
Peroneus longus tendon autograft is a safe, reliable, and effective alternative graft option for anatomical ACL reconstruction, providing excellent functional outcomes with minimal donor-site morbidity.
Dr Gagan Khanna, Department of Orthopaedics, Sri Guru Ram Das Institute of Medical Sciences and Research, Sri Guru Ram Das University of Health Sciences, Sri Amritsar, Punjab, India. E-mail: neerajmittal9898@gmail.com
Abstract
Introduction: While hamstring and patellar tendon autografts are traditional choices for anterior cruciate ligament (ACL) reconstruction, concerns regarding donor-site morbidity and graft diameter persist. The peroneus longus tendon (PLT) has emerged as a promising alternative with excellent biomechanical properties and minimal knee-specific morbidity.
Objectives: To prospectively evaluate knee functional outcomes, clinical stability, and donor-site morbidity following arthroscopic ACL reconstruction using a full-thickness tripled PLT autograft in an Indian patient cohort.
Materials and Methods: A prospective interventional study was conducted on 30 patients (mean age 18–50 years) with ACL insufficiency. All underwent arthroscopic reconstruction using a triple PLT autograft. Clinical stability was assessed through Lachman and Pivot Shift tests. Functional outcomes were measured using the Lysholm Knee Score, while donor-site morbidity was evaluated using the American Orthopaedic Foot and Ankle Society (AOFAS) and Foot and Ankle Disability Index (FADI) scores over a 6-month follow-up period.
Results: The mean graft diameter was 8.7 ± 0.6 mm. The mean Lysholm score significantly improved from 54.6 ± 8.1 preoperatively to 91.3 ± 5.4 at 6 months (P < 0.001). Post-operative stability was restored in over 90% of cases. Ankle function remained stable, with mean AOFAS (98.0 ± 2.3) and FADI (99.0 ± 1.2) scores showing no significant decline from baseline. No graft failures or major ankle complications were recorded.
Conclusion: The full-thickness tripled PLT autograft is a safe, robust, and effective alternative for ACL reconstruction. It provides effective graft diameter and excellent functional recovery with negligible donor-site morbidity, making it particularly suitable for active young adults.
Keywords: Anterior cruciate ligament reconstruction, peroneus longus tendon, autograft, Lysholm score, donor-site morbidity.
Anterior cruciate ligament (ACL) injuries represent a significant burden in sports medicine, carrying profound implications for joint stability, functional capacity, and long-term musculoskeletal health [1]. Driven by a global surge in athletic participation and high-impact training, the incidence of ACL ruptures has risen steadily, particularly among adolescents and young adults [1,2]. In the Indian subcontinent, this trend is increasingly evident among urban youth; however, historical challenges in healthcare access and a reliance on conservative management have often led to underreporting and secondary degenerative sequelae [3,4]. The ACL functions as the primary restraint to anterior tibial translation and a critical regulator of rotational stability through its two distinct bundles: the anteromedial and posterolateral [5]. Beyond mechanical stabilisation, the ligament provides essential proprioceptive feedback [6]. Its intra-articular, extra-synovial nature results in a poor intrinsic healing capacity; consequently, untreated deficiency leads to recurrent instability, meniscal damage, and accelerated early-onset osteoarthritis [7]. The paradigm of ACL management has shifted from open repair to anatomical arthroscopic reconstruction [8]. While autografts remain the gold standard due to effective biological incorporation, traditional donor sites present inherent trade-offs: Bone–Patellar Tendon–Bone (BPTB): Risks anterior knee pain and kneeling discomfort [9]. Hamstring Tendons: Associated with variable graft diameters and potential flexor weakness [10]. Quadriceps Tendon: Limited by donor site pain and surgeon familiarity [11]. The peroneus longus tendon (PLT) has recently gained traction as a robust autograft candidate. Biomechanically, its tensile strength and stiffness are comparable and in some cases superior to native ACL and hamstring grafts [12]. Its harvest provides consistent diameter and length while sparing the primary knee flexors, potentially offering a more favourable profile for patients with high functional demands [13]. Despite these advantages, concerns regarding donor site