
Arthroscopic rotator cuff repair provides significant improvement in pain and shoulder function. Routine acromioplasty does not confer additional clinical benefit and should be performed selectively.
Dr Puneet Kamra, Department of Orthopaedics, Faculty of Medicine and Health Sciences, SGT University, Gurugram, Haryana, India. E-mail: puneetpgi292@gmail.com
Abstract
Background: Arthroscopic rotator cuff repair (ARCR) is a widely accepted treatment for symptomatic rotator cuff tears. Acromioplasty is frequently performed to reduce subacromial impingement; however, its routine use remains controversial. The purpose of this study was to compare the functional and clinical outcomes of ARCR performed with and without acromioplasty.
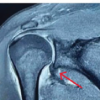
Materials and Methods: This is a prospective comparative study that involved 50 participants who had tears in their rotator cuff muscles. These were grouped into two equal numbers: Group A, consisting of ARCR with acromioplasty (n = 25), and Group B, consisting of ARCR without acromioplasty (n = 25). The participants were aged between 30 and 70 years and had tears in their rotator cuff muscles confirmed by a magnetic resonance imaging scan and had failed conservative management. Patients were followed for 6 months postoperatively. The results were evaluated using the Visual Analogue Scale (VAS) score for pain, Constant-Murley Score, University of California-Los Angeles (UCLA) Shoulder Score, and range of motion (ROM).
Results: The majority of patients were aged 41–60 years (60%), with male predominance (66%). Pre-operative VAS scores were comparable (7.8 ± 0.9 vs. 7.6 ± 1.0; P = 0.42). At 6 months, significant pain reduction was observed in both groups (VAS: 2.1 ± 0.8 vs. 2.3 ± 0.9; P = 0.38). Functional outcomes improved substantially, with Constant scores increasing to 78.6 ± 6.3 in Group A and 76.9 ± 6.8 in Group B (P = 0.29) and UCLA scores of 30.2 ± 3.5 and 29.5 ± 3.8, respectively (P = 0.47). ROM improved in both groups without significant differences. Complication rates were similar, with re-tears observed in 8% of cases in each group.
Conclusion: Both techniques resulted in significant improvement in pain and function. Routine acromioplasty did not provide additional clinical benefit and should be considered selectively.
Keywords: Arthroscopic repair, acromioplasty, rotator cuff tear, shoulder function, subacromial impingement.
Arthroscopic rotator cuff repair (ARCR) has become the gold standard for the management of symptomatic rotator cuff tears that fail conservative treatment, owing to its minimally invasive nature, reduced post-operative morbidity, and improved functional outcomes. The population over 50 years old shows a significant increase in rotator cuff tears, which serve as the primary reason for shoulder pain and disability [1]. The development of rotator cuff tears involves multiple factors, which include intrinsic tendon degeneration and hypovascularity and external mechanical impingement. “[1.1] Subacromial impingement, which results from acromion morphology, functions as an external factor that historically serves as a major cause of rotator cuff disorders. The medical field adopted acromioplasty as a surgical method which reshapes the acromion undersurface to reduce impingement and provide additional room for rotator cuff tendons [2].
Neer popularised the procedure of acromioplasty through his research study, which showed that rotator cuff tendon degeneration and tearing occurred when mechanical abrasion happened to the cuff tissue located under the anterior acromion and coracoacromial ligament [3]. The surgical method, which combined acromioplasty and rotator cuff repair, emerged as the most commonly used procedure during the following years. The procedure aimed to achieve two outcomes by first removing the acromial spur and second creating space for decompression, which would decrease mechanical irritation and promote tendon healing while stopping any potential re-tear from occurring [4]. The need for doctors to perform acromioplasty procedures as standard practice has decreased due to improvements in arthroscopic methods and increased knowledge about rotator cuff biology. The studies show that intrinsic degeneration has a greater impact on how rotator cuff tears develop than extrinsic impingement does [5]. The histopathological analyses revealed that age-related changes lead to tendon problems because they cause collagen disorganisation and tenocyte apoptosis and reduced vascularity, which affect tendon integrity through mechanisms that do not depend on acromial shape [6]. The development of double-row fixation, along with biological augmentation, has brought about major advancements in surgical methods, which lead to better tendon healing results that reduce the extra advantages brought by acromioplasty procedures [7]. The results of randomised controlled trials, together with meta-analyses, have studied ARCR outcomes with and without acromioplasty, which produced inconsistent findings. The research studies show that patients who underwent rotator cuff repair with acromioplasty experienced identical pain relief and functional results and re-tear rates as their counterparts who did not receive acromioplasty treatment [8]. The research results demonstrate that acromioplasty should not be performed as a common procedure because it does not benefit certain groups of patients who do not have major acromial spurs or type III (hooked) acromion. The research results show that acromioplasty provides extra advantages in specific situations because it helps to increase subacromial space while decreasing post-operative impingement issues. The different research outcomes have created a continuing discussion about when to perform acromioplasty together with rotator cuff repair [9]. Neuroplasticity is the brain’s ability to change and adapt by making new connections between brain cells throughout life. This is especially evident during early childhood, where pruning and myelination of brain cells are active. Studies have shown that environmental stimulation and learning have a direct effect on the thickness of the cortex and the branching of dendrites. Functional magnetic resonance imaging (MRI) has also shown that the adult brain is capable of neuroplasticity, which helps the brain to heal from injuries and learn new things. The neuroplasticity model has significant implications for the fields of education and rehabilitation medicine [10]. In view of such divergent views, there clearly is a need for adequately conducted comparative clinical studies to determine the real effect that acromioplasty will have when carried out concurrently with ARCR surgery. This is crucial for determining guidelines that can help make optimal decisions. The current study was designed to conduct an analysis of the effects of ARCR surgery with and without acromioplasty.
