
The application of Joshi’s External Stabilizing System (JESS) facilitates controlled, three-dimensional correction of rigid neglected clubfoot through differential distraction histogenesis, providing a superior alternative to aggressive open surgery in older children.
Dr. V S Subramaniyan, Devadoss Multispeciality Hospital, Madurai, Tamil Nadu, India. E-mail:vss5950@gmail.com
Abstract
Introduction: Neglected congenital talipes equinovarus (CTEV) presents a formidable challenge in paediatric orthopaedics, characterised by rigid soft-tissue contractures and adaptive bony changes that occur when the deformity remains untreated past the walking age. While neonatal clubfoot is successfully managed via the Ponseti method, delayed presentations require interventions that can address fixed skeletal remodelling without the morbidity of extensive posteromedial releases. This report analyses a single case of a child with neglected CTEV treated with the Joshi’s external stabilising system (JESS), following the patient from the pre-operative state through a 3-year follow-up period.
Case Report: A 3.5-year-old female presented with an uncorrected, unilateral, neglected idiopathic clubfoot. The clinical examination revealed a rigid, non-reducible deformity with a Pirani score of 6.0 and a Dimeglio score of 18 (Grade IV). Severe equinus, varus, cavus, and forefoot adduction were present, complicated by a large lateral-border callosity. Treatment involved the surgical application of the JESS fixator using a three-stage frame assembly. A protocol of fractional differential distraction was initiated postoperatively, distracting the medial side at twice the rate of the lateral side (1 mm/day vs. 0.5 mm/day) over 6 weeks, followed by a 6-week static stabilisation phase.
Conclusion: By the 3-year follow-up, the patient achieved a painless, plantigrade, and functional foot with significantly improved radiological indices. The talocalcaneal angles in both anteroposterior and lateral views normalised, and the patient demonstrated excellent range of motion compared to historical outcomes of open soft-tissue procedures. This case underscores JESS as a versatile, minimally invasive, and effective modality for managing the complex biomechanical demands of neglected clubfoot in low-resource and delayed-presentation settings.
Keywords: Clubfoot, neglected congenital talipes equinovarus, Joshi’s external stabilizing system fixator, ligamentotaxis, distraction histogenesis, pediatric orthopedic surgery.
Congenital talipes equinovarus (CTEV) is among the most frequent congenital musculoskeletal deformities, with a global incidence of 1–2/1,000 live births [1]. In high-income countries, the diagnosis is usually prenatal or neonatal, and the Ponseti method of serial casting and percutaneous Achilles tenotomy achieves successful correction in over 90% of cases [1]. However, in many developing regions, socioeconomic factors, lack of specialised healthcare, and traditional beliefs lead to a significant number of “neglected” cases – children who present with untreated clubfoot at an age where they have already begun to walk [2]. The pathophysiology of neglected CTEV is distinct from its neonatal counterpart. As a child begins to bear weight on a deformed foot, the initial soft-tissue contractures are exacerbated by the forces of ambulation [3]. The soft tissues on the medial and posterior aspects – including the tibialis posterior, flexor digitorum longus, and flexor hallucis longus tendons, as well as the Achilles tendon and the plantar fascia – become thickened, fibrotic, and severely retracted [4]. Simultaneously, the bones of the tarsus, which are primarily cartilaginous at birth, begin to ossify in a malaligned position. The talar head and neck are diverted medially and plantarly; the navicular is displaced medially toward the medial malleolus, and the calcaneus is held in a position of fixed varus and equinus [3]. These adaptive changes result in a rigid, “bone-on-bone” deformity that is largely unresponsive to conservative manipulation and casting [4]. Historically, surgeons addressed these rigid deformities through extensive posteromedial soft-tissue releases (PMR). While PMR can achieve initial correction, the long-term outcomes in older children are often poor, characterised by significant scarring, stiff joints, weakened intrinsic musculature, and a high rate of recurrence [2]. The “surgical” foot often becomes a “stiff” foot, leading many surgeons to seek more physiological alternatives that utilise the body’s natural regenerative capacity [2]. The concept of ligamentotaxis and distraction histogenesis, pioneered by Professor Gavriil Ilizarov, provided a new paradigm for managing these cases. Ilizarov demonstrated that slow, controlled distraction of living tissue induces a state of active growth and regeneration – histogenesis – in skin, muscle, nerves, blood vessels, and bone [2]. While the Ilizarov ring fixator is a powerful tool for clubfoot correction, its complexity and the requirement for tensioned transfixing wires can be problematic in the smaller, osteopenic bones of a child’s foot [5]. In response to the need for a simpler, more affordable, and patient-friendly system, Dr B. B. Joshi developed the Joshi’s external stabilising system (JESS) in 1988 [2]. JESS is a versatile mini-external fixator that utilises K-wires and a series of rods and distractors to apply the principles of ligamentotaxis without the weight or complexity of circular frames [6]. JESS is particularly suited for the Indian context and other similar healthcare environments due to its cost-effectiveness and the relatively short learning curve required for orthopaedic surgeons [7]. The system allows for the simultaneous correction of all components of the clubfoot deformity – equinus, varus, cavus, and adduction – while preserving the joints and avoiding the extensive scarring associated with open surgery [8]. This case report details the treatment of a child with severe neglected CTEV using the JESS fixator, providing a deep dive into the surgical technique, the biomechanical rationale for differential distraction, and the long-term clinical and radiological outcomes over a 3-year period.
