
The CoreHip stem demonstrated favorable short-term outcomes. As it incorporates the strengths of previous stems, favorable long-term outcomes are anticipated.
Hiroki Kobayashi, Department of Orthopaedic Surgery, National Defence Medical College, Tokorozawa, Saitama, Japan. E-mail: supercova0205@gmail.com
Abstract
Introduction: The CoreHip Stem is a novel femoral stem introduced in 2021. It features a triple-taper design that enables three-dimensional load transmission and provides high rotational stability due to its rectangular cross-sectional geometry. This study aimed to retrospectively review the short-term clinical outcomes of primary total hip arthroplasty (THA) using the CoreHip stem.
Materials and Methods: A total of 41 primary THA cases (17 men and 24 women; mean age, 66 years; mean follow-up period, 18 months) performed through a supine anterolateral approach at our institution between July 2024 and August 2025 were enrolled in this study. The evaluated parameters included operative time, intraoperative blood loss, the Japanese Orthopaedic Association (JOA) hip scores, perioperative complications, postoperative stem alignment, subsidence, stress shielding, spot welds, cortical hypertrophy, and radiolucent lines. Statistical analyses were performed using the t-test.
Results: The mean operative time was 66.1 min, and the mean intraoperative blood loss was 202.2 mL. The mean JOA hip score improved from 44.9 points preoperatively to 95.2 points postoperatively. No perioperative complications were observed during the follow-up period. The stem survival rate was 100% at the final follow-up. No case showed obvious stem malalignment or subsidence of ≥2 mm. Grade I stress shielding was observed in five cases. Spot welds were identified in 30% of cases in Gruen zones 2 and 6 and in 27% of cases in zones 3 and 5. No other radiographic abnormalities were observed.
Discussion: Past studies have shown favourable short- to mid-term clinical outcomes in THA cases using short tapered-wedge stems. The results of the present study were consistent with previous reports. Although the CoreHip Stem was originally designed to promote proximal bone ingrowth, distal spot welds were often observed in our cases. This finding may reflect strong distal fixation and reactive bone formation induced by the cancellous bone bed. In our experience, the CoreHip Stem is relatively easy to handle and has a wide range of clinical applications. Further long-term investigations are warranted to confirm our findings.
Conclusion: The THA cases using the CoreHip Stem showed favourable short-term clinical outcomes.
Keywords: CoreHip stem, total hip arthroplasty, clinical outcomes.
The CoreHip Stem (Aesculap AG, Tuttlingen, Germany) is a relatively new femoral stem for total hip arthroplasty (THA) that was introduced in 2021 (Fig. 1).
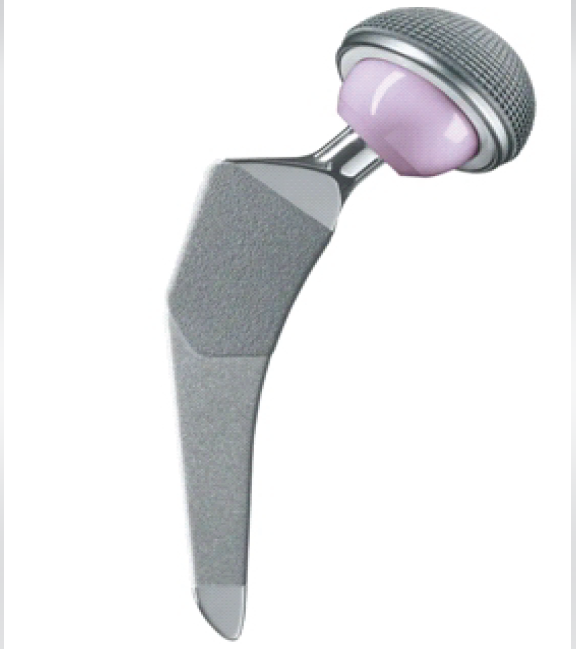
Figure 1: CoreHip stem.
