
The sequential Masquelet technique, followed by cylindrical titanium cage placement, effectively manages intra-articular tibial COM with 12 cm bone loss, enabling independent weight-bearing and ambulation within 6 months.
Mohammed Alshwieer, Department of Orthopedic Surgery, Security Forces Hospital, Riyadh, Saudi Arabia. E-mail: m.alshwieer@gmail.com
Abstract
Introduction: Managing large segmental bone defects secondary to chronic osteomyelitis is a major challenge in orthopaedic surgery, requiring both long-term and complex management. This study reports the outcome of effectively managing intra-articular tibial 12 cm bone loss secondary to chronic osteomyelitis (COM) with the sequential Masquelet technique followed by cylindrical titanium cage placement.
Case Report: A 37-year-old male with a distal tibia COM underwent a two-stage Masquelet technique with a titanium cage, autograft, and allograft for a 12 cm defect. Despite subsequent complications including plate breakage, varus deformity requiring revision, and plate removal due to skin complications, he achieved full pain-free weight-bearing within 1 year post-cage placement.
Discussion: This report describes the first documented case of managing COM with this specific combined technique. It demonstrates successful long-term functional recovery in complex distal tibia osteomyelitis, with sustained efficacy over a 2-year follow-up, validating this reconstructive approach despite avoidable post-operative complications.
Keywords: Orthopedic, trauma, osteomyelitis, bone infection, bone defect.
Long bone defects result from trauma, infection, non-union, or tumours, posing major challenges for patients and physicians [1]. Critical-sized defects (>5–6 cm) often lead to non-union, limb shortening, and functional loss, requiring reconstruction to restore limb function [1,2]. Available techniques include bone grafting, Ilizarov transport, vascularised fibula grafts, and the Masquelet procedure [2,3,4,5]. The cylindrical titanium mesh cages have emerged as a promising novel option for large traumatic defects [6,7,8,9,10]. This case report details the successful management of a patient presenting with chronic osteomyelitis (COM) and a large post-resection bone deficit, treated through a staged approach involving the Masquelet technique followed by the application of a mesh cage. Written informed consent was obtained from the patient for publication of this case report and any associated images.