morbidity, specifically ankle eversion strength and gait alterations, persist [14]. Furthermore, data regarding the efficacy of PLT autografts within the Indian population, characterised by unique anthropometric profiles and cultural requirements for squatting and barefoot ambulation, remains sparse [15]. Recent randomised trials, systematic reviews, and meta-analyses have established the PLT as a viable alternative autograft for ACL reconstruction [12,14,15]. However, prospective population-specific data from the Indian subcontinent remain limited, particularly regarding donor-site morbidity in patients with high functional demands such as squatting, barefoot ambulation, and cross-legged sitting. Furthermore, evidence evaluating full-thickness tripled PLT graft constructs with simultaneous assessment of knee stability and ankle functional preservation using standardised scoring systems remains sparse. Therefore, the present study was undertaken to evaluate clinical outcomes and donor-site morbidity following ACL reconstruction using a full-thickness PLT autograft in an Indian cohort. Therefore, the present study was undertaken to prospectively evaluate knee functional outcomes, clinical stability, and donor-site morbidity following arthroscopic ACL reconstruction using a full-thickness tripled PLT autograft in an Indian patient cohort. Knee function was assessed using the Lysholm Knee Score, while donor-site morbidity was evaluated using the American Orthopaedic Foot and Ankle Society (AOFAS) and Foot and Ankle Disability Index (FADI) scoring systems.
Study design and setting
This prospective interventional study was conducted at the Department of Orthopaedics, SGRDIMSAR, Sri Amritsar, Punjab, from July 2024 to December 2025. The study cohort comprised 30 patients undergoing arthroscopic ACL reconstruction. Randomization was not performed due to the prospective single-arm study design.
Selection criteria
Patients were selected based on the following rigorous criteria: Age 18–50 years with clinical instability and magnetic resonance imaging (MRI)-confirmed ACL insufficiency, isolated ACL tears or those associated with remedial/lateral meniscal injuries and pre-operative eversion power ≥4 on the Medical Research Council scale were included in the study. Whereas associated tibial/femoral fractures or bony avulsion injuries and a history of significant ipsilateral ankle injury or instability and concomitant multi-ligamentous knee injuries were excluded from the study.
Pre-operative protocol
A comprehensive clinical evaluation, neurovascular assessment, and MRI of the affected knee were performed for all participants. All patients provided written informed consent, and anaesthetic fitness was secured. Prophylactic intravenous antibiotics were administered 30 min before the induction of spinal or general anesthesia. Routine post-operative MRI assessment could not be performed due to financial and logistical constraints, unless deemed necessary in selected special cases.
Surgical technique
Diagnostic arthroscopy and portal placement
With the patient in a supine position and a thigh tourniquet applied, standard anterolateral and anteromedial portals were established. Initial diagnostic arthroscopy was performed to confirm the ACL tear and address any associated meniscal pathology.
PLT harvesting
The PLT was harvested from the ipsilateral limb through a 2 cm longitudinal incision located 2–3 cm proximal to the posterior margin of the lateral malleolus.
- Harvesting: After isolating the PLT, a closed tendon stripper was advanced proximally, terminating 4–5 cm distal to the fibular head to safeguard the common peroneal nerve.
- Donor site management: To preserve ankle stability, the distal stump of the PLT was tenodesed to the peroneus brevis.
- Graft preparation: The tendon was cleared of soft tissue and folded (tripled) to achieve the target diameter. Both ends were secured with whip-stitches using No. 5 Ethibond sutures.
Tunnel preparation and fixation
Femoral and tibial tunnels were created independently at their respective anatomical footprints. The autograft was pulled through the tunnels and secured using: Femoral side: Suspensory fixation (Endobutton system). Tibial side: Aperta/interference screw.
Post-operative evaluation and follow-up
Patients followed a standardized rehabilitation protocol and were evaluated at 6, 12, 18, and 24 weeks. The clinical outcomes and donor-site morbidity were quantified using assessment tool (Table 1).