Study design:
This prospective comparative clinical study was conducted in the Department of Orthopaedics of a tertiary care teaching hospital equipped with advanced arthroscopic surgical facilities. The study was carried out over a period of 18 months, including patient recruitment, surgical intervention, and post-operative follow-up, with the objective of evaluating the functional and clinical outcomes of ARCR performed with versus without acromioplasty. The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all patients before their inclusion in the study.
Participants:
Patients presenting with symptomatic rotator cuff tears and meeting the eligibility criteria were included in the study.
Inclusion criteria :
- Patients aged between 30 and 70 years
- Clinically and radiologically confirmed rotator cuff tear (MRI-based diagnosis)
- Patients with persistent symptoms not responding to conservative management for at least 3 months
- Patients willing to undergo ARCR
- Patients providing informed consent.
Exclusion criteria:
- Patients with massive irreparable rotator cuff tears
- Previous shoulder surgery on the affected side
- Associated shoulder instability or fracture
- Advanced glenohumeral arthritis
- Neuromuscular disorders affecting shoulder function
- Patients unwilling or unable to comply with follow-up protocol.
Study sampling:
A consecutive sampling method was employed in which all eligible patients presenting during the study period were included until the required sample size was achieved. This method ensured minimization of selection bias and allowed for representation of routine clinical cases encountered in the hospital setting.
Study sample size:
A total of 50 patients were included in the study. The sample size was determined based on the expected number of eligible patients presenting during the study period, feasibility considerations, and previously published comparative studies evaluating outcomes following ARCR. No formal a priori sample size calculation was performed.
Study groups:
Patients were allocated to either the acromioplasty or non-acromioplasty group according to the operating surgeon’s intraoperative assessment, acromial morphology, extent of subacromial impingement, and clinical judgement. Allocation was not randomised. Baseline demographic and clinical characteristics were compared to ensure group comparability.
Study parameters:
The primary outcome measure of the study was functional recovery assessed using the Constant-Murley Score. Secondary outcome measures included pain assessment using the Visual Analogue Scale (VAS), functional evaluation using the University of California-Los Angeles (UCLA) Shoulder Score, post-operative range of motion (ROM) (abduction, flexion, and external rotation), re-tear rate, and the incidence of post-operative complications, including stiffness, infection, and tendon re-tear. These parameters were evaluated preoperatively and during follow-up to compare the clinical effectiveness of ARCR performed with and without acromioplasty.
Study procedure:
All patients were subjected to a comprehensive pre-operative evaluation that included clinical assessment and an MRI scan of the shoulder joint to diagnose the pathology and analyze the tear. The surgical procedure was conducted under general anaesthesia in the beach-chair or lateral decubitus position. The posterior, anterior, and lateral standard portals were employed for the procedure. Initially, diagnostic arthroscopy was performed to evaluate the intra-articular structures. Rotator cuff repair was done by either a single or double row of sutures based on the tear dimensions and anatomy. Acromioplasty was done in Group A patients using a motorised burr for the contouring and debridement of the undersurface of the acromion bone. No acromioplasty was done in Group B patients. Postoperatively, the rehabilitation protocol included immobilisation in a shoulder sling and progressive physiotherapy.
Study data collection:
The data collection process entailed the use of a structured pro forma form before and after follow-up. Before surgery, demographic data, clinical findings, and imaging data were collected. Data after surgery were collected at 6-week, 3-month, and 6-month intervals. The pain, functional score, and ROM were measured for each follow-up interval.
Data analysis:
Data analysis involved entry of collected data into Microsoft Excel and analysis of the data using statistical software like the Statistical Package for the Social Sciences (SPSS). Data that were quantitative were presented in terms of mean and standard deviation, while qualitative data were presented in terms of frequency and percentages. Comparison between the two sets of data was done using relevant statistical tests like the independent t-test and the Chi-square test, respectively. A level of significance of P < 0.05 was adopted throughout the study.
A total of 50 patients with symptomatic rotator cuff tears were included in the study and equally allocated to Group A (ARCR with acromioplasty, n = 25) and Group B (ARCR without acromioplasty, n = 25). The majority of patients were between 41 and 60 years of age (60%), with a male predominance (66%). The right shoulder was more commonly involved (70%), and full-thickness tears accounted for 62% of all cases. Baseline demographic and clinical characteristics were comparable between the groups, with no statistically significant differences in age, sex distribution, side involved, or tear characteristics (all P > 0.05) (Table 1).