Patient presentation and clinical history:
The patient was a 3.5-year-old female from a rural background who presented at our orthopaedic hospital with a severely deformed right foot. According to the parents, the deformity had been present since birth, but due to financial constraints and a lack of local specialised services, no medical treatment had been sought. The child had been walking on the deformed foot for over 2.5 years. Pre-operative clinical photographs are shown in Fig. 1.

Figure 1: Pre-operative clinical photographs of the patient (age 3.5 years) showing the severely deformed right foot with fixed equinus, hindfoot varus, forefoot adduction, deep medial and posterior skin creases, and the lateral border callosity. (a) Posterior view showing heel varus and equinus. (b) Medial view showing cavus and deep medial crease. (c) Lateral view showing the lateral border callosity.
On initial observation, the child demonstrated a significant gait abnormality, bearing weight on the outer, dorsal aspect of the right foot. A large, hyperkeratotic callosity was visible over the lateral border, particularly over the base of the fifth metatarsal. The right foot was noticeably smaller than the left, and there was associated wasting of the right calf muscles.
Detailed clinical examination:
A systematic clinical examination was performed to assess the severity and rigidity of the deformity. The foot was in a position of fixed equinus, severe varus of the hindfoot, significant cavus in the midfoot, and marked adduction of the forefoot. There were deep skin creases on the medial and posterior aspects of the foot, which were rigid and did not stretch upon manual manipulation. To quantify the deformity, we utilised the Pirani and Dimeglio scoring systems, which are the gold standards for clubfoot assessment [9]. The combined Pirani and Dimeglio scoring is presented in Table 1.
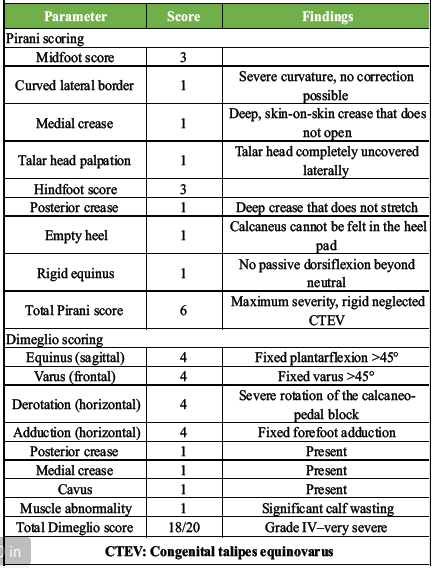
Table 1: Pre-operative Pirani and Dimeglio scoring of the affected foot
The Dimeglio score, which evaluates four parameters on a scale of 0–4 and adds points for “pejorative” factors, resulted in a score of 18 out of 20, placing the foot in Grade IV (Very Severe) [9].
Radiological evaluation:
Standard weight-bearing anteroposterior (AP) and lateral radiographs were obtained. In neglected CTEV, the usual bony landmarks are often distorted, but the relationships between the talus, calcaneus, and metatarsals remain critical for assessment [10].
- AP view: The talocalcaneal (TC) angle was measured at 11° (normal: 30°–55°). The Talo-1st Metatarsal angle was 40°, indicating severe forefoot adduction [10].
- Lateral view: The TC angle was 9° (normal: 25°–50°), and the tibiocalcaneal angle demonstrated fixed equinus at 60° [10].