A 34-year-old male, previously healthy with no significant past medical history, sustained multiple traumatic injuries from a 10-m fall. Initial injuries included multiple tendon ruptures in the left hand, a left scapular fracture, bilateral closed shoulder dislocations, an open fracture of the left talus, and an open fracture of the right distal tibia. At initial presentation following the fall, the patient underwent emergency management:
- Left ankle external fixation for talus open fracture
- Right distal tibia external fixation for open fracture
- Bilateral shoulder closed reduction for dislocations.
All acute injuries were managed appropriately according to standard trauma protocols. Timeline of the events listed in Table 1.
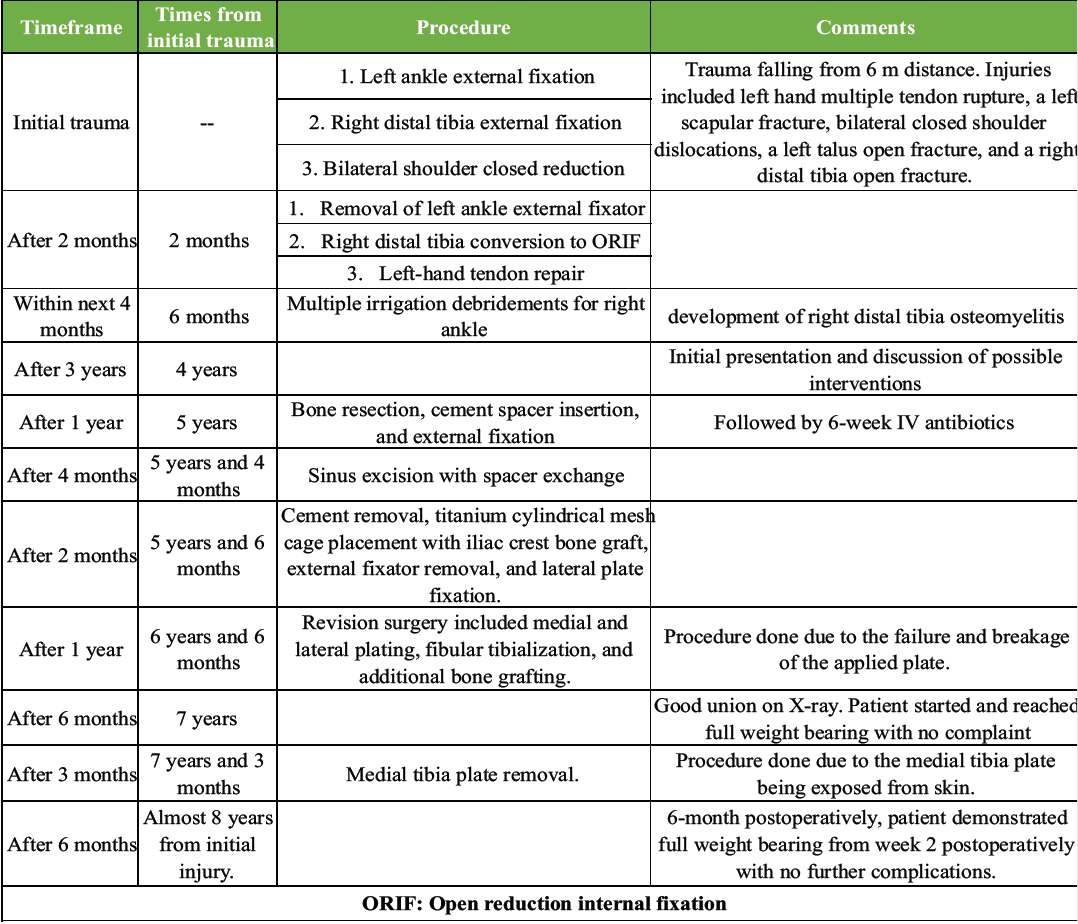
Table 1: Timeline from the start to the finish which includes all key interventions done to the patient
During early follow-up (2 months post-injury), the left talus open fracture demonstrated complete healing, allowing for: Removal of the left ankle external fixator and doing left-hand tendon repair. The right distal tibia open fracture was converted from external fixation to open reduction and internal fixation with a lateral tibia plate at 4 weeks post-injury. Several months later, despite achieving full weight-bearing, the patient was readmitted as COM of the left tibia. Despite 7 times of irrigation and debridement procedures with implant removal through an anteromedial approach, the infection persisted, leading to transfer to a specialised tertiary care centre.
Tertiary care presentation (4-year post-injury):
Approximately 4 years after the initial trauma, the patient presented to our hospital clinic bearing weight on both limbs with an antalgic gait and persistent sinus discharge from the right distal tibia. Initial radiographic and computed tomography evaluation (Fig. 1) revealed destructive changes and diffuse osteopenia in the distal tibia.
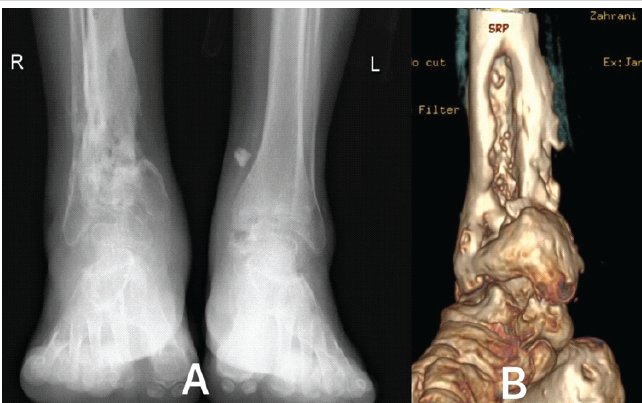
Figure 1: (a) This is X-ray anteroposterior view of the bilateral ankle of the patient. Detailing the signs of chronic osteomyelitis in the right distal tibia. (b) 3D computed tomography scan of the right distal tibia and ankle joint.