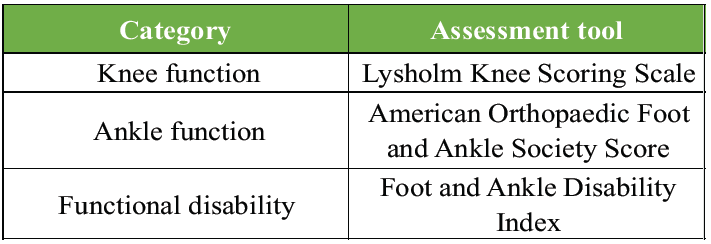 Table 1. Clinical Outcome Measures Used for Functional Assessment
Table 1. Clinical Outcome Measures Used for Functional Assessment
Statistical analysis
Data were analyzed using descriptive and inferential statistics. Quantitative variables were expressed as mean ± standard deviation, while qualitative data were expressed as frequencies and percentages to draw valid clinical conclusions.
A staggering 90% of patients belong to the age group of 18–35 years, representing the most physically active and economically productive segment of society. There is a distinct male predominance (86.6%), likely reflecting higher participation rates in contact sports and risk-prone occupational tasks within this specific region (Table 2). Sports-related trauma is the primary driver of injury (60%), followed by road traffic accidents (26.7%), underscoring the high-velocity nature of these ligamentous ruptures. Injury distribution across the right (56.7%) and left (43.3%) knees is relatively balanced. Interestingly, the cohort is split evenly (50/50) between acute and chronic presentations, indicating that half of the patients seek or receive surgical intervention after the 3-month mark. While 73.3% of cases were isolated ACL tears, over a quarter (26.7%) presented with concomitant meniscal injuries, highlighting the complexity of trauma often associated with the initial pivoting event (Table 2).
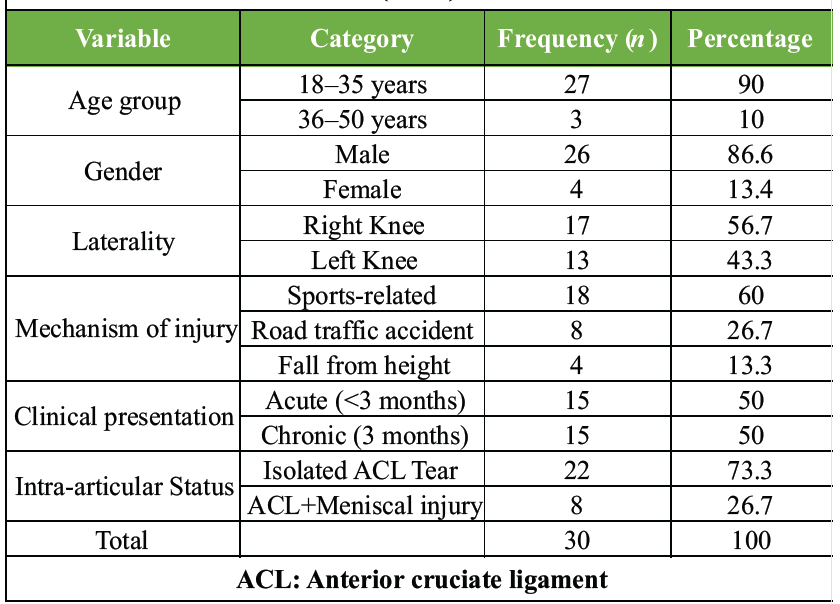
Table 2: Baseline demographic and injury profile of the study cohort (n=30)
Graft characteristics and surgical uniformity
All patients underwent reconstruction using a tripled peroneus longus autograft secured with a fixed-loop Endobutton (femoral) and an interference screw (tibial).
Mean graft length: 26.4 ± 2.1 cm (Range: 23–30 cm)
Mean graft diameter: 8.7 ± 0.6 mm (Range: 7.5–9 mm)
Functional outcomes and clinical stability
There was a highly significant improvement in knee function from the pre-operative state to the 6-month follow-up.
The longitudinal analysis of the Lysholm Knee Score demonstrates a remarkable and statistically significant recovery of joint function following reconstruction with the peroneus longus autograft (Table 3).