- Foot bimalleolar axis (FBA): The FBA was measured at 62°, confirming severe internal talar spin (normal: 82.5°) [1].
Surgical intervention: JESS fixator application:
The patient was scheduled for surgical correction using JESS ligamentotaxis. The procedure was performed under general anaesthesia with the patient in the supine position. While a tourniquet was placed, it was kept uninflated to allow for the assessment of digital capillary refill throughout the wire placement process [10]. Intraoperative photographs of the JESS frame assembly are shown in Fig. 2.
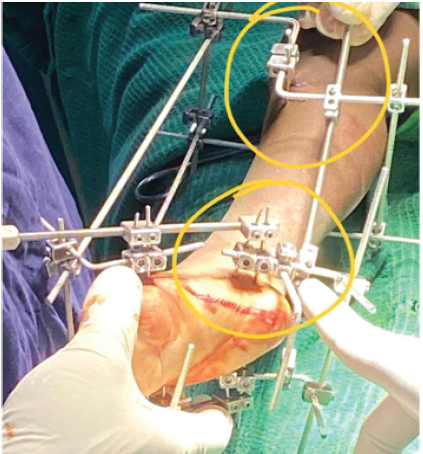
Figure 2: Intraoperative photographs demonstrating the three-stage Joshi’s external stabilizing system (JESS) frame assembly showing Kirschner wire placement in the tibial, calcaneal, and metatarsal zones, and the completed JESS construct with tibio-calcaneal and calcaneo-metatarsal distractors and the static tibio-metatarsal rod in situ.
The surgical technique was divided into three primary phases: wire installation, hold creation, and frame connection [11].
Kirschner wire installation:
The foundation of the JESS frame relies on precise K-wire placement in three key anatomical zones: the tibia, the calcaneus, and the metatarsals [11].
- Tibial zone: Two 2.0 mm transfixing K-wires were passed through the proximal tibial diaphysis, approximately 2 cm distal to the tibial tuberosity. The wires were passed from the lateral to the medial side, parallel to each other and to the knee joint line. In this 3.5-year-old child, a third wire was added 2 cm distal to the second wire to increase the axial stability of the tibial hold [11].
- Calcaneal zone: Two parallel 2.0 mm wires were passed through the posterior tuber of the calcaneus from the medial to the lateral side. Utmost care was taken to avoid the posterior tibial neurovascular bundle by palpating the pulse and entering the bone posterior to the vessel’s course [3]. An essential “axial” half-pin K-wire was then inserted from the posterior aspect of the heel, just distal to the Achilles tendon insertion, and directed anteriorly along the longitudinal axis of the calcaneus [11].
- Metatarsal zone: A 2.0 mm transfixing wire was passed through the necks of the first and fifth metatarsals. To ensure a stable hold on the forefoot, two additional wires were passed – one through the first and second metatarsals from the medial side and another through the fifth and fourth metatarsals from the lateral side – ensuring that all five metatarsals were integrated into the forefoot block [12].
Creation of holds:
The K-wires were then organised into three rigid “holds” using JESS components:
- Tibial hold: The tibial wires were attached to two Z-rods (one medial, one lateral). Before tightening the link joints, the wires were “pre-stressed” by bowing them slightly, which increases the stiffness of the assembly and prevents wire-to-bone migration [12].
- Calcaneal and metatarsal holds: These were created using L-rods and link joints, forming rigid blocks that could be independently manipulated during the distraction phase [11].
Connection and distraction assembly:
The final stage involved connecting the holds with distractors to address each component of the deformity:
- Calcaneo-metatarsal distractors: Two distractors were placed (one medial, one lateral) between the calcaneal and metatarsal holds to address midfoot cavus and forefoot adduction [13]
- Tibio-calcaneal distractors: Two distractors were placed posteriorly between the tibial Z-rods and the calcaneal L-rods to address the equinus [12]
- Static tibio-metatarsal rod: A static rod was connected between the tibial and metatarsal holds. This is a crucial biomechanical feature of JESS; it keeps the anterior portion of the ankle joint open, preventing the crushing of the talar dome and tibial plafond during the correction of equinus [11]
- Toe sling: A dynamic rubber sling was attached to the metatarsal wires to prevent flexion contractures (clawing) of the toes during distraction [12].