Notably, despite COM, the patient remained afebrile and fully weight-bearing on both limbs, though the right lower limb continued to drain purulent material. Laboratory investigations demonstrated normal white cell count and C-reactive protein levels. Surgical intervention options were discussed, including the Ilizarov technique, amputation, bone transport, and free tissue transfer. The patient initially refused all proposed interventions.
Definitive management: Masquelet technique (5-year post-injury):
One year later (5 years post-injury), the patient consented to surgical intervention. Following comprehensive preoperative investigation, he underwent right distal tibia bone resection through an anterolateral approach, cement spacer insertion, and external fixation application with a delta frame external fixator. Approximately 12 cm of bone loss resulted from the resection (Fig. 2).
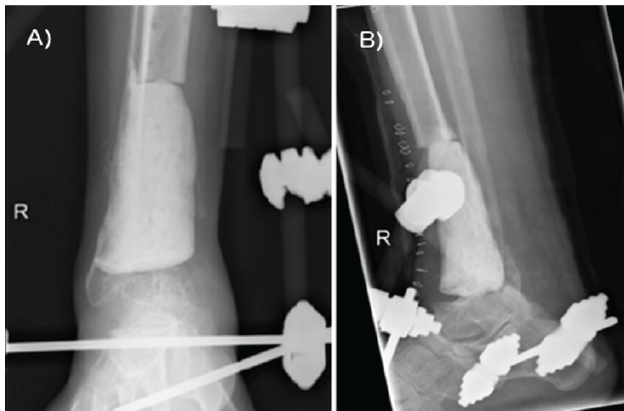
Figure 2: Right distal tibia anteroposterior and lateral views showing cement application with external fixation representing the first stage of Masqulete technique.
Intraoperative cultures grew Pseudomonas aeruginosa, necessitating a 6-week inpatient course of intravenous antibiotics. Spacer exchange was attempted at 4 months following the initial procedure. The patient was readmitted due to the development of an anteromedial sinus extending to the cement spacer, without active purulent discharge. He underwent second-stage irrigation and debridement, spacer exchange, and excision of the sinus. Six-month post-initial procedure (5.5-year post-injury), with no evidence of infection, the patient underwent third-stage reconstruction: Cement removal, titanium cylindrical mesh cage placement with iliac crest bone graft, external fixator removal, and lateral plate fixation. Intraoperatively, a well-developed membrane was observed. Fixation included a cage filled with allograft and autograft, a distal fibula plate used in the lateral tibia spanning the ankle to talus, and an anteroposterior ⅓ tubular plate securing the cage (Fig. 3). The decision to avoid a lateral tibia plate was due to poor skin condition overlying the tibia.
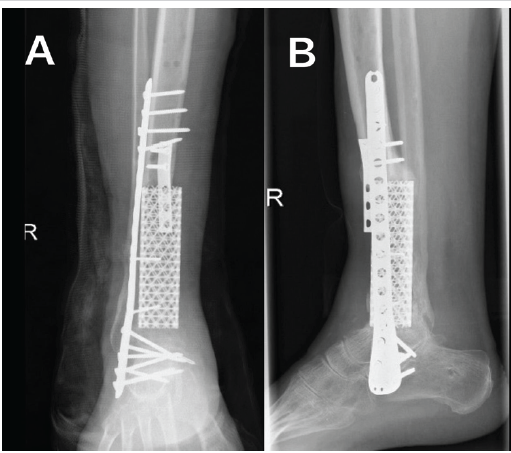
Figure 3: Right distal tibia anteroposterior and lateral views following second stage operation, showing titanium mesh cage fixed with 1/3 tubular plate.
Post-reconstruction complications and revisions:
At 1-year follow-up from the reconstruction, radiographs showed persistent non-union. Weight-bearing was initiated by the patient. Three weeks later, the patient presented with pain. Imaging revealed broken plate and varus deformity (Fig. 4).
