
Most sports injuries appear to be sports-specific and knee injuries are common across many sports, especially football.
Dr. Chirag Sharma, Department of Orthopaedics and Trauma, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences, Shillong - 793018, Meghalaya, India. E-mail: chiragammu@gmail.com
Abstract
Introduction: Participation in sports has increased across North-East India, bringing important physical and psychological benefits. However, region-specific data on sports-related injuries remain limited, making it difficult to develop targeted prevention strategies.
Materials and Methods: This retrospective descriptive study analysed data from sportspersons presenting with sports-related injuries between January 2020 and December 2023. The aim was to describe the demographic characteristics, patterns, and modes of sports-related musculoskeletal injuries presenting to a regional tertiary-care teaching hospital. Information on age, sex, type of sport, anatomical site of injury, and mode of injury (contact vs. non-contact) was collected and analysed using descriptive statistics and chi-square tests.
Results: A total of 156 sportspersons were included, with a marked male predominance (134 males, 22 females; male-to-female ratio ≈ 6:1). Most injuries occurred in the 20–29-year age group (56.4%). Football was the most commonly associated sport (36.5%), followed by cricket and basketball. The knee was the most frequently injured anatomical site, particularly among football players. Contact sports accounted for 62% of all injuries. Significant associations were observed between the type of sport and anatomical site of injury, as well as between sport and mode of injury (P < 0.001).
Conclusion: Sports-related injuries in this region predominantly affect young adult males, with football-related knee injuries being the most common. The findings highlight the importance of sport-specific injury prevention strategies, particularly in contact sports such as football.
Keywords: Sports injury, football, knee injury, contact sports, musculoskeletal injury, injury prevention.
Participation in sports provides clear physical, psychological, and social health benefits, but it also comes with an inherent risk of injury. In everyday orthopaedic practice, sports-related musculoskeletal injuries form a significant proportion of cases and can lead to considerable morbidity, time away from sport, and financial burden for athletes, especially in competitive settings [1,2]. Accurate injury surveillance, therefore, plays an important role in developing effective prevention strategies [3]. The epidemiology of sports injuries varies widely depending on geographic region, type of sport, level of participation, and availability of training infrastructure [4,5]. Previous studies have also demonstrated differences in injury patterns between male and female athletes and across sporting disciplines [6,7]. Sports injuries are common among children and young athletes and may influence long-term participation in sports [8]. Adolescent athletes represent a vulnerable group with characteristic injury profiles that warrant focused attention [9]. While several studies from different parts of India have described patterns of sports-related injuries, data from North East India remain limited [2,3]. This region has a distinct sporting culture, with widespread participation in football alongside other activities such as basketball, badminton, cricket, and martial arts. Environmental factors, including prolonged monsoon seasons and variability in training conditions, may further influence injury patterns in this population. Understanding region-specific injury profiles is essential for identifying high-risk sports, commonly affected anatomical sites, and vulnerable demographic groups. Such information is crucial for developing targeted injury-prevention strategies, optimising resource allocation, and improving clinical management of injured athletes. The present study aims to describe the demographic characteristics, distribution, anatomical patterns, and modes of sports-related injuries presenting to a regional tertiary-care teaching hospital in North-East India over a 4-year period. In addition, the study evaluates the association between the type of sport, anatomical site of injury, and mode of injury to provide clinically relevant insights for prevention strategies.
Study design and setting:
This was a retrospective descriptive observational study conducted at a regional tertiary-care teaching hospital in North-East India. Institutional Ethics Committee approval was obtained before data collection, vide approval letter no. NEIGR/IEC/M5/F5/2024. The study was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice guidelines. Records from January 2020 to December 2023 were reviewed. Data were obtained from a dedicated sports injury and arthroscopy clinic functioning under the Department of Orthopaedics. All sportspersons presenting with injuries sustained during sporting activities were included. Injuries sustained during organised or recreational sporting activity, training or competition were included, involving all age groups. Injuries unrelated to sports activity and any incomplete or inadequate medical records in the register were excluded. Data were extracted from a standardised sports injury registry maintained at the sports injury clinic. Variables collected included age, sex, type of sport, anatomical site of injury, and mode of injury (contact or non-contact). Patients were further categorised into age groups (<10 years, 10–19 years, 20–29 years, 30–39 years, 40–49 years, 50–59 years, and ≥60 years). The primary outcomes were the distribution of injuries by sport, anatomical site, age group, sex, and mode of injury. Associations between categorical variables were also evaluated.