Post-operative protocol and distraction schedule:
The patient’s leg was elevated, and neurovascular checks were performed hourly for the first 24 h. Distraction was not started immediately; instead, a “latency period” of three days was observed to allow for the initial resolution of surgical oedema and the stabilisation of the pin-skin interface [10]. On the 3rd post-operative day, the “fractional differential distraction” protocol was initiated. The principle of differential distraction is to lengthen the medial side of the foot faster than the lateral side to correct the adduction and varus while simultaneously correcting the equinus [2]. The distraction schedule is outlined in Table 2.
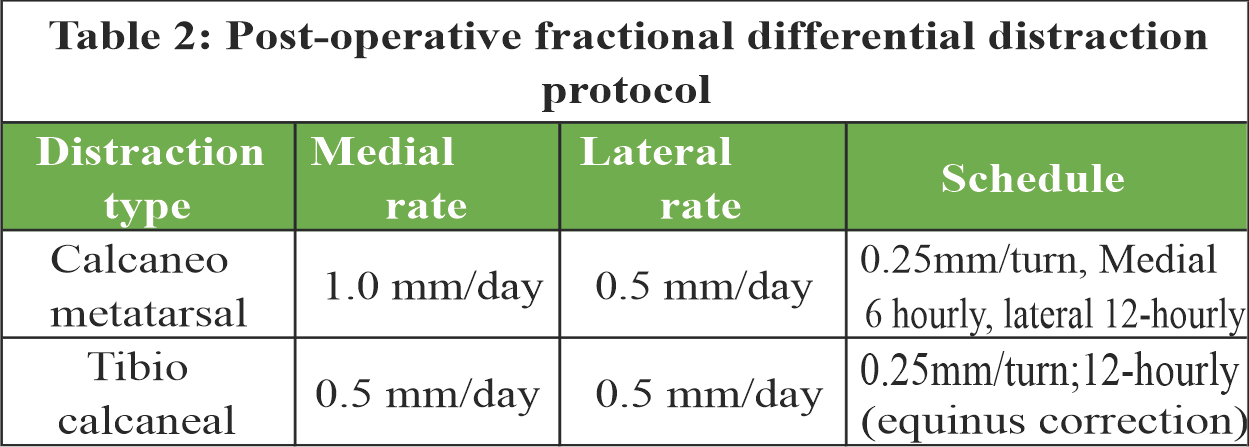
Table 2: Post-operative fractional differential distraction protocol.
The parents were trained to perform the turns using an Allen key. The distraction phase continued for 45 days. During this time, the foot was visually monitored for the gradual resolution of the medial crease and the improvement of the heel position. Weekly radiographs were obtained to ensure that no subluxation of the joints was occurring [13]. After full clinical correction was achieved (demonstrated by a plantigrade foot with 10° of dorsiflexion and 10° of abduction), the frame was locked in a “static phase” for an additional 6 weeks [13]. This phase is vital for the maturation of the regenerated tissues and the stabilisation of the tarsal bones in their new alignment [13].
Fixator removal and post-fixator care:
After 12 weeks, the JESS fixator was removed in a single stage under general anaesthesia. Following removal, a below-knee walking cast was applied in the corrected position for another 6 weeks. This cast protects the bones, which are often osteopenic after a period in an external fixator, and allows the pin tracts to heal fully [13]. Post-operative photographs are shown in Fig. 3.

Figure 3: Post-operative clinical photographs following fixator removal and cast application.
Once the cast was removed, the patient was transitioned into customised CTEV shoes with a lateral wedge and a night splint to maintain the correction. Physical therapy was initiated to improve the range of motion of the ankle and the strength of the calf muscles [11].
The management of neglected CTEV remains one of the most demanding tasks in paediatric orthopaedics. This case provides several insights into the advantages of JESS and the biological mechanisms of correction in older children.
Biomechanical advantages of JESS over Ilizarov:
The JESS fixator occupies a unique niche between conservative casting and complex ring fixation. While the Ilizarov method is highly effective, it has several drawbacks in the paediatric population, including its significant weight and the potential for tensioned wires to cut through soft, osteopenic bone [5]. JESS addresses these issues through its low-profile, lightweight design. The use of 2.0 mm untensioned K-wires provides enough stability to guide the foot into correction while being less invasive than the transfixing wires of the Ilizarov system [7]. The comparison of outcomes between the two systems suggests that JESS is particularly superior in children under 10 years of age, where the foot is smaller, and the bones are less dense [7].