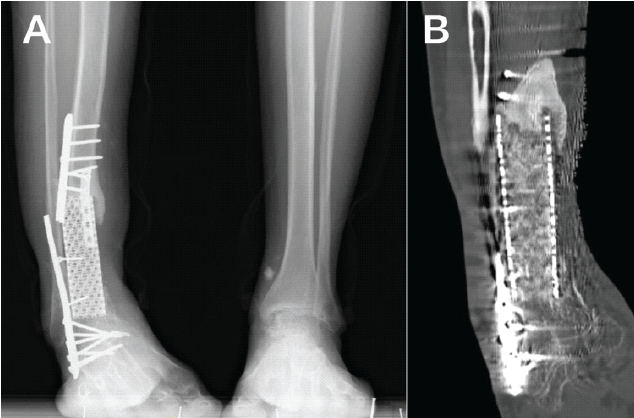
Figure 4: (a) Anteroposterior view of bilateral ankle showing right distal tibia going in varus deformity as a complication of fixation failure. (b) Computed tomography scan of the right distal tibia following plate failure showing plate full breakage.
Revision surgery included medial and lateral plating, fibular tibialisation, and additional bone grafting. Intraoperatively, cage distal fusion with ankle fusion was noted, and proximal loosening was identified. A proximal cage window was created, mixed cancellous grafts were impacted, and a fibular osteotomy was performed. The fibular graft was placed outside the cage and fixed laterally, while the medial and tibial surfaces were roughened to promote healing (Fig. 5).
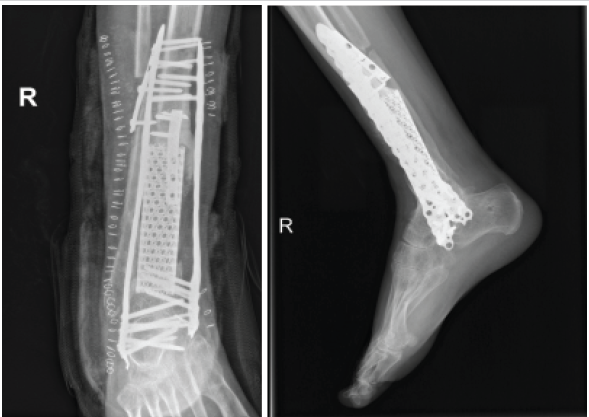
Figure 5: Right distal tibia anteroposterior view showing the addition of medial tibia plate with augmentation with fibula tibialization.
Six months of clinic follow-up showed minimal signs of union on radiographs. The patient was instructed to begin weight-bearing as tolerated. Two months later (8 months from the last revision), he achieved full weight-bearing on the right side and was ambulating freely with the aid of a cane. The second complication occurred 1 year later (7.25 years post-injury), and the case was complicated by an exposed medial plate, though the wound was clean with no signs of infection. The procedures done were irrigation and debridement, plate removal, and application of Magnifuse and bone morphogenetic protein (BMP) for bone healing augmentation. Intraoperative findings showed: After plate removal, the underlying bone was exposed, and the cage was circumferentially covered with bone proximally. Distally, the cage was exposed only on the posteromedial side (approximately 70° of the circumference). The bone was fully integrated into the cage and ankle, functioning as a single unit with the leg and ankle with excellent healing (Fig. 6). BMP, activated for 15 min, was then applied as a foam to the same region. Primary wound closure was performed. The final X-ray is shown in Fig. 6.
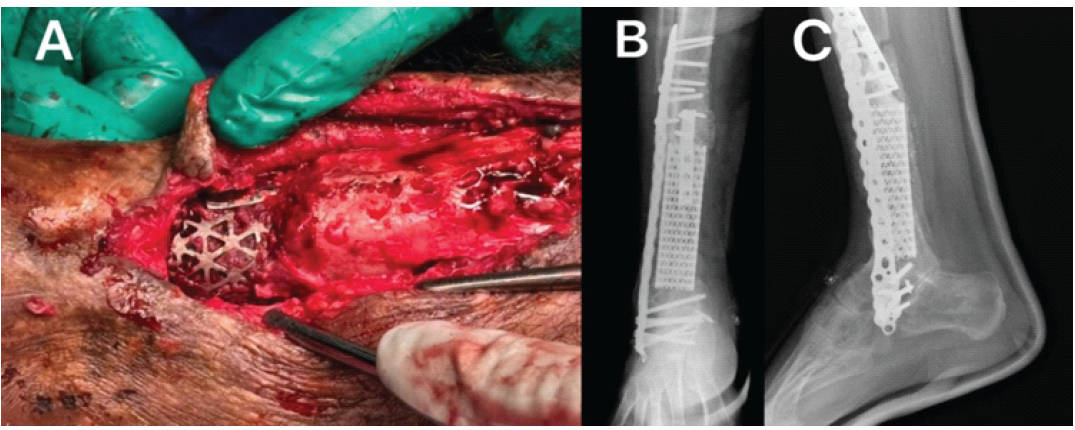
Figure 6: (a) Intraoperative image showing full integration of the cage proximally and distally acting as a single unit with the leg and foot. This figure shows complete coverage of the anterior surface of the tibia. (b and c) Final right distal tibial X-ray following medial tibia plate removal due to exposed plate. With a clinical picture of the affected limb, the patient is bearing full weight on it.
