
Bilateral clavicle fractures are rare injuries, and conservative treatment is considered to facilitate early mobilisation and optimise functional outcomes.
Dr. Elchin Orujov, Department of Traumatology and Orthopaedics, Azerbaijan Medical University, Baku, Azerbaijan. E-mail: doktorelcin86@mail.ru
Abstract
Introduction: Bilateral clavicle fractures are rare injuries, particularly when both fractures are non-displaced, accounting for less than 0.5% of all clavicle fractures. These injuries are typically associated with high-energy trauma, such as road traffic accidents or falls from height. Diagnosis may be challenging, as plain radiographs can miss subtle or non-displaced fractures, necessitating advanced imaging, such as computed tomography (CT) for accurate detection.
Case Report: We report the case of a 21-year-old male who sustained bilateral non-displaced midshaft clavicle fractures following a high-speed road traffic accident. Initial radiographs were inconclusive despite persistent clinical suspicion. CT imaging subsequently confirmed bilateral fractures involving the middle third of the clavicles. The patient was managed conservatively with bilateral arm slings, analgesia, and activity restriction. At 12-week follow-up, radiographs demonstrated satisfactory fracture union with callus formation. The patient achieved full, pain-free range of motion, including forward flexion (0–180°), abduction (0–180°), and external rotation (0–90°), without complications. This case highlights an important diagnostic pitfall and underscores the role of CT imaging in patients with suspected clavicle fractures and negative radiographs. It also reinforces the effectiveness of conservative management in non-displaced bilateral clavicle fractures, which can result in excellent functional outcomes.
Conclusion: Non-displaced bilateral midshaft clavicle fractures are exceptionally rare injuries that may be easily overlooked, particularly in the setting of high-energy trauma, where initial radiographs can be inconclusive. This case highlights a critical diagnostic pitfall, emphasising that persistent clinical suspicion should prompt advanced imaging, such as CT, to ensure accurate and timely diagnosis.
Categories: Radiology, Trauma, Orthopedics, hand surgery, fracture, clavicle radiology
Keywords: Bilateral clavicle fracture, computed tomography, midshaft clavicle fracture, non-displaced fracture, trauma.
Clavicle fractures are among the most common orthopaedic injuries, accounting for approximately 2.6–5% of all fractures and up to 35–45% of injuries involving the shoulder girdle [1,2]. The majority occur in the middle third of the clavicle (69–82%), due to its biomechanical vulnerability and lack of strong ligamentous support [3,4]. Bilateral clavicle fractures are rare, representing <0.5% of all clavicle fractures, and are usually associated with high-energy trauma, such as road traffic accidents, falls from height, or direct bilateral shoulder impact [2,5]. Non-displaced bilateral fractures are even more uncommon and may be easily overlooked, particularly in the acute trauma setting. Management of clavicle fractures depends on fracture displacement, shortening, comminution, and associated injuries. While displaced fractures may require surgical fixation, non-displaced fractures are generally treated conservatively with immobilisation, analgesia, and early rehabilitation [3,6,7,8]. Conservative management is considered the gold standard in non-displaced fractures due to the clavicle’s rich vascular supply, high union rates, preservation of alignment, and avoidance of surgical risks [4,9,10,11,12]. Despite the widespread use of plain radiography as the initial imaging modality, up to 5–10% of clavicle fractures may be missed, particularly when fractures are non-displaced or obscured by overlapping anatomical structures [8,9]. In such cases, computed tomography (CT) plays a crucial role in confirming the diagnosis and guiding management [9,12]. This report presents a rare case successfully managed with conservative treatment, highlighting important diagnostic and therapeutic considerations. To our knowledge, reports of bilateral non-displaced midshaft clavicle fractures with initially inconclusive radiographs confirmed on CT are exceedingly rare, particularly in the context of associated head injury managed conservatively and even more so from this geographic region. This report presents a rare case of bilateral non-displaced midshaft clavicle fractures following high-energy trauma, successfully managed with conservative treatment, highlighting the importance of thorough clinical evaluation and appropriate imaging.
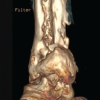
A 21-year-old male presented to the emergency department following a high-speed road traffic accident involving a frontal collision. The patient experienced a brief loss of consciousness at the scene. On admission, he was haemodynamically stable with normal vital parameters. His Glasgow Coma Scale score was 13/15. CT imaging of the head revealed a small subdural haematoma, which was managed conservatively. The patient was admitted to the intensive care unit for close neurological monitoring. During the secondary survey, the patient complained of bilateral shoulder pain, rated 7/10 on the visual analogue scale. Physical examination revealed localised tenderness over the midshaft of both clavicles with mild swelling. There was no visible deformity, skin tenting, or open injury. Active shoulder motion was limited due to pain. Neurovascular examination of both upper extremities was normal. Initial plain radiographs of the clavicles (Fig. 1) were inconclusive. Given persistent clinical suspicion, CT imaging with multiplanar and three-dimensional reconstruction was performed (Fig. 2, 3, 4), revealing non-displaced fractures of the middle third of both clavicles. The patient was managed conservatively with bilateral arm slings, oral analgesics (non-steroidal anti-inflammatory drugs), and restriction of upper limb activity. Immobilisation was maintained for pain control, followed by gradual mobilisation with supervised physiotherapy. Serial follow-up radiographs were obtained to monitor healing. At 12 weeks (Fig. 5), imaging demonstrated satisfactory fracture union with callus formation. Functional assessment showed a full, pain-free range of motion of both shoulders, including forward flexion (0–180°), abduction (0–180°), and external rotation (0–90°). The patient successfully returned to normal daily activities without limitations or complications.