The “tension-stress” effect and histogenesis:
The success of this case relies on the “tension-stress” effect described by Ilizarov, which states that living tissues, when subjected to slow, continuous tension, respond by increasing their biosynthetic activity [2]. In our patient, the rigid medial skin and fibrotic ligaments did not merely stretch; they underwent active growth. This is particularly evident in the resolution of the deep medial crease, which would have been impossible to correct with casting alone without risking skin necrosis or pressure sores [12]. Furthermore, JESS avoids the “crushing” of articular cartilage. In traditional casting or aggressive manipulation, the bones are often forced against each other, which can lead to avascular necrosis of the talus or flattening of the talar dome. The static tibio-metatarsal rod in the JESS assembly provides an “internal distractive force” that keeps the ankle joint distracted, allowing the talus to glide smoothly into the mortise as the equinus is corrected [11].
Analysis of clinical outcomes and scoring:
The transformation of the Pirani and Dimeglio scores in this case is a testament to the system’s efficacy. A drop in Pirani score from 6.0 to 0.5 over 12 weeks indicates that the correction was not only achieved but successfully maintained during the child’s growth [11]. The outcome data are summarised in Table 3.
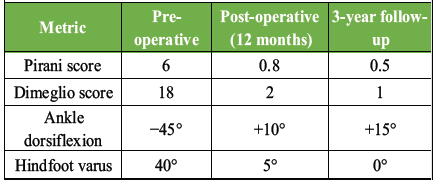
Table 3: Clinical and radiological outcome metrics at pre-operative, 12-month, and 3-year follow-up
The Dimeglio score’s improvement from Grade IV to Grade I is equally significant. Many studies on JESS have reported similar shifts. For example, a study of 20 feet by Shaik and Kumar showed that 80% of patients achieved excellent or good outcomes following the JESS protocol, with a significant reduction in the severity of the deformity [2].
Radiological parameters and the internal talar spin:
Radiological correction in neglected CTEV is often more difficult to achieve than clinical correction, as the bones have already adapted to the deformed position. However, JESS has been shown to improve the TC and talo-1st metatarsal angles significantly [10]. In our patient, the AP TC angle improved from 11° to 32°, and the lateral TC angle improved from 9° to 30° [14]. Perhaps more importantly, the FBA, which measures the internal talar spin, normalised from 62° to 82° [1]. Talar spin is a critical but often overlooked component of the clubfoot deformity; if the talus remains rotated within the ankle mortise, the risk of recurrence is high [1]. The differential distraction of JESS effectively derotates the calcaneo-pedal block around the talus, restoring the normal anatomical relationship between the leg and the foot [1].
Comparison with literature and meta-analysis of JESS outcomes:
Our results are consistent with a broad body of evidence supporting JESS for neglected CTEV. Several series have evaluated the long-term efficacy of this method, as summarised in Table 4.
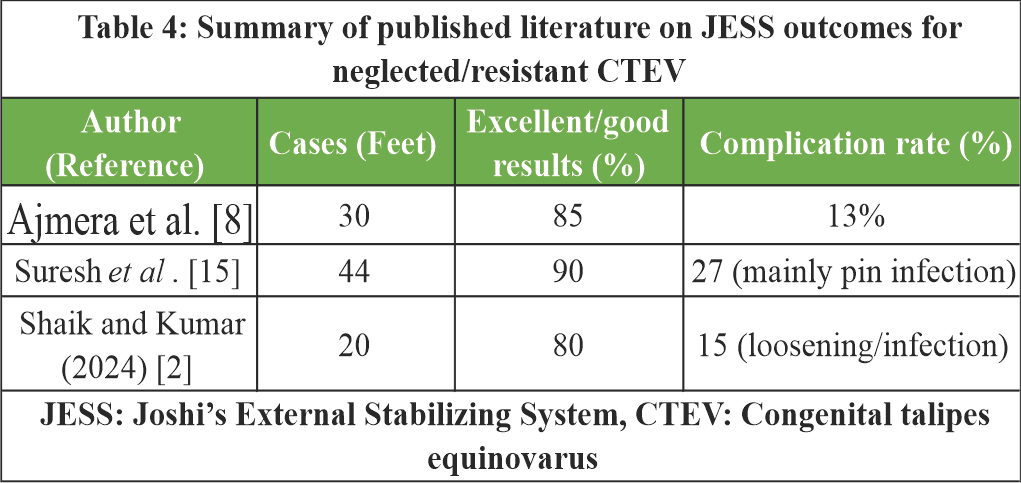
Table 4: Summary of published literature on JESS outcomes for neglected/resistant CTEV.
