan, India. E-mail: raghavendravyas@gmail.com
Abstract
Introduction: Multiple extensor tendon repairs may be complicated by adhesions, retear, stiffness, and loss of range of motion, especially when supervised hand therapy and regular follow-up are difficult. We report a simple technique using a vascularized adipofascial flap based on the first dorsal metacarpal artery to cover the repair site and create a biologically favorable gliding tunnel.
Case Report: An 18-year-old manual worker sustained glass lacerations over extensor zone VII of the wrist with complete transection of the thumb and finger extensor tendons. The tendons were repaired primarily and augmented with a vascularized adipofascial flap based on the first dorsal metacarpal artery, which was wrapped around the repair site as a gliding tunnel. At 6 weeks, the patient had full active finger and thumb extension and flexion without lag, and he returned to heavy activity by 12 weeks.
Conclusion: This local flap may provide a low-cost, vascularized interface that supports tendon healing and limits adhesion after complex dorsal wrist tendon injury, particularly where supervised hand therapy access is limited.
Keywords: Adipofascial flap, extensor tendon injury, first dorsal metacarpal artery, tendon adhesion, tendon repair, zone VII.
Extensor tendon injuries are common in hand surgery and require accurate diagnosis, meticulous repair, protected mobilization, and coordinated rehabilitation to restore motion [1,2,3]. The superficial course of the extensor tendons over the dorsum of the wrist and hand makes them vulnerable to deep-structure injury even after apparently small penetrating lacerations [4]. After tendon repair, the desired outcome is a repair that is strong enough to permit safe, controlled motion while maintaining a smooth gliding interface. Early protected motion and modern biomechanical repair concepts have improved outcomes, but multiple tendon injuries remain susceptible to adhesion, stiffness, retear, and loss of range of motion [3,5,6,7,8,9]. Biologic strategies such as growth factors, stem cell-based approaches, and natural or synthetic biomaterials have been proposed to enhance tendon healing; however, these may be costly and are often unavailable in resource-constrained settings [10]. We describe an unusual glass laceration involving multiple extensor tendons in zone VII that was treated with primary tendon repair and augmentation using a vascularized adipofascial flap based on the first dorsal metacarpal artery. The flap was fashioned as a tunnel around the repaired tendons to create a local vascularized gliding interface.
The patient was informed that clinical data and images would be submitted for publication and gave written consent. The patient was an 18-year-old male manual worker who presented to the emergency department after a road traffic accident. He had sustained glass lacerations from a broken windshield over the dorsum of the left wrist and hand. On examination, there were two apparently benign wounds, each approximately 4 × 3 × 0.5 cm, over extensor zone VII (Fig. 1).

Figure 1: Clinical photograph showing two lacerated wounds over the dorsum of the left wrist and hand in extensor zone VII.
Active flexion of the fingers and thumb was preserved, but active extension of all four fingers and the thumb was absent (Fig. 2).

Figure 2: Pre-operative clinical photograph demonstrating the inability to actively extend the fingers and thumb.
There was no major active bleeding. The wound was irrigated and dressed, and a below-elbow plaster slab was applied. After informed consent, surgical exploration was performed under general anesthesia. The lacerations were extended and explored under loupe magnification. All extensor tendons at zone VII were transected (Fig. 3). Multiple retained glass fragments were removed (Fig. 4).

Figure 3: Intra-operative photograph showing complete transection of the extensor tendons in zone VII after wound exploration.

Figure 4: Removed glass fragments from the wound.
The extensor tendons were repaired primarily with 3-0 polypropylene sutures using a modified Kessler technique (Fig. 5).

Figure 5: Primary repair of multiple extensor tendons using 3-0 Prolene with a modified Kessler technique.
After confirming satisfactory tendon repair, a vascularized adipofascial flap based on the first dorsal metacarpal artery was elevated by blunt dissection with fine tenotomy scissors and bipolar cautery (Fig. 6). Good bleeding from the flap confirmed vascularity (Fig. 7).