Final outcome (almost 8 years post-injury):
The immediate post-operative period was uneventful. The patient was instructed to start full weight-bearing at 2 weeks post-operatively after wound healing. By 6 weeks, the patient had progressed to full weight-bearing, entirely pain-free (Fig. 7). Leg length discrepancy was measured using a centogram and estimated to have the right side 2 cm shorter than the left side.
Long bone open fractures, particularly those with significant bone loss, pose substantial reconstructive challenges. The tibia is most commonly affected (68%), followed by the femur (22%) [11]. Defects exceeding 3 cm are especially problematic, often necessitating bone-length reconstruction and, in severe cases, amputation, as classified by Ferreira and Tanwar (types 2, 3, and 4) [1,2,12]. Titanium cylindrical cage mesh, typically filled with bone graft, originated in spinal surgery, receiving Food and Drug Administration approval in 1990 [6]. Its application historically expanded to maxillofacial surgery and acetabular reconstruction, becoming a well-established method in spine procedures with favourable outcomes [13,14]. Cobos et al. first documented the use of cylindrical titanium mesh for long bone segmental defects in 2000 [6]. Their initial report detailed two cases of extra-articular traumatic defects treated immediately with a graft-filled cage and intramedullary fixation, enabling early weight-bearing at 1-year follow-up. This pioneering work was supported by numerous subsequent case reports demonstrating similar positive results [7,15,16]. Further evidence of efficacy includes a 2004 case series on six traumatic bone defects, which showed reliable healing without autogenous cancellous bone grafting [17]. More recently, a 2018 study of 17 patients with segmental long bone diaphyseal defects reported favourable outcomes and radiological healing in 16 cases when treated with titanium mesh cages filled with cancellous bone grafts, combined with intramedullary nailing and plate osteosynthesis [8]. While previous investigations consistently reported favourable outcomes with single-stage cage stems and bone grafts in traumatic patients with substantial bone loss, none specifically addressed this method’s utility in COM [7,8,15,16,17]. Effective COM management requires thorough debridement and bone resection, irrespective of resulting defects [18], a gap this case addresses. Management of COM usually consists of bone resection and prolonged antibiotics. Hence, the application of the Masqulete technique emerged. Recent research highlights the effectiveness of the application of the Masquelet technique with titanium cylindrical mesh cages. Kaya et al. demonstrated superior outcomes in animals with combined procedures versus mesh cage alone [9]. Ma et al. reported satisfactory results in open fractures with significant bone loss (average 8.3 cm) using a two-stage Masquelet technique followed by titanium mesh implantation [19]. Chen et al. further supported combined approaches, successfully using 3D-printed titanium porous prostheses with the Masquelet technique for large osteomyelitis-induced femoral defects [10]. This case report details the successful management of intra-articular tibial COM with 12 cm of bone loss, using a sequential Masquelet technique followed by cylindrical titanium cage placement. The patient achieved independent weight-bearing and ambulation within 6 months post-cage placement, demonstrating a favourable functional outcome. Future advancements may include 3D-printed mesh cages for enhanced customisation [10,20]. However, our successful outcome with a standard cylindrical titanium mesh is promising due to its greater accessibility compared to specialised 3D-printed alternatives. In this case, an initial autograft and cancellous allograft within the cage failed due to plate failure. Subsequent revision involved augmenting the cage with a fibula strut bone, a viable option for large segmental defects, especially after previous iliac bone grafts or with multiple fractures [5,21].