Bilateral clavicle fractures are rare clinical entities, typically resulting from high-energy trauma, such as road traffic accidents or falls [2,3]. Their rarity and often subtle presentation make diagnosis challenging, particularly when fractures are non-displaced. The middle third of the clavicle is the most commonly affected region due to its biomechanical vulnerability and stress concentration [3,7]. In bilateral injuries, symmetrical force transmission may lead to similar fracture patterns on both sides, as observed in this case. A key clinical insight from this case is the limitation of plain radiography. Previous studies have demonstrated that up to 5–10% of clavicle fractures may be missed on initial radiographs, particularly when fractures are non-displaced or obscured by overlapping anatomical structures [6,9]. Missed diagnoses may result in persistent pain, delayed management, and potential functional impairment. In such scenarios, CT provides superior sensitivity and enables accurate visualisation of fracture morphology, particularly with multiplanar and three-dimensional reconstruction [9]. It should therefore be considered when clinical suspicion persists despite inconclusive radiographs. In the acute trauma setting, differential diagnoses for bilateral shoulder pain include acromioclavicular joint injury, sternoclavicular dislocation, scapular fracture, rib fractures, and soft tissue injuries. These are summarised in Table 1. Careful clinical assessment combined with appropriate imaging is essential to avoid misdiagnosis. Conservative management remains the gold standard for non-displaced clavicle fractures due to the clavicle’s rich vascular supply, which promotes reliable healing [4,8,10,11,12]. Reported union rates range from 90 to 100% in non-displaced fractures, with excellent functional outcomes and low complication rates [10,13,14]. Recent literature continues to support the evolving role of imaging and individualised management in clavicle fractures. A 2025 systematic review evaluating temporal trends in midshaft clavicle fracture management highlighted that although surgical fixation provides faster recovery and lower non-union rates in displaced fractures, long-term functional outcomes frequently converge with conservative management, emphasising the importance of appropriate patient selection [12,13,14,15]. Similarly, a 2026 systematic review of randomised controlled trials reported union rates of approximately 82–94% with conservative treatment compared to 93–100% with surgical intervention but noted that differences in long-term functional outcomes remain minimal [14,15]. These findings reinforce the present consensus that non-operative management remains appropriate for non-displaced fractures, where anatomical alignment is preserved, and the biological healing potential is high. Long-term outcome studies further support this approach. A 2023 follow-up study evaluating patients treated conservatively for midshaft clavicle fractures demonstrated generally favourable long-term functional outcomes, with most patients achieving satisfactory shoulder function years after injury [14]. In contrast, surgical intervention is typically reserved for specific indications, such as significant displacement, shortening greater than 2 cm, open fractures, neurovascular compromise, or symptomatic non-union [7]. While operative fixation may offer advantages, such as faster early recovery and reduced risk of non-union in displaced fractures, it is also associated with complications, including hardware irritation, infection, and reoperation [15]. A 2023 systematic review further emphasised that the timing and necessity of surgery remain debated, with outcomes influenced by fracture characteristics and patient-specific factors. Bilateral clavicle fractures may present additional functional challenges due to temporary impairment of both upper limbs, affecting activities of daily living. Despite this, available evidence suggests that non-displaced bilateral fractures can be successfully managed conservatively, with outcomes comparable to unilateral injuries when appropriately selected [3]. The present case is particularly noteworthy due to the combination of bilateral involvement, absence of displacement, and initial radiographic inconclusiveness. This highlights an important diagnostic pitfall: Reliance solely on plain radiography may lead to missed injuries. Clinicians should therefore maintain a high index of suspicion in trauma patients presenting with bilateral shoulder pain and pursue advanced imaging when clinical findings and radiographs are discordant [6,9]. Overall, this case reinforces present evidence that conservative management of non-displaced midshaft clavicle fractures yields excellent functional and radiological outcomes while avoiding surgical risks. It also underscores the critical role of CT imaging in detecting subtle fractures and guiding appropriate management.
Non-displaced bilateral midshaft clavicle fractures are exceptionally rare injuries that may be easily overlooked, particularly in the setting of high-energy trauma, where initial radiographs can be inconclusive. This case highlights a critical diagnostic pitfall, emphasising that persistent clinical suspicion should prompt advanced imaging, such as CT, to ensure accurate and timely diagnosis.
Conservative management remains the treatment of choice in non-displaced fractures, offering high union rates, excellent functional recovery, and avoidance of surgical risks. Despite the potential functional limitations associated with bilateral involvement, appropriately selected patients can achieve complete and pain-free restoration of shoulder function. Overall, this case underscores the importance of integrating thorough clinical evaluation with appropriate imaging strategies and reinforces that non-operative management can yield excellent outcomes even in rare and diagnostically challenging presentations.