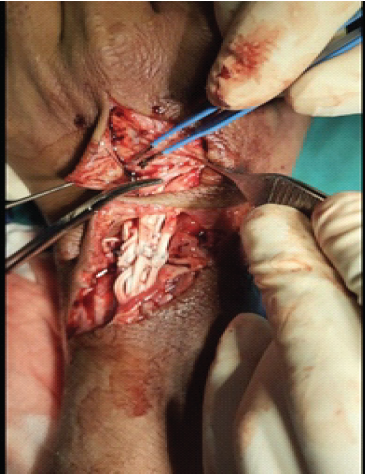
Figure 6: Elevation of the vascularized adipofascial flap based on the first dorsal metacarpal artery.

Figure 7: Intra-operative confirmation of flap vascularity, showing bleeding from the harvested flap.
The flap was mobilized and wrapped around the repair site in the form of a tunnel, with the fatty layer oriented toward the tendons and the fascial layer outward. The flap was secured with 4-0 polyglactin sutures (Fig. 8).
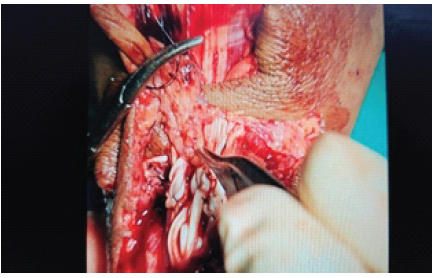
Figure 8: Vascularized adipofascial flap wrapped around the repaired extensor tendons to create a gliding tunnel.
Free gliding of the tendons through the tunnel was confirmed by passive finger motion. The wound was irrigated and closed in layers. A volar splint was applied with the wrist, hand, and fingers in functional position. Sutures were removed on post-operative day 12, and the slab was converted to a flexion-blocking splint with the wrist, hand, and fingers in neutral position (Fig. 9).

Figure 9: Post-operative splinting after suture removal and conversion to a flexion-block splint.
The patient was instructed to perform protected finger motion within the splint, including gentle active extension against the splint. At 6 weeks, the splint was removed. The patient demonstrated complete active extension and flexion of all fingers and the thumb, with good power against resistance and no extensor lag (Fig. 10). At 12 weeks, during telephone follow-up, he reported return to heavy manual activity with normal hand function.
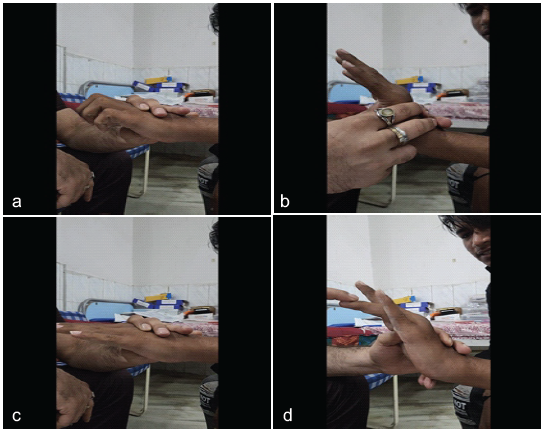
Figure 10: (a, b, c, d) Six-week follow-up clinical photographs showing active extension and flexion of all fingers and the thumb with good functional recovery and no extension lag.
Zone VII extensor tendon injuries present a distinct reconstructive challenge because the finger and thumb extensors converge at the dorsum of the wrist, pass beneath the extensor retinaculum, and then diverge toward their individual digital insertions [11,12,13,14,15,16]. In this region, restoration of tendon continuity alone is not sufficient; the surgeon must also restore the capacity for independent tendon excursion through a narrow, scar-prone, mechanically active tunnel. This is particularly important when multiple tendons are injured simultaneously, because tethering of even one repair can disturb composite wrist, finger, and thumb extension. The case also emphasises the deceptive nature of dorsal wrist and hand lacerations. Extensor tendons are superficially located and are covered by relatively thin soft tissue, making them vulnerable to glass, sharp metal, and other penetrating injuries [4,12,16]. Small wounds may therefore hide major deep-structure damage. In our patient, two apparently benign-looking dorsal wounds were associated with complete transection of the thumb and finger extensor tendons. This underlines the importance of assessing active extension of each digit and the thumb against gravity and resistance, rather than judging severity from wound size alone. Diagnosis may be further complicated by the anatomical interconnections between the extensor tendons. The juncturae tendinum can transmit extension force from adjacent intact tendons and may partially mask the functional deficit after a single tendon injury [11,17]. In multiple tendon injuries, however, this compensatory mechanism may be overwhelmed, as occurred in the present case. The surgeon should still assess each tendon independently during exploration, because the pattern of injury may not be obvious from the external wound, especially when glass fragments and contused wound edges are present. Prompt exploration is important in acute open injuries because retained foreign bodies, devitalised tissue, and tendon-end contamination can contribute to infection, stiffness, and impaired tendon gliding. In the present case, removal of glass fragments, wound lavage, loupe-assisted identification of all transected tendons, and primary repair were performed in the same sitting. Early definitive management also prevented tendon retraction and gap formation, which are important reasons why delayed or neglected extensor tendon injuries may require grafting or staged reconstruction rather than direct repair [11,18,19]. A strong primary repair remains the foundation of treatment. Clinical and biomechanical studies have compared several extensor tendon suture techniques, including running interlocking and horizontal mattress methods, with the objective of improving resistance to gap formation while avoiding excessive bulk at the