It is a short tapered-wedge femoral stem with a triple-taper design. The proximal portion is coated with PlasmaPore to promote bone ingrowth, whereas the distal portion is sandblasted to facilitate bone ongrowth. In addition, the distal part has a tapered rectangular geometry, as seen in the Zweymüller-type design. This geometry is expected to provide strong rotational stability. Triple-taper stems incorporate tapering in the coronal and sagittal planes as well as from medial to lateral. The potential advantages of the triple-taper concept include strong initial fixation, prevention of stem subsidence, and avoidance of stress shielding through appropriate load transfer [1,2]. Favourable long-term outcomes have been reported for cementless stems with a similar triple-taper design. For example, the Polarstem demonstrated a 99% stem survival rate at 10 years [3]. In addition, the CoreHip Stem uses a compaction broaching system that enables uniform load distribution by forming a cancellous bone bed around the stem. This system has been reported to improve stem fixation and efficient load transfer [4,5]. Excellent survivorship has been documented for the Corail stem, which uses a similar system, with a 96% stem survival rate at 20 years [6]. Since the CoreHip stem incorporates concepts from previous stems associated with favourable clinical outcomes, it is expected to produce good long-term results. However, the clinical results using this stem are limited, mainly due to its relatively short production history. In this study, we retrospectively reviewed the short-term clinical outcomes of primary THA using the CoreHip Stem.
This study was conducted in accordance with the ethical standards of the Declaration of Helsinki and approved by the Ethics Committee of the National Defence Medical College, Japan (Approval No. 5353). All participants provided written informed consent before their inclusion in the study. A total of 41 primary THA cases performed via a supine anterolateral approach at our institution and affiliated hospitals between July 2024 and August 2025 were retrospectively analysed. This study was designed as a single-arm observational series to describe the short-term radiographic outcomes of a new THA implant. The sample size was determined based on the precision of estimation rather than on a formal hypothesis test. Assuming an expected incidence of a representative femoral bone reaction of approximately 30%, a sample size of around 40 hips would provide a 95% confidence interval with a precision of roughly ±15%, which we considered acceptable for this exploratory short-term observational study. Accordingly, the inclusion of approximately 40 consecutive hips was deemed appropriate, and 41 hips were finally analysed. The surgical procedure was performed as follows. A supine anterolateral approach was used, and all underlying muscles and tendons were preserved. Both the femoral and acetabular components were implanted using a press-fit, cementless technique. After trial reduction, leg length and offset were adjusted under fluoroscopic guidance. The final implants were inserted, and the wound was closed after confirming that no dislocation occurred in any position. The clinical parameters evaluated in this study included operative time, intraoperative blood loss, preoperative and postoperative Japanese Orthopaedic Association (JOA) hip score, complications (infection, fracture, dislocation, nerve palsy, and pulmonary embolism), and the need for revision surgery. Radiographic evaluation included assessment of stem alignment, stem subsidence, and periprosthetic bone reactions, including stress shielding, spot welds, cortical hypertrophy, and radiolucent lines. Stem alignment was measured on anteroposterior radiographs, and deviation of more than 3° from the neutral position was defined as varus or valgus alignment. Stress shielding was assessed according to the classification proposed by Engh et al. [7], whereas the presence of spot welds, cortical hypertrophy, and radiolucent lines was evaluated using the Gruen zone classification [8]. All results are presented as the mean ± standard deviation. Radiographic and clinical data were analysed on a per-hip basis. Continuous variables, including operative time, blood loss, and JOA hip scores, were summarised as means and standard deviations, whereas categorical variables, such as complications and each type of femoral bone reaction (stress shielding, spot welds, cortical hypertrophy, and radiolucent lines), were presented as counts and percentages. Because the primary aim of this study was descriptive, no formal hypothesis testing was planned. Missing data, if present, were not imputed and were reported as such, and all calculations were performed using Microsoft Excel (Microsoft Corp., Redmond, WA, USA).