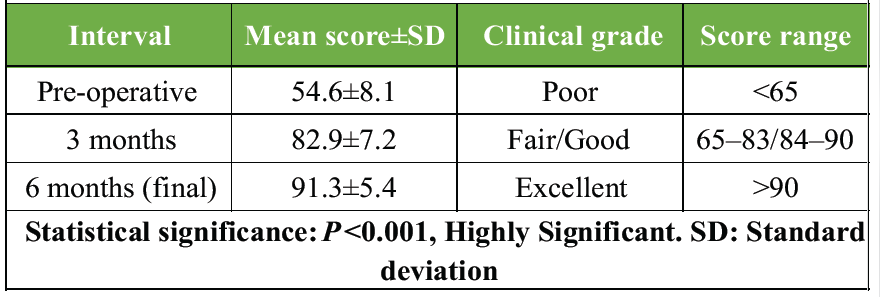
Table 3: Longitudinal comparison of lysholm knee scores
The mean score surged from a pre-operative 54.6 (Poor) to a final 91.3 (Excellent). This represents a 67% improvement in subjective knee function, stability, and weight-bearing capacity. Phase 1 (0–3 Months): Rapid initial recovery, with scores climbing by nearly 30 points as mechanical stability was restored and acute post-operative symptoms subsided. Phase 2 (3–6 Months): Refinement of function, where scores moved into the excellent range, reflecting successful graft incorporation and the effectiveness of the rehabilitation protocol. The P < 0.001 confirms that these improvements are not incidental.
- Restoration of sagittal stability: Preoperatively, 100% of the cohort exhibited high-grade (II/III) anterior laxity during the Lachman Test. Post-reconstruction, 86.7% (26/30 patients) returned to a completely normal clinical profile, demonstrating the graft’s exceptional ability to resist anterior tibial translation (Table 4).
- Superior rotational control: The pivot shift test, often considered the most clinically relevant indicator of “giving way” showed an even more impressive correction. While 80% of patients had a positive pivot shift before surgery, 93.3% reached a negative/normal status postoperatively, highlighting the graft’s efficacy in restoring the complex kinematics required for pivoting and sports (Table 4).
- Mechanical reliability: The high conversion rate from Grade II/III instability to “Normal” status underscores the structural stiffness of the tripled PLT, which provides a restraint comparable to the native ACL (Table 4).
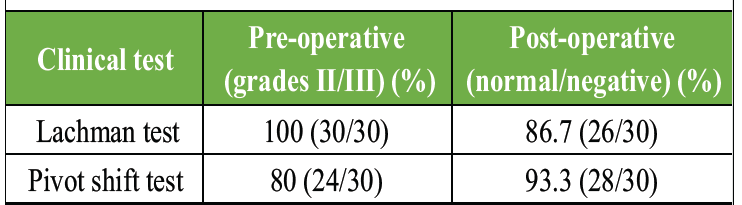
Table 4: Evolution of clinical stability (pre-op vs. 6 months)
Donor-site morbidity and complications
The assessment of the ankle and foot via AOFAS and FADI scores revealed minimal functional deficit following graft harvest.
<H3>Functional integrity and stability
- Negligible score variance: The AOFAS and FADI scores remained remarkably stable, with a decline of <1% from pre-operative levels. This near-perfect maintenance of scores (moving from 98.2 to 98.0 and 99.1 to 99.0) indicates that the foot and ankle’s complex biomechanics remain intact after harvest (Table 5).
- Successful synergy: The data suggest that the synergistic action of the peroneus brevis and other everters effectively compensates for the PLT harvest, maintaining the medial longitudinal arch and gait stability (Table 5).
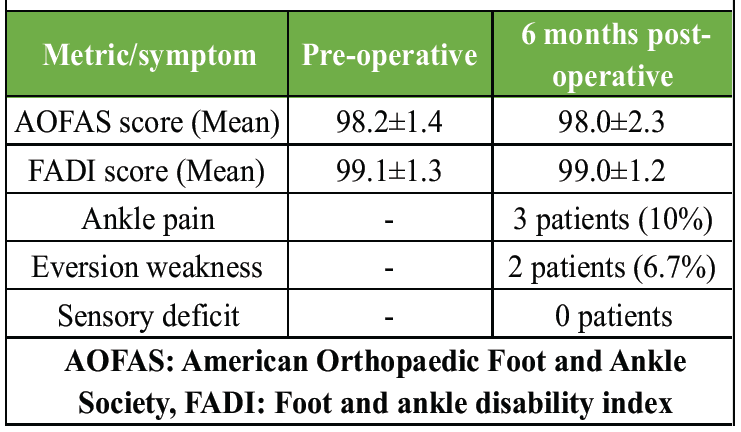
Table 5: Ankle function and donor-site issues
Morbidity profile
- Minimal clinical footprint: Only 10% of patients reported minor ankle pain, and a mere 6.7% (2 out of 30) exhibited mild eversion weakness, which did not iTampact daily activities (Table 5).