repair site [3,6,7,8,9,13,16]. The extensor tendons are flatter and thinner than flexor tendons in many zones, and they may not tolerate bulky repairs. Therefore, the repair must balance strength, smoothness, and preservation of tendon length. In this case, the modified Kessler repair restored continuity, while the flap was used only as an adjunct to improve the local biological and mechanical environment. The need for a repair strong enough to permit protected motion is well established in the extensor tendon literature. Immobilisation protects the repair but encourages stiffness, oedema, scar maturation, and tendon adherence. Early controlled motion, when performed safely, can improve tendon excursion and hasten early functional recovery [5,19,20,21,22,23,24,25,26,27]. Patil and Koul, in a prospective randomised trial of extrinsic extensor tendon repairs, found better early total active motion and earlier return to work with early active mobilisation than with immobilisation, although long-term differences decreased [21]. Similarly, Saini et al. reported good results with an active mobilisation plan using a simple static splint [22]. Systematic reviews and contemporary rehabilitation papers also support early active mobilisation protocols after zone V and VI extensor tendon repair, while recognising that protocols differ and must be individualised [23,27]. Relative motion extension orthoses, immediate controlled active motion programmes, and short-arc motion concepts have been developed to allow safe tendon excursion while reducing tension at the repair site [24,25,26,28]. These strategies are relevant to zone VII injuries because early movement must be balanced against the risk of gapping or rupture, particularly when several tendons have been repaired together. However, the success of these rehabilitation protocols depends on factors that are often outside the operating room: Access to a trained hand therapist, availability of custom orthoses, patient education, travel distance, occupational demands, and adherence to restrictions. Manual workers may have economic pressure to resume activity early, and patients in rural or resource-limited settings may be unable to attend frequent therapy visits. The technique described in this report should not be interpreted as a replacement for rehabilitation but as a biological adjunct that may make the repair environment more forgiving when ideal supervised therapy cannot be guaranteed. Adhesion formation is the central biological problem that this technique attempts to address. Tendon healing involves inflammatory, proliferative, and remodelling phases, and functional outcome depends on the balance between intrinsic tendon healing and extrinsic scar ingrowth [6,29]. Excessive peritendinous scarring can tether the repair, reduce excursion, and produce extensor lag or loss of flexion. This is especially concerning in zone VII, where the extensor retinaculum and surrounding scar can limit independent gliding of multiple tendons within a confined space [2,16,27]. Several anti-adhesion strategies have been proposed in hand surgery, including hyaluronic acid-based products, amniotic membrane, acellular dermal matrix, absorbable films, pharmacologic agents, and other biomaterials [6,29]. Although some studies suggest improvements in range of motion with selected barriers, a recent systematic review of anti-adhesion agents in hand trauma concluded that high-quality clinical evidence remains limited and that further research is needed [29]. For many centres, the additional cost and availability of commercial barriers remain practical obstacles. The concept of using vascularised adipofascial tissue is attractive because it combines a physical gliding layer with a living biological interface. Adipofascial flaps have been used to reduce adhesions between plates and the extensor apparatus after proximal phalanx fixation, and comparative work has suggested improved total active motion when an adipofascial flap is interposed [30,31]. Del Pinal et al. also reported that vascularised free adipofascial flaps combined with tenolysis improved the local environment in scarred beds, with all flaps surviving and active motion approximating the passive motion obtained intraoperatively [32]. The present technique applies that principle at the time of acute primary tendon repair rather than during secondary tenolysis. By wrapping a vascularised adipofascial flap around the repaired tendons, the surgeon creates a soft biological tunnel. The adipose surface facing the tendons may reduce friction, while the fascial surface