Bilateral non-displaced clavicle fractures are exceptionally rare and can be overlooked on initial radiographs following high-energy trauma. Careful clinical evaluation and advanced imaging are essential to prevent missed diagnoses. Persistent clinical suspicion should prompt CT imaging to ensure accurate diagnosis, while conservative management can result in excellent functional and radiological outcomes.
References
- 1. Nordqvist A, Petersson C. The incidence of fractures of the clavicle. Clin Orthop Relat Res 1994;300:127-32. [Google Scholar] [PubMed]
- 2. Robinson CM. Fractures of the clavicle in the adult. Epidemiology and classification. J Bone Joint Surg Br 1998;80:476-84. [Google Scholar] [PubMed]
- 3. Stanley D, Norris. Recovery following fractures of the clavicle treated conservatively. Injury 1988;19:162-4. [Google Scholar] [PubMed]
- 4. Throckmorton T, Kuhn. Fractures of the medial end of the clavicle. J Shoulder Elbow Surg 2007;16:49-54. [Google Scholar] [PubMed]
- 5. Alao D, Guly Missed clavicular fracture: inadequate radiograph or occult fracture? Emerg Med J 2005;22:232-3. [Google Scholar] [PubMed]
- 6. Hill JM, McGuire MH, Crosby. Closed treatment of displaced middle-third fractures of the clavicle gives poor results. J Bone Joint Surg Br 1997;79:537-9. [Google Scholar] [PubMed]
- 7. Canadian Orthopaedic Trauma Society. Nonoperative treatment compared with plate fixation of displaced midshaft clavicular fractures. A multicentre, randomised clinical trial. J Bone Joint Surg Am 2007;89:1-10. [Google Scholar] [PubMed]
- 8. Ganesh MT, Pandian H, Palasseril Outcome of clavicle fractures treated by various modalities. J Orthop Case Rep 2025;15:250-6. [Google Scholar] [PubMed]
- 9. Sayed M, Sutar S, Kamel F, Faleel A, Dwyer AJ. Temporal trends in the management of midshaft clavicle fractures: A systematic review. Cureus 2025;17:e96532. [Google Scholar] [PubMed]
- 10. Yue L, Huang C, Zhang J, Wang Z, Wang S, Sun H. Classification of distal clavicle fractures and indications for conservative Orthop Res Rev 2025;17:221-7. [Google Scholar] [PubMed]
- 11. Cho CH, Kim BS, Kim DH, Choi CH, Dan J, Lee H. Distal clavicle fractures: A new classification. Orthop Traumatol Surg Res 2018;104:1231-5. [Google Scholar] [PubMed]
- 12. Toogood P, Horst P, Samagh S, Feeley BT. Clavicle fractures: A review of the literature and update on treatment. Phys Sportsmed 2011;39:142-50. [Google Scholar] [PubMed]
- 13. Riiser MO, Molund M. Long-term functional outcomes and complications in operative versus nonoperative treatment for displaced midshaft clavicle fractures in adolescents: A retrospective comparative study. J Pediatr Orthop 2021;41:279-83. [Google Scholar] [PubMed]
- 14. Virtanen KJ, Malmivaara AO, Remes VM, Paavola MP. Operative and nonoperative treatment of clavicle fractures in adults. Acta Orthop 2012;83:65-73. [Google Scholar] [PubMed]
- 15. Kang LX, Faulkner HJ, Howard WH, Low AK. Displaced medial clavicle fractures: A systematic review of outcomes after nonoperative and operative management. JSES Int 2022;7:79-85. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Management of Chronic Osteomyelitis Bone Defect Titanium Cage Combined with the Masquelet Technique: A Case Report
July 1, 2026 Management of Chronic Osteomyelitis Bone Defect Titanium Cage Combined with the Masquelet Technique: A Case Report May 1, 2026 The Computed Tomography-based Morphometry of Thoracolumbar Junction (T11–L2) in Western Indian Population: Implications for Transpedicular Screw Fixation
May 1, 2026 The Computed Tomography-based Morphometry of Thoracolumbar Junction (T11–L2) in Western Indian Population: Implications for Transpedicular Screw Fixation April 1, 2026 Intraoperative Assessment of Combined Anteversion Using the Ranawat Technique with a Smartphone Application: A Prospective Computed Tomography-based Agreement Study in Uncemented Total Hip Arthroplasty
April 1, 2026 Intraoperative Assessment of Combined Anteversion Using the Ranawat Technique with a Smartphone Application: A Prospective Computed Tomography-based Agreement Study in Uncemented Total Hip Arthroplasty February 1, 2026 Medial Clavicle Fracture with Posterior Dislocation of the Ipsilateral Acromioclavicular Joint Following Skiing Trauma
February 1, 2026 Medial Clavicle Fracture with Posterior Dislocation of the Ipsilateral Acromioclavicular Joint Following Skiing Trauma