Statistical analysis:
Data were analysed using descriptive statistics. Categorical variables were summarised as frequencies and percentages. Associations between categorical variables were assessed using the chi-square test. A P < 0.05 was considered statistically significant. Statistical analysis was performed using Microsoft Excel and Python-based statistical tools.
Age and sex distribution:
A total of 156 sportspersons presenting with sports-related injuries were included in the study. Most injured sportspersons were aged 20–29 years (88 cases, 56.4%), followed by 10–19 years (28 cases, 17.9%) and 30–39 years (27 cases, 17.3%). Injuries were less frequent in older age groups, with only 13 cases (8.4%) occurring in individuals aged over 40 years (Table 1). A marked male predominance was observed across all age groups, with 134 males (85.9%) and 22 females (14.1%). Female athletes were predominantly represented in younger age groups, with no injuries recorded above 40 years. No statistically significant association was observed between age group and sex (χ2 = 3.38, P = 0.185).
| Table 1: Age and sex distribution of injured sportspersons | ||||
| Age group (years) | Male | Female | Total | Percentage |
| <10 | 0 | 0 | 0 | 0.00 |
| 10–19 | 22 | 6 | 28 | 17.90 |
| 20–29 | 75 | 13 | 88 | 56.40 |
| 30–39 | 24 | 3 | 27 | 17.30 |
| 40–49 | 7 | 0 | 7 | 4.50 |
| 50–59 | 4 | 0 | 4 | 2.60 |
| ≥60 | 2 | 0 | 2 | 1.30 |
| Total | 134 | 22 | 156 | 100 |
Sex distribution:
The study population showed a clear male predominance, with a male-to-female ratio of approximately 6:1 (Table 2). A Chi-square test, however, showed no statistically significant association between age group and sex (χ2 = 3.38, P = 0.185).
| Table 2: Sex distribution of study population | ||
| Sex | Frequency | Percentage |
| Male | 134 | 85.9 |
| Female | 22 | 14.1 |
Sport-specific injury distribution:
A total of 22 different types of sports (both contact and non-contact) were associated with injuries. Football was the most common sport (57 cases, 36.5%), followed by cricket (20 cases, 12.8%) and basketball (18 cases, 11.5%) to incur injuries (Fig. 1). Other sports included badminton (12 cases), running/trekking (12 cases), mixed martial arts (8 cases), and volleyball (6 cases), with the remaining sports contributing to a smaller proportion of injuries. Sex distribution varied significantly across different sports as depicted (Table 3 and Fig. 1), and this was statistically significant (χ2 = 61.87, P < 0.001).
| Table 3: Distribution of sports-specific injuries (Frequency+Male/Female) | ||||
| No. | Sports | Frequency | Male | Female |
| 1 | Football | 57 | 57 | 0 |
| 2 | Cricket | 20 | 20 | 0 |
| 3 | Basketball | 18 | 13 | 5 |
| 4 | Badminton | 12 | 10 | 2 |
| 5 | Running/Trekking | 12 | 5 | 7 |
| 6 | Mixed martial arts (Mma) | 8 | 5 | 3 |
| 7 | Volleyball | 6 | 4 | 2 |
| 8 | Weight lifting | 2 | 2 | 0 |
| 9 | Kabaddi | 2 | 2 | 0 |
| 10 | Hockey | 1 | 1 | 0 |
| 11 | Horse riding | 1 | 1 | 0 |
| 12 | Archery | 1 | 1 | 0 |
| 13 | Arm wrestling | 2 | 2 | 0 |
| 14 | Paragliding | 2 | 2 | 0 |
| 15 | High Jump | 3 | 3 | 0 |
| 16 | Golf | 1 | 1 | 0 |
| 17 | Table tennis | 1 | 1 | 0 |
| 18 | Tennis | 1 | 1 | 0 |
| 19 | Cycling | 1 | 1 | 0 |
| 20 | gymnastics | 2 | 0 | 2 |
| 21 | Kayaking | 1 | 0 | 1 |
| 22 | Boxing | 2 | 2 | 0 |
Mode of injury:
Contact sports accounted for most injuries (96 cases, 62%), while non-contact mechanisms accounted for 60 cases (38%), as tabulated (Table 4). A significant association was observed between the type of sport and mode of injury (χ2 = 156.0, P < 0.001).