outward may separate the repair from the surrounding scarbed. Vascularised tissue may also support local healing and tissue remodelling, although this proposed benefit requires formal study in a larger clinical series. The first dorsal metacarpal artery provides a useful local vascular axis in the same operative region. Reviews of the first dorsal metacarpal artery flap family describe it as a versatile and reliable option in hand reconstruction, particularly for local soft-tissue coverage, because of its relatively constant anatomy and ease of elevation [33]. In the present case, the flap was not used as a skin flap for external coverage; instead, it was harvested as an adipofascial flap and transposed internally to wrap the tendon repair site. This modification allowed the flap to be used without adding a distant donor site or microsurgical anastomosis. Several technical points are important. The flap should be raised gently with preservation of its vascular pedicle, and bleeding from the flap should be confirmed before the inset. The adipose surface should face the repaired tendons, and the tunnel should be loose enough to permit free tendon glide without constriction. After the inset, passive finger and thumb movement should be performed intraoperatively to ensure that the repaired tendons glide freely within the tunnel and that the flap does not create a mechanical block. The clinical recovery in this patient was encouraging. At 6 weeks, the patient had complete active flexion and extension of the fingers and thumb without extensor lag, and at 12 weeks, he reported a return to heavy manual activity. These findings compare favourably with the major functional concerns described after extensor tendon repair, including extensor lag, stiffness, adhesions, rupture, and delayed return to work [1,3,16,21,22,23,34,35,36]. The result is also clinically meaningful because all finger extensors and the thumb extensor mechanism were involved at the wrist level. Nevertheless, the favourable outcome cannot be attributed solely to the adipofascial flap. The result likely reflects a combination of acute presentation, adequate debridement, removal of glass fragments, complete primary repair, vascularised interposition, protective splinting, and patient-performed controlled movement. It is also possible that a similar patient could have achieved a good result with conventional repair and an excellent rehabilitation programme. Therefore, this report should be viewed as a proof-of-concept technical case rather than evidence of superiority. This report has several limitations. It describes a single patient with short-term follow-up and lacks validated patient-reported outcome measures, total active motion measurement, grip-strength testing, ultrasound assessment of tendon gliding, and comparison with repair alone. Future work should include a prospective case series with standardised functional scoring, serial range-of-motion measurements, documentation of therapy access and compliance, and longer follow-up. Comparative studies would be required to determine whether this vascularised gliding tunnel reduces adhesion formation, therapy dependence, secondary tenolysis, or time to return to work. Despite these limitations, the technique is simple, local, economical, and biologically plausible. It may be considered in selected acute multiple zone VII extensor tendon injuries when the repair lies in a scar-prone bed, when many tendons require simultaneous repair, or when the surgeon anticipates difficulty with frequent supervised rehabilitation. Its main value is not to replace careful repair and hand therapy but to add a living, low-friction, vascularised interface around the repaired tendons.
Primary repair of multiple zone VII extensor tendon injuries can be augmented with a local vascularised adipofascial flap based on the first dorsal metacarpal artery. In this patient, the flap was used as a gliding tunnel around the repaired tendons and was followed by early recovery of active extension and flexion. The method may be considered when surgeons wish to add a low-cost vascularised interface in complex dorsal wrist tendon injuries, particularly where access to intensive hand therapy is limited.
In acute multiple zone VII extensor tendon lacerations, a first dorsal metacarpal artery-based vascularised adipofascial flap can be wrapped around primary tendon repairs to create a local gliding tunnel and may help limit adhesions and provide a vascular environment to promote healing, particularly when access to intensive supervised hand therapy is limited.