Managing large segmental bone defects is a major challenge in orthopaedic surgery. A promising approach uses a spinal cage as a contained space for a bone graft. We applied this method to an iatrogenic defect caused by chronic osteomyelitis, augmenting it with the Masquelet technique to allow bacterial eradication before cage placement. This combined strategy resulted in a successful outcome, with the patient achieving full weight-bearing approximately six months after bone resection.
The sequential Masquelet technique, followed by cylindrical titanium cage placement, effectively manages intra-articular tibial COM with 12 cm bone loss, enabling independent weight-bearing and ambulation within 6 months.
References
- 1. Rosslenbroich SB, Oh CW, Kern T, Mukhopadhaya J, Raschke MJ, Kneser U, et al. Current management of diaphyseal long bone defects – a multidisciplinary and international perspective. J Clin Med 2023;12:6283. [Google Scholar] [PubMed]
- 2. Salcedo Cánovas C, Martínez Ros J, Ondoño Navarro A, Molina González J, Hernández Torres A, Moral Escudero E, et al. Infected bone defects in the lower limb. Management by means of a two-stage distraction osteogenesis protocol. Eur J Orthop Surg Traumatol 2021;31:1375-86. [Google Scholar] [PubMed]
- 3. Masquelet AC, Begue T. The concept of induced membrane for reconstruction of long bone defects. Orthop Clin North Am 2010;41:27-37. [Google Scholar] [PubMed]
- 4. Dheenadhayalan J, Devendra A, Velmurugesan P, Shanmukha Babu T, Ramesh P, Zackariya M, et al. Reconstruction of massive segmental distal femoral metaphyseal bone defects after open injury: A study of 20 patients managed with intercalary gamma-irradiated structural allografts and autologous cancellous grafts. J Bone Joint Surg Am 2022;104:172-80. [Google Scholar] [PubMed]
- 5. Jayaramaraju D, Venkataramani H, Rajasekaran RB, Agraharam D, Sabapathy SR, Rajasekaran S. Modified Capanna’s technique (vascularised free fibula combined with allograft) as a single-stage procedure in post-traumatic long-segment defects of the lower end of the femur: Outcome analysis of a series of 19 patients with an average gap of 14 cm. Indian J Plast Surg 2019;52:296-303. [Google Scholar] [PubMed]
- 6. Cobos JA, Lindsey RW, Gugala Z. The cylindrical titanium mesh cage for treatment of a long bone segmental defect: Description of a new technique and report of two cases. J Orthop Trauma 2000;14:54-9. [Google Scholar] [PubMed]
- 7. Attias N, Lindsey RW. Case reports: management of large segmental tibial defects using a cylindrical mesh cage. Clin Orthop Relat Res 2006;450:259-66. [Google Scholar] [PubMed]
- 8. Attias N, Thabet AM, Prabhakar G, Dollahite JA, Gehlert RJ, DeCoster TA. Management of extra-articular segmental defects in long bones using a titanium mesh cage as an adjunct to other methods of fixation: A multicentre report of 17 cases. Bone Joint J 2018;100-B:646-51. [Google Scholar] [PubMed]
- 9. Kaya O, Mirioglu A, Ozkan C, Bicer OS, Deveci MA, Tekin M, et al. Reconstruction of critical-size segmental femoral diaphyseal defects of New Zealand rabbits by using a combined titanium mesh cage and induced membrane technique. Eur J Orthop Surg Traumatol 2023;33:629-37. [Google Scholar] [PubMed]
- 10. Chen Z, Xing Y, Li X, Liu B, Liu N, Huo Y, et al. A 3D-printed porous titanium prosthesis combined with the Masquelet technique for the management of a large femoral bone defect caused by osteomyelitis. BMC Musculoskelet Disord 2024;25:474. [Google Scholar] [PubMed]