The cohort consisted of 17 hips in men and 24 hips in women. The mean age at the time of surgery was 66 ± 9.5 years, the mean body mass index was 24.8 ± 5.1 kg/m2, and the mean follow-up period was 18 months. The underlying diagnoses were osteoarthritis in 31 hips, osteonecrosis of the femoral head in 5 hips, and rapidly destructive coxarthropathy in 5 hips. Femoral canal morphology was classified according to the Dorr classification as type A in 2 hips, type B in 36 hips, and type C in 3 hips (Table 1).
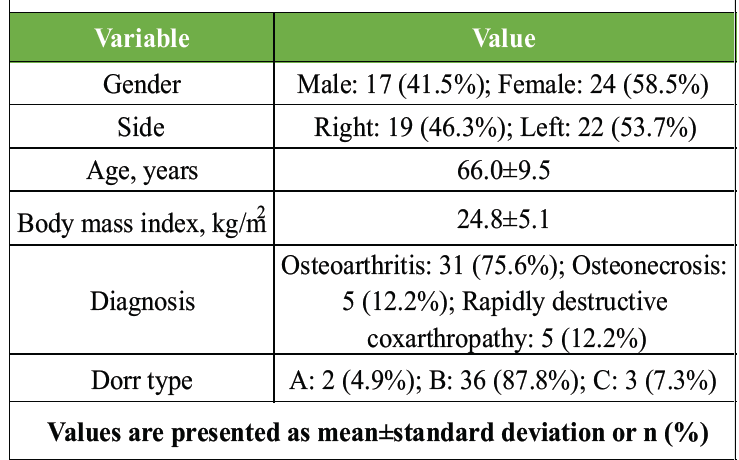
Table 1: Demographics of the patients
The mean operative time was 66.1 ± 22.4 min, and the mean intraoperative blood loss was 202.2 ± 144.6 mL. The mean JOA hip score improved from 44.9 ± 13.4 points preoperatively to 95.2 ± 5.2 points postoperatively. No post-operative complications were observed in any case. No patient required revision surgery during the follow-up period. Regarding the stem alignment, 14 stems were placed in a neutral position, 16 demonstrated varus alignment within 3°, and 11 demonstrated valgus alignment within 3°. No stem exhibited varus or valgus malalignment exceeding 3°. The mean stem subsidence was 0.2 ± 0.4 mm, and no cases showed subsidence of 2 mm or more. Stress shielding of Grade I was observed in five cases. Grade II or higher stress shielding was not found in any case. Spot welds were observed in zone 2 in 12 cases (29%), zone 3 in 11 cases (27%), zone 5 in 11 cases (27%), and zone 6 in 13 cases (32%), while no spot welds were observed in zones 1, 4, or 7. Neither cortical hypertrophy nor radiolucent lines were observed in any case.
Case presentation:
A 63-year-old man presented with bilateral hip pain and limited range of motion of both hips. Based on radiographic findings, he was diagnosed with bilateral osteonecrosis of the femoral head (Fig. 2). Due to severe pain, he had difficulty walking. Bilateral THA was performed using a supine anterolateral approach (Fig. 3).