References
- 1. Matzon JL, Bozentka DJ. Extensor tendon injuries. J Hand Surg Am 2010;35:854-61. [Google Scholar] [PubMed]
- 2. Griffin M, Hindocha S, Jordan D, Saleh M, Khan W. Management of extensor tendon injuries. Open Orthop J 2012;6:36-42. [Google Scholar] [PubMed]
- 3. Dy CJ, Rosenblatt L, Lee SK. Current methods and biomechanics of extensor tendon repairs. Hand Clin 2013;29:261-8. [Google Scholar] [PubMed]
- 4. Tuncali D, Yavuz N, Terzioglu A, Aslan G. The rate of upper-extremity deep-structure injuries through small penetrating lacerations. Ann Plast Surg 2005;55:146-8. [Google Scholar] [PubMed]
- 5. Crosby CA, Wehbé MA. Early protected motion after extensor tendon repair. J Hand Surg Am 1999;24:1061-70. [Google Scholar] [PubMed]
- 6. Altobelli GG, Conneely S, Haufler C, Walsh M, Ruchelsman DE. Outcomes of digital zones IV and V and thumb zone TI to TIV extensor tendon repairs using a running interlocking horizontal mattress technique. J Hand Surg Am 2013;38:1079-83. [Google Scholar] [PubMed]
- 7. Lee SK, Dubey A, Kim BH, Zingman A, Landa J, Paksima N. A biomechanical study of extensor tendon repair methods: Introduction to the running-interlocking horizontal mattress extensor tendon repair technique. J Hand Surg Am 2010;35:19-23. [Google Scholar] [PubMed]
- 8. Woo SH, Tsai TM, Kleinert HE, Chew WY, Voor MJ. A biomechanical comparison of four extensor tendon repair techniques in zone IV. Plast Reconstr Surg 2005;115:1674-81. [Google Scholar] [PubMed]
- 9. Newport ML, Pollack GR, Williams CD. Biomechanical characteristics of suture techniques in extensor zone IV. J Hand Surg Am 1995;20:650-6. [Google Scholar] [PubMed]
- 10. Wu F, Nerlich M, Docheva D. Tendon injuries: Basic science and new repair proposals. EFORT Open Rev 2017;2:332-42. [Google Scholar] [PubMed]
- 11. Rohith K, Nellaiyappan B, Subashini R. Neglected but negotiated – a case report of multiple Zone VII extensor tendon injuries reconstructed using a fascia lata autograft. J Orthop Case Rep 2026;16:498-502. [Google Scholar] [PubMed]
- 12. Kontor JA. Extensor tendon injuries and repairs in the hand. Can Fam Physician 1982;28:1159-63. [Google Scholar] [PubMed]
- 13. Newport ML, Williams CD. Extensor tendon injuries. Hand Clin 1995;11:373-86. [Google Scholar] [PubMed]
- 14. Kleinert HE, Verdan C. Report of the committee on tendon injuries (international federation of societies for surgery of the hand). J Hand Surg Am 1983;8:794-8. [Google Scholar] [PubMed]
- 15. Wehbe MA, Schneider LH. Extensor tendon injuries. Clin Orthop Relat Res 1984;183:75-90. [Google Scholar] [PubMed]
- 16. Colzani G, Tos P, Battiston B, Merolla G, Porcellini G, Artiaco S. Traumatic extensor tendon injuries to the hand: Clinical anatomy, biomechanics, and surgical procedure review. J Hand Microsurg 2016;8:2-12. [Google Scholar] [PubMed]
- 17. Landsmeer JM. The anatomy of the dorsal aponeurosis of the human finger and its functional significance. Anat Rec 1949;104:31-44. [Google Scholar] [PubMed]
- 18. Green DP, Hotchkiss RN, Pederson WC, Wolfe SW. Green’s Operative Hand Surgery. 6th, Philadelphia, PA: Elsevier Churchill Livingstone; 2011. p. 187-215. [Google Scholar] [PubMed]
- 19. Sylaidis P, Youatt M, Logan A. Early active mobilisation for extensor tendon injuries. The Norwich regime. J Hand Surg Br 1997;22:594-6. [Google Scholar] [PubMed]
- 20. Chester DL, Beale S, Beveridge L, Nancarrow JD, Titley OG. A prospective, controlled, randomised trial comparing early active extension with passive extension using a dynamic splint in the rehabilitation of repaired extensor tendons. J Hand Surg Br 2002;27:283-8. [Google Scholar] [PubMed]