Suresh and Ahmed’s study highlighted that while the results are overwhelmingly good, the complication rate (approximately 30%) is a factor that surgeons must manage [15]. The most common complications are superficial pin tract infections, which occurred in our case as well. These are generally managed with local care and oral antibiotics and rarely lead to the failure of the procedure [15]. More serious complications like skin necrosis or epiphyseal separation are extremely rare with JESS compared to the Ilizarov system [15].
Management of complications and technical pearls:
The success of JESS in this case can be attributed to several technical “pearls” identified during the 12-week treatment period:
- Avoid over-distraction: If the digital capillary refill time exceeds 3 s, distraction must be paused for 24 h. In our case, a brief period of edema in the 2nd week was managed by pausing the distraction for 48 h [15]
- Pin tract care: Daily cleaning of the pin sites with saline and the application of a dry dressing are mandatory to prevent infection. Keeping the skin around the pins “tension-free” by making small skin incisions at the entry points significantly reduced the rate of infection [12]
- The toe sling: Flexion contractures of the toes are a common complication of distraction as the long flexors are stretched. The consistent use of the toe sling in this patient prevented “clawing”, which is often difficult to correct once established [15]
- The static phase: Many early failures of JESS were due to premature frame removal. Maintaining the frame for a minimum of 6 weeks after correction is achieved is essential for collagen stabilisation [13].
Long-term implications and growth:
At the 3-year follow-up, our patient showed no signs of recurrence. This is a crucial finding, as the high growth velocity during pre-adolescence can often trigger a relapse if the initial correction was incomplete or if muscle balance was not restored. The fact that the patient has a functional, plantigrade foot and can participate in normal childhood activities demonstrates that JESS-mediated correction is durable [1]. Three-year follow-up photographs are shown in Fig. 4.

Figure 4: Clinical photograph showing 3-year follow-up photographs demonstrating a durable, full weight-bearing on a plantigrade foot with resolved callosity and creases.
The management of neglected CTEV with the JESS represents a significant advancement over traditional, more aggressive surgical techniques. This case demonstrates that the rigid, unyielding deformities of a 3.5-year-old child can be corrected physiologically through the principle of distraction histogenesis. The JESS fixator provides several key advantages:
- Minimally invasive: It avoids the extensive scarring and joint stiffness associated with open posteromedial releases
- Controlled correction: The fractional differential distraction protocol allows the surgeon to tailor the correction to the specific biomechanical needs of the foot, addressing cavus, adduction, varus, and equinus simultaneously
- Joint preservation: By distracting the ankle and midtarsal joints during correction, the system protects the articular cartilage and promotes normal ossification of the tarsal bones
- Cost-effective and practical: Its simplicity and affordability make it an ideal choice for orthopedic departments in developing countries
- At the 3-year mark, our patient maintains a supple, plantigrade foot with normalised radiological indices and high functional scores. For the orthopaedic community, JESS remains a vital tool in the armamentarium against the disability caused by neglected clubfoot, offering a biological solution to a complex mechanical problem.
In children with rigid neglected CTEV, the JESS fixator facilitates a “biological” correction through differential distraction histogenesis. This modality effectively bypasses the limitations of casting and the morbidity of extensive open surgery, resulting in a durable, functional, and plantigrade foot. Success is contingent upon a rigid frame assembly, a disciplined distraction schedule, and a prolonged static stabilisation phase.