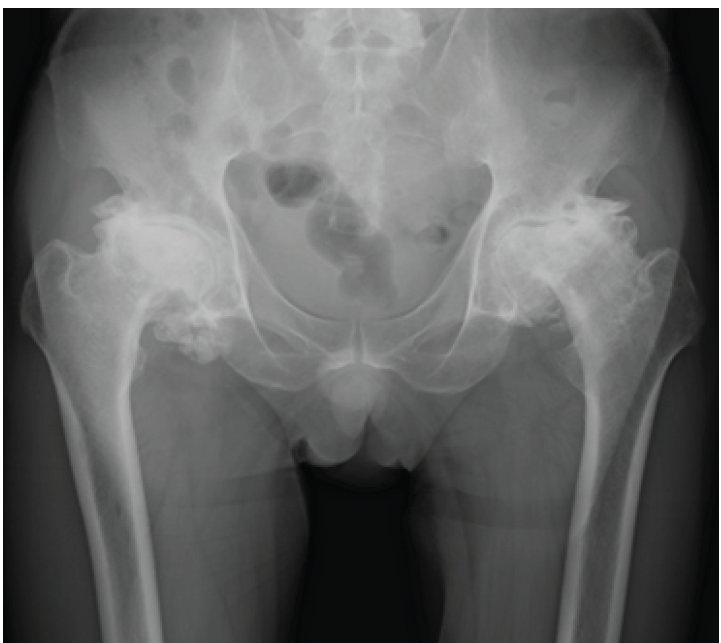
Figure 2: Preoperative radiographs. Collapse of the femoral heads due to bilateral osteonecrosis, along with surrounding osteophyte formation, is observed.

Figure 3: Postoperative radiographs. No intraoperative adverse events occurred, and no obvious abnormalities in stem alignment are observed.
The operative time was 120 min, and intraoperative blood loss was 200 mL. He demonstrated stable ambulation postoperatively and was discharged home 1 week after surgery. At the 2-year follow-up, he reported no pain and maintained a stable gait. The JOA hip score improved from 47 points preoperatively to 98 points at 2 years postoperatively. Radiographic evaluation revealed the presence of spot welds in zones 3 and 5. Stem subsidence was <2 mm. Cortical hypertrophy, stress shielding, or radiolucent lines were not identified (Fig. 4).
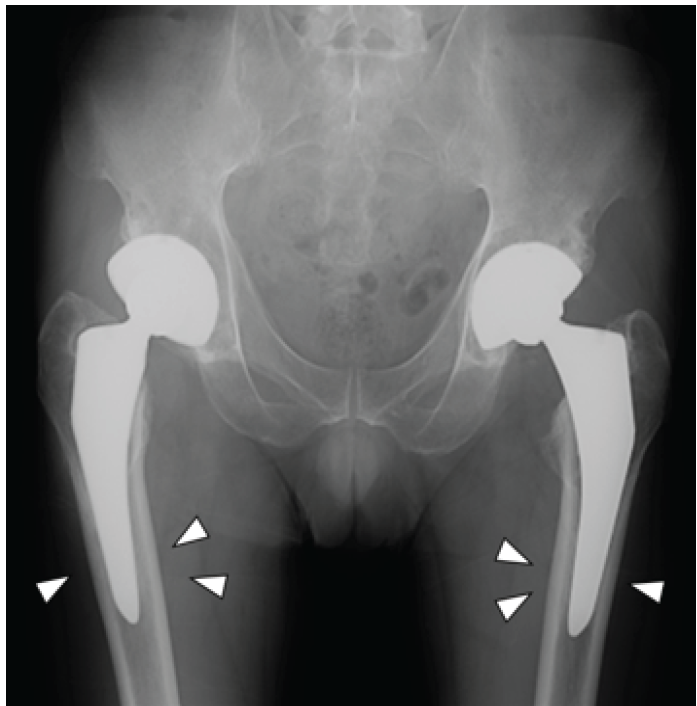
Figure 4: Final follow-up radiographs. Spot welds are observed in zones 3 and 5 (white arrowheads). No obvious stem subsidence is noted, and no cortical hypertrophy, stress shielding, or radiolucent lines are observed.