- Neurovascular safety: The 0% incidence of sensory deficits validates the harvesting technique, specifically the safety margin maintained to protect the superficial peroneal nerve (Table 5).
The complication profile highlights the safety and structural reliability of the peroneus longus autograft, characterized by an exceptionally low rate of adverse events (Table 6). The 0% graft failure rate is the most significant finding, confirming the biological and mechanical robustness of the tripled PLT during the critical early healing phase (Table 6). The absence of major ankle-related complications (0%) reinforces that harvesting this tendon when combined with a distal tenodesis is a safe procedure that does not jeopardize joint stability. The most common minor issue (Knee Stiffness n = 2), typically associated with post-operative rehabilitation compliance rather than the graft source itself. A single case was successfully managed with standard care, indicating no inherent increased risk of infection with this technique (Table 6).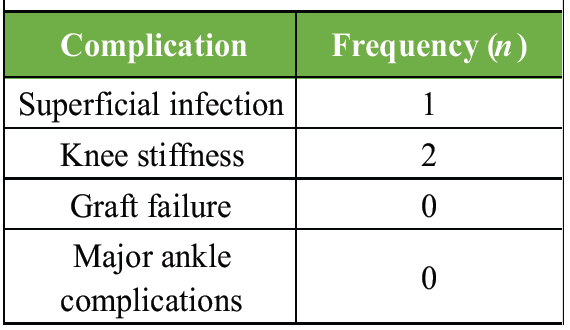
Given that 90% of our cohort were young adults in their peak productive years (Table 2), the PLT offers a distinct cultural advantage. In a population where squatting, sitting cross-legged, and barefoot ambulation are daily necessities, avoiding the donor-site pain of patellar grafts or the flexor weakness of hamstring grafts is a significant clinical victory [15]. Rhatomy et al. [16] reported a mean age of 26.8 years, while Kusumastutia et al. [17] and Rajani et al. [18] observed mean ages ranging from 24 to 30 years. Indian studies by Miu et al. [19] and Agrawal et al. [20] similarly documented that more than 80% of their patients were below 35 years. The concordance of the present findings with those reported in the literature indicates that the study population is broadly representative of the typical demographic undergoing ACL reconstruction with a peroneus longus graft. Although recent randomized controlled trials, systematic reviews, and meta-analyses have already demonstrated that the PLT is a viable alternative autograft for ACL reconstruction, [12,14,15,21,22] prospective data from the Indian population remain comparatively limited. This is particularly relevant in individuals with high functional demands involving squatting, barefoot ambulation, and cross-legged sitting. The present study contributes prospective short-term clinical data evaluating both knee functional recovery and donor-site morbidity using standardized outcome measures such as Lysholm, AOFAS, and FADI scores. Our findings support the growing body of evidence suggesting that PLT autografts can provide satisfactory functional outcomes with minimal ankle-related morbidity. Selection of an appropriate ACL autograft requires balancing biomechanical strength, graft adequacy, and donor-site morbidity. Our findings suggest that the full-thickness tripled PLT) achieves this equilibrium, providing a robust scaffold for the knee while preserving the functional integrity of the ankle. A critical determinant of ACL reconstruction success is graft diameter; literature suggests that grafts smaller than 8 mm are significantly more prone to failure [10]. In our cohort, the mean graft diameter was a substantial 8.7 ± 0.6 mm, achieved consistently through a tripled configuration. This anatomical advantage providing a mean length of 26.4 cm directs correlates with our 0% graft failure rate, reinforcing the PLT’s role as a structurally superior alternative to the often-variable and thinner hamstring tendons [10,12]. The primary objective of ACL reconstruction is the elimination of the giving way phenomenon and the prevention of secondary meniscal damage [7,23]. Our results demonstrated a transformative shift in joint kinematics-the transition of 93.3% of patients to a negative Pivot Shift (Table 4) is particularly noteworthy. This suggests that the