- 11. Study to Prospectively Evaluate Reamed Intramedullary Nails in Patients with Tibial Fractures. Investigators: Bhandari M, Guyatt G, Tornetta P 3rd, Schemitsch EH, Swiontkowski M, et al. Randomised trial of reamed and unreamed intramedullary nailing of tibial shaft fractures. J Bone Joint Surg Am 2008;90:2567-78. [Google Scholar] [PubMed]
- 12. Ferreira N, Tanwar YS. Systematic approach to the management of post-traumatic segmental diaphyseal long bone defects: Treatment algorithm and comprehensive classification system. Strategies Trauma Limb Reconstr 2020;15:106-16. [Google Scholar] [PubMed]
- 13. Grob D, Daehn S, Mannion AF. Titanium mesh cages (TMC) in spine surgery. Eur Spine J 2005;14:211-21. [Google Scholar] [PubMed]
- 14. Zhang ZX, Li T, Hao DJ. Single-stage treatment of osteomyelitis of the cervical spine using anterior instrumentation and titanium mesh cages. Spine (Phila., Pa. 1976) 2016;41:E949-54. [Google Scholar] [PubMed]
- 15. Ostermann PA, Haase N, Rübberdt A, Wich M, Ekkernkamp A. Management of a long segmental defect at the proximal meta-diaphyseal junction of the tibia using a cylindrical titanium mesh cage. J Orthop Trauma 2002;16:597-601. [Google Scholar] [PubMed]
- 16. Reynders P, Broos PL, Stoffelen D. The use of cylindrical titanium mesh cages in the treatment of post-traumatic segmental bone loss of the femur. Osteosynthesis Trauma Care 2003;11:99-104. [Google Scholar] [PubMed]
- 17. Lindsey RW, Gugala Z. Cylindrical titanium mesh cage for the reconstruction of long bone defects. Osteosynthesis Trauma Care 2004;12:108-15. [Google Scholar] [PubMed]
- 18. Panteli M, Giannoudis PV. Chronic osteomyelitis: What the surgeon needs to know. EFORT Open Rev 2016;1:128-35. [Google Scholar] [PubMed]
- 19. Ma XY, Yuan H, Cui D, Liu B, Han TY, Yu HL, et al. Management of segmental defects post open distal femur fracture using a titanium cage combined with the Masquelet technique A single-centre report of 23 cases. Injury 2023;54:111130. [Google Scholar] [PubMed]
- 20. Tetsworth K, Woloszyk A, Glatt V. 3D printed titanium cages combined with the Masquelet technique for the reconstruction of segmental femoral defects: Preliminary clinical results and molecular analysis of the biological activity of human-induced membranes. OTA Int 2019;2:e016. [Google Scholar] [PubMed]
- 21. Kim WY, Ji JH, Park SE, Kim YY, Jeong JJ, Kang HT. Surgical management of pilon fractures with large segmental bone defects using fibular strut allografts: A report of two cases. Eur J Orthop Surg Traumatol 2011;21:439-44. [Google Scholar] [PubMed]
Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2025 Spontaneous Clavicular Osteomyelitis Caused by Cutibacterium acnes Treated with Calcium Sulfate Beads
March 1, 2025 Spontaneous Clavicular Osteomyelitis Caused by Cutibacterium acnes Treated with Calcium Sulfate Beads July 1, 2026 Bilateral Non-Displaced Clavicle Fractures: A Very Rare Case Report
July 1, 2026 Bilateral Non-Displaced Clavicle Fractures: A Very Rare Case Report July 1, 2026 Continuous Local Antibiotic Perfusion for Refractory Musculoskeletal Infections: Functional and Patient-reported Outcomes in a 13-Case Series
July 1, 2026 Continuous Local Antibiotic Perfusion for Refractory Musculoskeletal Infections: Functional and Patient-reported Outcomes in a 13-Case Series June 1, 2026 Ceftazidime-Avibactam/Aztreonam Combination for the Treatment of Carbapenem-resistant Klebsiella pneumoniae-induced Osteomyelitis: A Case Series with Review of Literature
June 1, 2026 Ceftazidime-Avibactam/Aztreonam Combination for the Treatment of Carbapenem-resistant Klebsiella pneumoniae-induced Osteomyelitis: A Case Series with Review of Literature