| Table 4: Mode of injury of study population | ||
| Mode of injury | Frequency | Percentage |
| Contact | 96 | 62 |
| Non-contact | 60 | 38 |
Anatomical distribution of injuries:
The knee was the most frequently injured anatomical site (70 cases, 44%), followed by foot and ankle injuries (24 cases, 15%), lower back injuries (20 cases, 13%), and injuries involving the wrist and hand (15 cases, 10%). Shoulder injuries accounted for 12 cases (8%), while other anatomical sites contributed a smaller proportion of injuries (Table 5).
| Table 5: Distribution of injuries by anatomical site | ||
| Anatomic site of injury | Frequency | Percentage |
| Knee | 70 | 44 |
| Foot and ankle | 24 | 15 |
| Lower back ache | 20 | 13 |
| Shoulder | 12 | 8 |
| Elbow | 6 | 4 |
| Leg | 3 | 2 |
| Hand/wrist | 15 | 10 |
| Others | 6 | 4 |
Sport-specific anatomical distribution of injury patterns:
Distinct sport-specific injury patterns were observed. Football injuries predominantly involved the knee joint (41 cases), while running was associated mainly with knee and ankle injuries. Basketball injuries were more frequently seen in the wrist and hand (7 cases), whereas cricket showed a mixed pattern involving the shoulder (5 cases), wrist/hand (3 cases), and lower limb (Table 6). A highly significant association was observed between the type of sport and anatomical site of injury (χ² = 712.59, P < 0.001).
Association between injury site and mode of injury:
Mode of injury was categorized as contact or non-contact based on the nature of the sport and mechanism of injury, with sports involving physical player-to-player interaction classified as contact sports. We categorized injuries into contact and non-contact based on the nature of the sport, and used Chi-square to assess whether the distribution of anatomical injury sites differed between these two groups. Table 5 and Fig. 2 present the overall distribution of injuries by anatomical site, whereas Table 6 provides a detailed cross-tabulation of injury sites according to the type of sport, allowing identification of sport-specific injury patterns. A statistically significant association was found between anatomical site of injury and mode of injury (χ2 = 11.58, P = 0.021). However, no significant association was observed between sex and anatomical site of injury in our study (χ2 = 2.62, P = 0.623).
| Table 6: Distribution of anatomical site of injury according to sport | |||||||||
| Sport | Knee | Ankle | Thigh | Leg | Shoulder | Wrist/Hand | Arm | Back | Other |
| Archery | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Arm wrestling | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 |
| Badminton | 4 | 2 | 0 | 0 | 1 | 0 | 0 | 4 | 1 |
| Basketball | 4 | 5 | 0 | 0 | 0 | 7 | 0 | 2 | 0 |
| Boxing | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 0 | 0 |
| Cricket | 3 | 3 | 1 | 0 | 5 | 3 | 0 | 4 | 1 |
| Cycling | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Football | 41 | 6 | 0 | 2 | 0 | 3 | 0 | 5 | 0 |
| Golf | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Gymnastics | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| High Jump | 2 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 |
| Hockey | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Horse riding | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 |
| Kabaddi | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Kayaking | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Mma | 4 | 0 | 0 | 0 | 0 | 1 | 0 | 2 | 1 |
| Paragliding | 1 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 |
| Running | 6 | 6 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Table tennis | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Tennis | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 |
| Volleyball | 1 | 2 | 0 | 0 | 2 | 0 | 0 | 1 | 0 |
| Weight lifting | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 |
This study provides an overview of sports-related musculoskeletal injuries presenting to a tertiary care center in North-East India, a region where published data remain limited. The findings show that injuries are predominantly seen in young adult males, with football-related knee injuries forming the bulk of cases. A clear male predominance was observed in our cohort, with a male-to-female ratio of approximately 6:1. This likely reflects higher participation of males in competitive and contact sports in our setting, a trend that has been reported in previous studies [5,6]. However, it is important to recognize that generally injury patterns are more closely related to the type of sport and level of exposure rather than sex alone [7]. Most injuries occurred in the 20–29-year age group, which represents the most active and physically engaged segment of the population engaged in sports activities. Similar age distributions have been reported in earlier studies [9,10]. The conspicuous absence of females with sport injuries in older age groups in our study may be related to lower participation rates, as well as sociocultural factors that influence their long-term involvement in sports. Football was the most commonly associated sport, accounting for more than one-third of injuries. This differs from reports from other parts of India, where cricket is often the leading cause of sports-related injuries [3]. The predominance of football in our study likely reflects the sporting culture of North-East India, where football is widely played at both recreational and semi-professional levels [11]. In many cases, this participation occurs without structured training, adequate supervision, or protective measures, which may contribute to the higher injury burden [11]. The knee was the most