Short stems for THA have been actively developed due to their ease of handling in anterior minimally invasive approaches and their advantage in preserving bone stock [9]. Favourable outcomes have been reported for short stems such as the Taperloc Microplasty and Fitmore, demonstrating results comparable to those of standard stems [10,11,12]. In the present study as well, although the follow-up period was short, no particular clinical issues were observed, and satisfactory outcomes were achieved. In addition, previous reports on the CoreHip stem have indicated that the degree of stem subsidence is comparable to or less than that of other stems [13], and similarly in our study, subsidence was minimal. However, although short stems offer excellent operability due to their greater freedom within the femoral canal, several reports have noted a higher incidence of malalignment compared with standard stems [14]. Fortunately, no obvious malalignment was observed in this study, and this may be attributed to the design of this stem. On the anteroposterior view, the distal portion of the stem is slightly widened, which likely reduces varus–valgus error. Furthermore, the increased thickness in the anteroposterior direction may contribute to a shape that facilitates alignment with the femoral axis, despite being a short stem. Spot welds are commonly used as a radiographic indicator of stem stability. In our cases, spot welds were frequently found not only in zones 2 and 6, which correspond to the proximal plasma pore-coated region, but also in zones 3 and 5 in the distal region. This finding may reflect the unique structural characteristics of the stem. The triple-taper design of the stem provides strong rotational stability and enhances initial fixation [1,2]. Furthermore, the Plasma Pore coating in the proximal region promotes early bone ingrowth, while the sandblasted distal surface induces bone ongrowth through frictional effects. Consistent with the proposed mechanisms, there was no cortical hypertrophy indicative of stem instability or radiolucent lines attributable to micromotion in our cases, suggesting that strong initial fixation was achieved. These characteristics may overcome the poor outcomes associated with distal fixation in non-porous regions, a known limitation of prior tapered-wedge stems [15]. Therefore, this stem may have a wide range of applications, including cases where sufficient proximal initial fixation is difficult to obtain. On the other hand, while the stem excels at evenly distributing mechanical stress, this property can lead to reduced proximal load transfer and stress shielding over time [16]. In addition, the compaction broaching system used for this stem may be associated with an increased risk of intraoperative and early postoperative periprosthetic femoral fractures compared with conventional broaching [17]. Although we did not experience any implant-related fractures in our cases, the CoreHip system allows conversion to a cemented stem during the procedure in the event of such a complication. Based on the overall assessment of these findings, the most suitable candidates for this implant are patients in whom an anterior-based approach is preferred to preserve the surrounding muscles and tendons. Although there are no strict limitations regarding bone quality, the use of a cemented stem may be more appropriate in cases with extremely poor bone stock, as intraoperative conversion remains feasible. Whereas previous stems generally required surgeons to choose between proximal or distal fixation, this stem provides sufficient stability at either level and is less dependent on the patient’s femoral morphology. This characteristic represents a major advantage of the present stem design.
The short-term clinical and radiographic outcomes of the CoreHip Stem were favorable. However, longer-term follow-up studies are mandatory to confirm the long-term effectiveness of this stem.
The CoreHip stem demonstrated favorable short-term outcomes. As it incorporates the strengths of previous stems, favorable long-term outcomes are anticipated.