inherent stiffness of the PLT autograft effectively restores the complex rotational constraints of the native ACL [11,24]. The leap in Lysholm scores from 54.6 to 91.3 (Table 3) represents a 67% improvement in subjective function. This mirrors the clinical success of the “gold standard” BPTB graft but without the associated morbidity of anterior knee pain and extensor mechanism dysfunction [9,25]. Apprehensions regarding harvesting a primary ankle evertor have historically limited PLT utilization. However, our study provides objective evidence to the contrary, the negligible variance in AOFAS and FADI scores (Table 5) supports the theory of “synergistic compensation.” By performing a distal tenodesis of the PLT stump to the peroneus brevis, the lateral column stability and medial longitudinal arch are preserved [14]. The absence of sensory deficits (0%) validates our harvesting technique, specifically the safety margin maintained 4–5 cm distal to the fibular head to protect the common peroneal nerve [26].
Mild ankle pain and eversion weakness were observed in a small proportion of patients, with no instability or sensory deficits (Table 5). These findings are comparable to those reported by Agrawal et al. [20], Jadhav et al. [27], and Singh et al. [28]. Importantly, no patient reported functional limitation in daily activities, supporting the safety profile of peroneus longus harvest. The present study recorded a low incidence of post-operative complications. Superficial infection occurred in one patient and resolved with conservative management with oral and local antibiotics with regular dressings. Knee stiffness was noted in two patients, both of whom improved with physiotherapy. Importantly, no graft failures or major ankle-related complications were observed. Rajani et al. [18] reported superficial infection rates of 3–5% with no graft failures. Agrawal et al. [20] similarly reported low complication rates and absence of ankle instability. Systematic reviews by Quinn et al. [21] and Soleymanha et al. [22] concluded that peroneus longus grafts do not increase complication risk compared to hamstring grafts. The low complication rate in the present study further supports the safety and reproducibility of this technique when performed with meticulous surgical technique and standardized rehabilitation.
Limitations
The present study has several limitations. The relatively small sample size and short duration of recruitment may limit broader generalizability of the findings. As this was a single-center study conducted in a resource-constrained tertiary care setting, multicentric studies are required for wider external validation. Longer follow-up studies are necessary to evaluate long-term graft survivorship and late complications. The absence of a comparative control group such as hamstring tendon autografts limits direct comparative interpretation. Additionally, objective biomechanical assessment of ankle eversion strength and gait analysis were not performed.
The present prospective study demonstrates that the full-thickness tripled PLT autograft provides satisfactory short-term functional and stability outcomes following arthroscopic ACL reconstruction, with minimal donor-site morbidity. The graft consistently achieved adequate diameter while preserving ankle function as assessed by AOFAS and FADI scores. Although recent literature has already established PLT as a viable graft option, the present study contributes prospective clinical data from an Indian population with high functional demands. Larger comparative studies with longer follow-up are required to further validate long-term outcomes and graft survivorship.
Peroneus longus tendon autograft provides adequate graft diameter and satisfactory short-term functional outcomes in ACL reconstruction with minimal donor-site morbidity, making it a viable option in patients where hamstring graft size may be inadequate.