References
- 1. Singh A. Evaluation of neglected idiopathic CTEV managed by ligamentotaxis using JESS: A long-term follow-up. Adv Orthop 2011;2011:218489. [Google Scholar] [PubMed]
- 2. Shaik S, Kumar VK. The potential outcome of JESS in resistant and neglected CTEV cases. Int J Med Public Health 2024;14:757-61. [Google Scholar] [PubMed]
- 3. Meena R, Meena DS, Chauhan A. JESS and Ilizarov in neglected/relapsed CTEV: A prospective comparative study. IOSR J Dent Med Sci 2014;13:25-31. [Google Scholar] [PubMed]
- 4. Freedman JA, Watts H, Otsuka NY. The Ilizarov method for the treatment of resistant clubfoot: Is it an effective solution? J Pediatr Orthop 2006;26:432-7. [Google Scholar] [PubMed]
- 5. Ansari MO, Siddiqui YS, Harun F, Rana T, Hari K, Abbas M. Management of relapsed, residual, and resistant idiopathic congenital talipes equinovarus. J Orthop Case Rep 2026;16:413-20. [Google Scholar] [PubMed]
- 6. Gupta R, Kumar K, Jugran P. A prospective study of neglected and resistant clubfoot cases treated using Joshi’s external stabilisation system. Int J Res Orthop 2019;5:227-31. [Google Scholar] [PubMed]
- 7. Sinha S, Kumar A, Kumar S, Qureshi OA, Jameel J, Shyam A. The Joshi external stabilisation system (JESS): simple yet versatile. J Orthop Case Rep 2024;14:1-3. [Google Scholar] [PubMed]
- 8. Ajmera A, Jain S, Singh AK, Solanki M, Verma A. Simultaneous lateral column shortening along with differential distraction by Joshi’s external stabilisation system for rigid, neglected clubfoot correction. J Pediatr Orthop B 2019;28:579-85. [Google Scholar] [PubMed]
- 9. Emeka IH, Henry N, Lasebikan O, Emmanuel I, Oluchi IA, Malachy EC. Clinical evaluation of the pirani and dimeglio scoring systems and their correlation with the number of casting sessions using the ponseti method for idiopathic clubfoot treatment. EAS J Orthop Physiother 2025;7:63-9. [Google Scholar] [PubMed]
- 10. Muktevi S. Management of children with the Jess fixator. J Evol Med Dent Sci 2014;3:13920-5. [Google Scholar] [PubMed]
- 11. Joshi BB, Laud NS, Warrier S, Kanaji BG, Joshi AP, Dabake H. Treatment of CTEV by Joshi’s external stabilisation system (JESS). In: Kulkarni GS, editor. Textbook of Orthopaedics and Trauma. 1st New Delhi: Jaypee Brothers Medical Publishers; 1999. p. 459-64. [Google Scholar] [PubMed]
- 12. Narang AS, Singh H, Sharma V, Khare S. Comparison of short-term results of the JESS distractor and one-stage posteromedial release for neglected, resistant and relapsed or recurrent clubfoot. J Orthopaedics 2011;8(4):e8. [Google Scholar] [PubMed]
- 13. Sadana A, Pal CP, Dinkar KS. An assessment of the results of controlled fractional distraction by Joshi’s external stabilisation system in clubfoot. J Foot Ankle Surg (Asia Pacific) 2020;7:13-6. [Google Scholar] [PubMed]
- 14. Baghdadi S, Yadav P, Banskota B, Aroojis A, Talwar D, Spiegel DA. Outcome evaluation of treated clubfeets. J Foot Ankle Surg (Asia Pacific) 2020;7:87-92. [Google Scholar] [PubMed]
- 15. Suresh S, Ahmed A, Sharma VK. Role of Joshi’s external stabilisation system fixator in the management of idiopathic club foot. J Orthop Surg (Hong Kong) 2003;11:194-201. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Cadaveric Dissection of Adult Neglected Talipes Equinovarus
July 1, 2026 Cadaveric Dissection of Adult Neglected Talipes Equinovarus June 1, 2026 Clinical and Ultrasonographic Outcomes of Percutaneous Achilles Tenotomy Using an 18-Gauge Needle in Idiopathic Clubfoot: A Prospective Study
June 1, 2026 Clinical and Ultrasonographic Outcomes of Percutaneous Achilles Tenotomy Using an 18-Gauge Needle in Idiopathic Clubfoot: A Prospective Study March 1, 2026 Bilateral Clubfoot in Nail-Patella Syndrome: A Rare Syndromic Case Successfully Treated with the Ponseti Method
March 1, 2026 Bilateral Clubfoot in Nail-Patella Syndrome: A Rare Syndromic Case Successfully Treated with the Ponseti Method August 1, 2025 A Case Series of Functional and Radiological Outcome of Comminuted Distal Radius Fractures Treated with Bridging External Fixator with Optional Percutaneous K-wires
August 1, 2025 A Case Series of Functional and Radiological Outcome of Comminuted Distal Radius Fractures Treated with Bridging External Fixator with Optional Percutaneous K-wires