References
- 1. Hayashi S, Nishiyama T, Fujishiro T. Periprosthetic bone mineral density with a cementless triple tapered stem is dependent on daily activity. Int Orthop 2011;36:1137-42. [Google Scholar] [PubMed]
- 2. Wroblewski BM, Siney PD, Fleming PA. Triple taper polished cemented stem in total hip arthroplasty: Rationale for the design, surgical technique, and 7 years of clinical experience. J Arthroplasty 2001;16 8 Suppl 1:37-41. [Google Scholar] [PubMed]
- 3. Cypres A, Fiquet A, Girardin P, Fitch D, Bauchu P, Bonnard O, et al. Long-term outcomes of a dual-mobility cup and cementless triple-taper femoral stem combination in total hip replacement: A multicenter retrospective analysis. J Orthop Surg Res 2019;14:376. [Google Scholar] [PubMed]
- 4. Hjorth MH, Kold S, Søballe K, Langdahl BL, Nielsen PT, Christensen PH, et al. Preparation of the femoral bone cavity for cementless stems: Broaching vs compaction. A five-year randomized radiostereometric analysis and dual energy X-ray absorption study. J Arthroplasty 2017;32:1894-901. [Google Scholar] [PubMed]
- 5. Kold S, Rahbek O, Vestermark M, Overgaard S, Søballe K. Bone compaction enhances fixation of weightbearing titanium implants. Clin Orthop Relat Res 2005;431:38-44. [Google Scholar] [PubMed]
- 6. Vidalain JP. Twenty-year results of the cementless corail stem. Int Orthop 2011;35:189-94. [Google Scholar] [PubMed]
- 7. Engh CA, Bobyn JD, Glassmann AH. Porous-coated hip replacement. The factors governing bone ingrowth, stress shielding, and clinical results. J Bone Joint Surg Br 1987;69:45-55. [Google Scholar] [PubMed]
- 8. Gruen TA, McNeice GM, Amstutz HC. “Modes of failure” of cemented stem-type femoral components: A radiographic analysis of loosening. Clin Orthop Relat Res 1979;141:17-27. [Google Scholar] [PubMed]
- 9. Hayashi S, Hashimoto S, Matsumoto T, Takayama K, Niikura T, Kuroda R. Risk factors of thigh pain following total hip arthroplasty with short, tapered-wedge stem. Int Orthop 2020;44:2553-8. [Google Scholar] [PubMed]
- 10. Van Veghel MH, Hannink G, Oldenrijk J, Van Steenbergen LN, Schreurs BW. A comparison of uncemented short versus standard stem length in total hip arthroplasty: Results from the Dutch arthroplasty register. Acta Orthop 2023;94:330-5. [Google Scholar] [PubMed]
- 11. Saragaglia D, Orfeuvre B. Mid-term results of 119 Taperloc MicroplastyTM femoral stems after a mean 61 months (50-82) of follow-up. Orthop Traumatol Surg Res 2020;106:1501-6. [Google Scholar] [PubMed]
- 12. Schader JF, Thalmann C, Maier KS, Schiener T, Stoffel K, Frigg A. Prospective evaluation of clinical and radiographic 10-year results of Fitmore short-stem total hip arthroplasty. J Orthop Surg Res 2023;18:893. [Google Scholar] [PubMed]
- 13. Morgan M, Sungu M, Schuster P. Subsidence analysis of the metaphyseal fixed shorter cementless CoreHip stem. J Surg 2025;10:11437. [Google Scholar] [PubMed]
- 14. Ima M, Kabata T, Inoue D, Yanagi Y, Iyobe T, Demura S. Influence of stem length on sagittal alignment in total hip arthroplasty: A comparison between short and standard stems. BMC Musculoskelet Disord 2025;26:188. [Google Scholar] [PubMed]
- 15. Cooper HJ, Jacob AP, Rodriguez JA. Distal fixation of proximally coated tapered stems may predispose to a failure of osteointegration. J Arthroplasty 2011;26:78-83. [Google Scholar] [PubMed]
- 16. Maeda T, Nakano M, Nakamura Y, Momose T, Sobajima A, Takahashi J, et al. Relationship between stress shielding and optimal femoral canal contact regions for short, tapered-wedge stem analyzed by 2D and 3D systems in total hip arthroplasty. J Clin Med 2023;12:3138. [Google Scholar] [PubMed]
- 17. Hovik O, Aamodt A, Amlie E, Sivertsen EA. Increased risk of intraoperative and early postoperative periprosthetic femoral fracture with compaction compared with broaching in cementless THA: A single-center study of 6,788 hips. Acta Orthop 2024;95:492-7, [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures
July 1, 2026 The Development of Metabolic Bone Failure as the Principal Manifestation of Undiagnosed Primary Hyperparathyroidism: A Rare Instance of Bilateral Femoral Neck Fractures July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach
July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach
July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study
June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study