- 21. Patil RK, Koul AR. Early active mobilisation versus immobilisation after extrinsic extensor tendon repair: A prospective randomised trial. Indian J Plast Surg 2012;45:29-37. [Google Scholar] [PubMed]
- 22. Saini N, Sharma M, Sharma VD, Patni P. Outcome of early active mobilisation after extensor tendon repair. Indian J Orthop 2008;42:336-41. [Google Scholar] [PubMed]
- 23. Collocott SJ, Kelly E, Ellis RF. Optimal early active mobilisation protocol after extensor tendon repairs in zones V and VI: A systematic review of literature. Hand Ther 2018;23:3-18. [Google Scholar] [PubMed]
- 24. Howell JW, Merritt WH, Robinson SJ. Immediate controlled active motion following zone 4-7 extensor tendon repair. J Hand Ther 2005;18:182-90. [Google Scholar] [PubMed]
- 25. Evans RB. Immediate active short arc motion following extensor tendon repair. Hand Clin 1995;11:483-512. [Google Scholar] [PubMed]
- 26. Hirth MJ, Howell JW, O’Brien L. Relative motion orthoses in the management of various hand conditions: A scoping review. J Hand Ther 2016;29:405-32. [Google Scholar] [PubMed]
- 27. Canham CD, Hammert WC. Rehabilitation following extensor tendon repair. J Hand Surg Am 2013;38:1615-7. [Google Scholar] [PubMed]
- 28. Merritt WH, Wong AL, Lalonde DH. Recent developments are changing extensor tendon management. Plast Reconstr Surg 2020;145:617-28e. [Google Scholar] [PubMed]
- 29. Forbes KE, Cavallaro D, Power D. A systematic review of anti-adhesion agents in hand trauma. Hand (N Y) 2025;20:831-9. [Google Scholar] [PubMed]
- 30. Lucchina S, Maggiulli F, Tos P, Ionac M, Fusetti C. Can an adipofascial flap be used to prevent adhesions after plating of the proximal phalanx? A case report. Chir Main 2015;34:86-90. [Google Scholar] [PubMed]
- 31. Lucchina S, D’Ambrosio A, Fusetti C, Guidi M. The use of an adipofascial flap to prevent extensor tendon adhesions after plating of the proximal phalanx of the fingers: A comparative study. Hand (N.Y.) 2022;17:691-700. [Google Scholar] [PubMed]
- 32. Del Pinal F, Moraleda E, De Piero GH, Ruas JS. Outcomes of free adipofascial flaps combined with tenolysis in scarred beds. J Hand Surg Am 2014;39:269-79. [Google Scholar] [PubMed]
- 33. Couceiro J, De Prado M, Menendez G, Manteiga Z. The first dorsal metacarpal artery flap family: A review. Surg J (N Y) 2018;4:e215-9. [Google Scholar] [PubMed]
- 34. Kumar H, Singh K, Rani P, Boparai RS, Singh J. Evaluation of extensor tendon repair of hand. Int J Orthop Sci 2018;4:377-82. [Google Scholar] [PubMed]
- 35. Pieter J, Adam W. Acute tendon injuries. Orthop Trauma 2019;33:53-61. [Google Scholar] [PubMed]
- 36. Dalton SS, Maharjan LM, Yousuf H, Pientka WF 2nd. Extensor tendon repair outcomes based on zone of injury. Hand (N.Y.) 2024;19:831-6. [Google Scholar] [PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Neglected but Negotiated – A Case Report of Multiple Zone VII Extensor Tendon Injuries Reconstructed Using Fascia Lata Autograft
June 1, 2026 Neglected but Negotiated – A Case Report of Multiple Zone VII Extensor Tendon Injuries Reconstructed Using Fascia Lata Autograft February 1, 2026 Split Peroneus Brevis: An Overlooked Cause of Ankle Dysfunction
February 1, 2026 Split Peroneus Brevis: An Overlooked Cause of Ankle Dysfunction December 1, 2025 Flexor Tendon Injuries in Zone 3: A Comprehensive Review and Case Report on Flexor Digitorum Profundus Rupture of the Middle Finger
December 1, 2025 Flexor Tendon Injuries in Zone 3: A Comprehensive Review and Case Report on Flexor Digitorum Profundus Rupture of the Middle Finger April 10, 2023 Treating Little Finger’s Flexor Profundus Tendon Rupture after Percutaneous K-wire Fixation of a Bennet Fracture – A Case Report
April 10, 2023 Treating Little Finger’s Flexor Profundus Tendon Rupture after Percutaneous K-wire Fixation of a Bennet Fracture – A Case Report