References
- 1. Griffin LY, Agel J, Albohm MJ, Arendt EA, Dick RW, Garrett WE, et al. Noncontact anterior cruciate ligament injuries: Risk factors and prevention strategies. J Am Acad Orthop Surg 2000;8:141-50. [Google Scholar] [PubMed]
- 2. Moses B, Orchard J, Orchard J. Systematic review: Annual incidence of ACL injury and surgery in various populations. Res Sports Med 2012;20:157-79. [Google Scholar] [PubMed]
- 3. Mlv SK, Mahmood A, Vatsya P, Garika SS, Mittal R, Nagar M. Demographic characteristics of patients who underwent anterior cruciate ligament reconstruction at a tertiary care hospital in India. World J Clin Cases 2023;11:3464. [Google Scholar] [PubMed]
- 4. Dhillon MS, Rakesh J, Sharma S, Prabhakar S, Behera P, Saxena S, et al. Epidemiology of knee injuries in Indian Kabaddi players. Asian J Sports Med 2017;8:e31670. [Google Scholar] [PubMed]
- 5. Butler DL, Noyes FR, Grood ES. Ligamentous restraints to anterior-posterior drawer in the human knee. J Bone Joint Surg 1980;62:259-70. [Google Scholar] [PubMed]
- 6. Shelbourne KD, Gray T. Minimum 10-year results after ACL reconstruction. Am J Sports Med 2009;37:471-80. [Google Scholar] [PubMed]
- 7. Rahardja R, Love H, Clatworthy MG, Young SW. Delayed reconstruction is associated with higher rates of medial meniscus and chondral injury following ACL injury: A New Zealand ACL registry study. Knee Surg Sports Traumatol Arthrosc 2025;33(1):1-8. [Google Scholar] [PubMed]
- 8. Fu FH, Bennett CH, Ma CB, Menetrey J, Lattermann C. Current trends in anterior cruciate ligament reconstruction. Part II. Operative procedures and clinical correlations. Am J Sports Med 2000;28:124-30. [Google Scholar] [PubMed]
- 9. Corry IS, Webb JM, Clingeleffer AJ, Pinczewski LA. Arthroscopic reconstruction of the anterior cruciate ligament. A comparison of patellar tendon autograft and four-strand hamstring tendon autograft. Am J Sports Med 1999;27:444-54. [Google Scholar] [PubMed]
- 10. Conte EJ, Hyatt AE, Gatt CJ Jr., Dhawan A. Hamstring autograft size can be predicted and is a potential risk factor for anterior cruciate ligament reconstruction failure. Arthroscopy 2014;30:882-90. [Google Scholar] [PubMed]
- 11. Geib TM, Shelton WR, Phelps RA, Clark L. Anterior cruciate ligament reconstruction using quadriceps tendon autograft: Intermediate-term outcome. Arthroscopy 2009;25:1408-14. [Google Scholar] [PubMed]
- 12. Opoku M, Abdramane AM, Abdirahman A, Fang M, Li Y, Xiao W. Can peroneus longus tendon autograft become an alternative to hamstring tendon autograft for anterior cruciate ligament reconstruction: A systematic review and meta-analysis of comparative studies. J Orthop Surg Res 2025;20:719. [Google Scholar] [PubMed]
- 13. Simonson R, Piussi R, Högberg J, Senorski C, Thomeé R, Samuelsson K, et al. Effect of quadriceps and hamstring strength relative to body weight on risk of a second ACL injury: A cohort study of 835 patients who returned to sport after ACL reconstruction. Orthop J Sports Med 2023;11:1-8 (23259671231157386). [Google Scholar] [PubMed]
- 14. Saoji A, Arora M, Jain G, Shukla T. There is a minimal difference in ankle functional outcomes after peroneus longus harvest: Systematic review and meta-analysis. Indian J Orthop 2023;57:1993-9. [Google Scholar] [PubMed]
- 15. Vijay C, Santosh MS, Avinash C, Adarsh T. Is Peroneus longus autograft a better alternative to the Hamstring autograft for anterior cruciate ligament reconstruction?- A randomised control study. J Orthop Trauma Rehabil 2022;29(1):1-9 (22104917221088335). [Google Scholar] [PubMed]
- 16. Rhatomy S, Hartoko L, Setyawan R, Soekarno NR, Asikin AI, Pridianto D, et al. Single bundle ACL reconstruction with peroneus longus tendon graft: 2-Years follow-up. J Clin Orthop Trauma 2020;11:S332-6. [Google Scholar] [PubMed]