frequently injured anatomical site, particularly among football players. This is consistent with existing literature, where the knee is recognised as a vulnerable joint due to its complex biomechanics and exposure to rotational and impact forces [3,9,10]. We also observed a clear sport-specific injury pattern. Football injuries were predominantly knee-related, basketball injuries were more commonly seen in the wrist and hand, and cricket showed a mixed pattern involving the shoulder and upper limb. These patterns are in keeping with the biomechanical demands of each sport and have been described in previous studies [11,12]. Contact mechanisms accounted for most injuries, and there was a significant association between the type of sport and mode of injury. Contact sports such as football, basketball, and mixed martial arts contributed disproportionately to the injury burden. In addition, the association between anatomical site and mode of injury suggests that the mechanism of injury may influence the pattern and location of injury [13]. Interestingly, we did not find a significant association between sex and anatomical site of injury. This suggests that injury patterns are largely determined by the sport itself rather than by sex. Similar observations have been reported in earlier studies [5,6]. The findings of this study have practical implications. Given the high burden of football-related knee injuries, there is a clear need for targeted injury-prevention strategies in this region. Introducing structured training programs, promoting awareness about injury prevention, and encouraging supervised play may help reduce the incidence of avoidable injuries [14]. From a clinical perspective, this highlights the importance of preventive strategies such as neuromuscular training, proprioceptive exercises, and structured warm-up programs like the FIFA 11+ protocol [15]. Overall, this study provides baseline epidemiological data from a previously underreported region, known for producing sports talents. While the findings are clinically relevant, further prospective studies incorporating injury severity, exposure data, and long-term outcomes would help build a more comprehensive understanding of sports injuries in this population.
Limitations:
This study has several limitations. First, its retrospective design restricts the ability to establish direct cause-and-effect relationships between risk factors and injury occurrence. It also relies on the accuracy and completeness of existing medical records, which can introduce potential information bias. Second, the study was carried out at a single tertiary-care center. This may limit how well the findings apply to the broader population, especially athletes who do not seek hospital-based care. Third, the study likely undercounts minor injuries and overcounts more severe cases since it included only patients who went to a specialized sports injury clinic. This introduces selection bias. Fourth, data on injury severity grading, detailed diagnostic categories (like ligamentous vs. muscular injuries), and functional outcomes were not available. This limits the ability to assess the clinical impact and prognosis of injuries. Fifth, the study did not record exposure data, such as the duration and intensity of sports participation. This prevents calculating injury incidence rates and limits comparisons with other epidemiological studies. Sixth, the relatively small number of female athletes made it difficult to conduct meaningful sex-specific analysis and limits conclusions about gender differences in injury patterns. Finally, potential confounding factors like training level, body mass index, use of protective equipment, playing surface, and previous injury history were not evaluated due to a lack of relevant data. These could influence injury risk and patterns. Despite these limitations, the study offers valuable baseline epidemiological data from an area that has been underreported. It also provides important insights for future research and targeted injury prevention strategies
In this study, sports-related injuries were seen predominantly in young adult males, with football emerging as the most common contributing sport. Knee injuries, particularly in football players, accounted for the majority of cases. We also found that injury patterns varied according to the type of sport, and contact sports were responsible for a larger share of injuries. These findings highlight the need for practical, sport-specific injury prevention strategies in this region. Simple measures such as structured training, supervised play, and basic injury-prevention programs could make a meaningful difference, especially in commonly played sports like football. Further prospective studies with more detailed data on injury severity and exposure would help in better understanding and preventing these injuries.
Clinical Message
In this single-center, retrospective study on sports injuries, we found that sports-related injuries were seen predominantly in young adult males; football emerging as the most common contributing sport. Knee injuries, particularly in football players, accounted for most injuries. While football injuries were predominantly knee-related, basketball injuries were more commonly seen in the wrist and hand, and cricket showed a mixed pattern involving the shoulder and upper limb. We also found that injury patterns varied according to the type of sport, and contact sports were responsible for a larger share of injuries. These findings highlight the need for injury surveillance and practical, sport-specific injury prevention strategies, especially in the high-risk group identified.