- 17. Kusumastutia AH, Rukmoyo T, Rhatomy S, Sakti YM. Anterior cruciatel ligament reconstruction with peroneus longus tendon autograft: Functional outcome and donor site morbidity. Orthop J Sports Med 2020;8(5):2325967120S00084. [Google Scholar] [PubMed]
- 18. Rajani AM, Shah UA, Mittal AR, Rajani A, Punamiya M, Singhal R. Functional and clinical outcome of anterior cruciate ligament reconstruction with peroneus longus autograft and correlation with MRI after 3 years. J Orthop 2022;34:215-20. [Google Scholar] [PubMed]
- 19. Miu CA, Hurmuz M, Miu LO, Ceachir D, Tatu RF. Reconstruction of chronic quadriceps and achilles tendon ruptures using achilles allografts: Clinical findings and review of literature. Biomedicines 2025;13:816. [Google Scholar] [PubMed]
- 20. Agrawal V, Ravikiran HG, Santhosh MS, Vijay C, Prashasth BS, Chandra A. Assessment of functional outcome and donor site morbidity in anterior cruciate ligament reconstruction using peroneus longus autograft. J Med Sci Health 2022;8:22-7. [Google Scholar] [PubMed]
- 21. Quinn M, Byrne RA, Albright JA, Testa E, Ahn B, Lemme N, et al. Peroneus longus tendon autograft may present a viable alternative for anterior cruciate ligament reconstruction: A systematic review. Arthroscopy 2024;40:1366-76.e1. [Google Scholar] [PubMed]
- 22. Soleymanha M, Soleymani Nejad A, Keyhani S, Vosoughi F, LaPrade RF, Tollefson LV. Peroneus longus tendon harvest for ACL reconstruction yields good functional outcome of the ankle: A systematic review and meta-analysis. Knee Surg Sports Traumatol Arthrosc 2025;33(1):1-14. [Google Scholar] [PubMed]
- 23. Andriacchi TP, Dyrby CO. Interactions between kinematics and loading during walking for the normal and ACL deficient knee. J Biomech 2005;38:293-8. [Google Scholar] [PubMed]
- 24. Teja KC, Kumar S, Kumar A, Haripriya H. Long-term outcomes of anterior cruciate ligament reconstruction: Peroneus longus versus hamstring tendons. J Arthrosc Surg Sports Med 2025;6:174-8. [Google Scholar] [PubMed]
- 25. Kartus J, Stener S, Lindahl S, Engström B, Eriksson BI, Karlsson J. Factors affecting donor-site morbidity after anterior cruciate ligament reconstruction using bone-patellar tendon-bone autografts. Knee Surg Sports Traumatol Arthrosc 1997;5:222-8. [Google Scholar] [PubMed]
- 26. Hurley ET, Davey MS, Jamal MS, Manjunath AK, Kingery MT, Alaia MJ, et al. High rate of return-to-play following meniscal allograft transplantation. Knee Surg Sports Traumatol Arthrosc 2020;28:3561-8. [Google Scholar] [PubMed]
- 27. Jadhav R, Bhardwaj V. Assessment of donor site morbidity and ankle stability after management of anterior cruciate ligament reconstruction with peroneus longus autograft- a prospective study in Indian patients. Glob J Res Anal 2024;13 (3):1-5. [Google Scholar] [PubMed]
- 28. Singh MP, Verma M, Agrawal DR, Gaur TN, Maravi DS, Dhanopeya A. Evaluation of ankle complications after peroneus longus tendon harvesting for ACL reconstruction. J Orthop Case Rep 2025;15:207-12. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide
June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide May 1, 2026 Comparative Evaluation of Peroneus Longus Tendon and Hamstring Tendon Autografts in Primary Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Trial
May 1, 2026 Comparative Evaluation of Peroneus Longus Tendon and Hamstring Tendon Autografts in Primary Anterior Cruciate Ligament Reconstruction: A Randomized Controlled Trial November 1, 2024 Randomized Controlled Study Comparing Hamstring Graft and Peroneus Longus Tendon Graft in Arthroscopic ACL Reconstruction
November 1, 2024 Randomized Controlled Study Comparing Hamstring Graft and Peroneus Longus Tendon Graft in Arthroscopic ACL Reconstruction July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction
July 1, 2026 Role of Meniscal Ramp Lesion Repair in Preventing Residual Instability after Anterior Cruciate Ligament Reconstruction