References
- 1. Palmer-Green D, Elliott N. Sports injury and illness epidemiology: Great britain olympic team (TeamGB) surveillance during the sochi 2014 winter olympic games. Br J Sports Med 2015;49:25-9. [Google Scholar] [PubMed]
- 2. Borgohain B, Tariang C, Darjee J, Marbaniang A, Komut O, Angom G, et al. A report on injuries and illnesses among athletes and games officials during XII South Asian Games-2016, Shillong, India. Int J Res Orthop 2017;3:1031-6. [Google Scholar] [PubMed]
- 3. John R, Dhillon MS, Syam K, Prabhakar S, Behera P, Singh H. Epidemiological profile of sports-related knee injuries in northern India: An observational study at a tertiary care centre. J Clin Orthop Trauma 2016;7:207-11. [Google Scholar] [PubMed]
- 4. Theisen D, Frisch A, Malisoux L, Urhausen A, Croisier JL, Seil R. Injury risk is different in team and individual youth sport. J Sci Med Sport 2013;16:200-4. [Google Scholar] [PubMed]
- 5. Hootman JM, Dick R, Agel J. Epidemiology of collegiate injuries for 15 sports: Summary and recommendations for injury prevention initiatives. J Athl Train 2007;42:311-9. [Google Scholar] [PubMed]
- 6. Edouard P, Feddermann-Demont N, Alonso JM, Branco P, Junge A. Injury risk is different between male and female athletes during 14 international athletics championships. Br J Sports Med 2017;51:315. [Google Scholar] [PubMed]
- 7. Powell JW, Barber-Foss KD. Sex-related injury patterns among selected high school sports. Am J Sports Med 2000;28:385-91. [Google Scholar] [PubMed]
- 8. Adirim TA, Cheng TL. Overview of injuries in the young athlete. Sports Med 2003;33:75-81. [Google Scholar] [PubMed]
- 9. Habelt S, Hasler CC, Steinbrück K, Majewski M. Sport injuries in adolescents. Orthop Rev (Pavia) 2011;3:e18. [Google Scholar] [PubMed]
- 10. Junge A, Lamprecht M, Stamm H, Hasler H, Bizzini M, Tschopp M, et al. Countrywide campaign to prevent soccer injuries in Swiss amateur players. Am J Sports Med 2011;39:57-63. [Google Scholar] [PubMed]
- 11. Wanivenhaus F, Fox AJ, Chaudhury S, Rodeo SA. Epidemiology of injuries and prevention strategies in competitive swimmers. Sports Health 2012;4:246-51. [Google Scholar] [PubMed]
- 12. Sheu Y, Chen LH, Hedegaard H. Sports- and recreation-related injury episodes in the United States, 2011-2014. Natl Health Stat Report 2016;99:1-12. [Google Scholar] [PubMed]
- 13. Koutedakis Y, Sharp NC. Seasonal variations of injury and overtraining in elite athletes. Clin J Sport Med 1998;8:18-21. [Google Scholar] [PubMed]
- 14. Feddermann-Demont N, Junge A, Edouard P, Branco P, Alonso JM. Injuries in 13 international athletics championships between 2007-2012. Br J Sports Med 2014;48:513-22. [Google Scholar] [PubMed]
- 15. Junge A, Rösch D, Peterson L, Graf-Baumann T, Dvorak J. Prevention of soccer injuries: A prospective intervention study in youth amateur players. Am J Sports Med 2002;30:652-9. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Proximal Rectus Femoris Avulsion Repair in a Collegiate Football Player: A Case Report
March 1, 2026 Proximal Rectus Femoris Avulsion Repair in a Collegiate Football Player: A Case Report October 1, 2025 Osteochondral Fragment from the Lateral Femoral Condyle in an Adult after Patellar Dislocation: A Surgical Challenge
October 1, 2025 Osteochondral Fragment from the Lateral Femoral Condyle in an Adult after Patellar Dislocation: A Surgical Challenge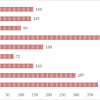 October 1, 2025 Musculoskeletal Occupational Injuries among Orthopedic Surgeons: Risk Factors and Insights from a Cross-Sectional Study
October 1, 2025 Musculoskeletal Occupational Injuries among Orthopedic Surgeons: Risk Factors and Insights from a Cross-Sectional Study June 10, 2024 From Trauma to Triumph: Navigating the Complexities of a Central Hip and Ipsilateral Knee Dislocation with Associated Fractures
June 10, 2024 From Trauma to Triumph: Navigating the Complexities of a Central Hip and Ipsilateral Knee Dislocation with Associated Fractures