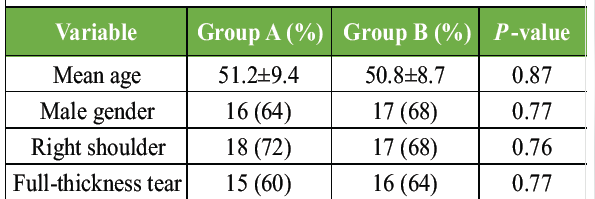
Table 1: Baseline demographic and clinical characteristics
Both groups demonstrated substantial improvement in pain and shoulder function at 6 months’ follow-up. Pre-operative VAS scores were similar between Group A and Group B (7.8 ± 0.9 vs. 7.6 ± 1.0; P = 0.42), improving to 2.1 ± 0.8 and 2.3 ± 0.9, respectively (P = 0.38). Functional outcomes also improved significantly in both groups. The mean Constant-Murley score increased to 78.6 ± 6.3 in Group A and 76.9 ± 6.8 in Group B (P = 0.29), while the mean UCLA Shoulder Score was 30.2 ± 3.5 and 29.5 ± 3.8, respectively (P = 0.47). ROM improved similarly in both groups, with no statistically significant differences in abduction, flexion, or external rotation (Table 2 and Fig. 1).
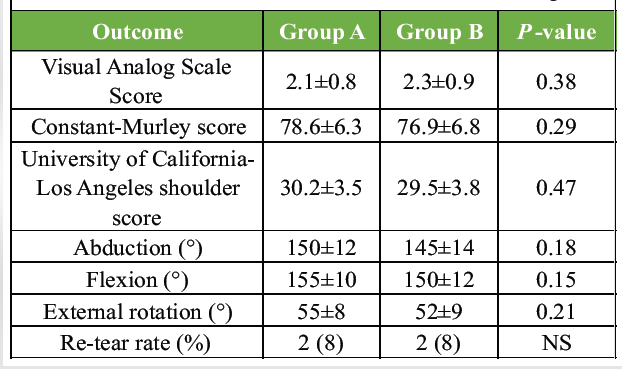
Table 2: Clinical outcomes at 6 months follow-up
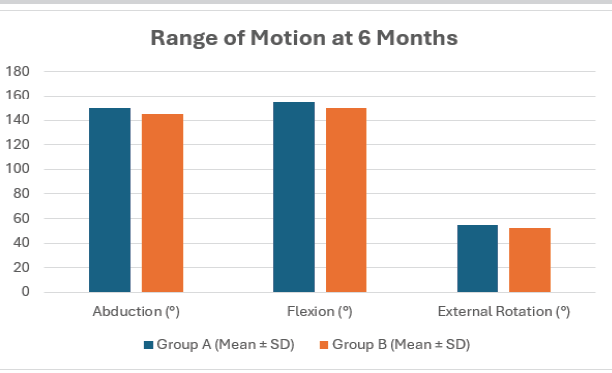
Figure 1: Comparison of post-operative functional outcomes and range of motion between arthroscopic rotator cuff repair with and without acromioplasty at 6 months follow-up.
Post-operative complications were infrequent and comparable between the groups. Stiffness occurred in 10% of patients, infection in 4%, and re-tearing in 8%, with no significant difference between treatment groups. Overall, 78% of patients experienced no post-operative complications (Fig. 2). These findings suggest that the addition of acromioplasty did not confer a significant clinical advantage in terms of pain relief, functional recovery, ROM, or complication rates.
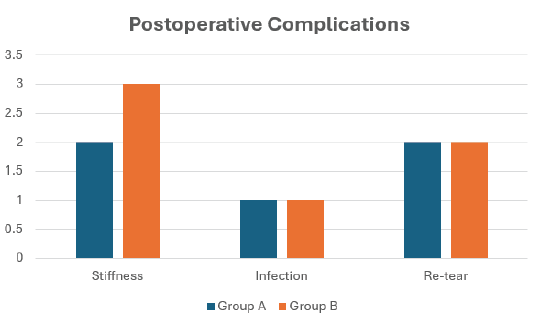
Figure 2: Distribution of post-operative complications in patients undergoing arthroscopic rotator cuff repair with and without acromioplasty.
The current prospective comparative study examined the impact of acromioplasty in ARCR and found that both cohorts, with regard to pain relief, functional outcomes, and ROM, gained similar improvements at no statistical differences between them. Such data contribute to the discussion concerning the requirement for the regular procedure in the context of ARCR and agree with previous literature emphasising that acromioplasty might not be indispensable and should be conducted selectively. Regarding demographics, it was noted that most participants belonged to the 41–60 years old cohort (60%), with the male gender dominating (66%). Besides, 70% of patients suffered from the right shoulder. All these figures are in accordance with the known epidemiology of rotator cuff injuries since middle-aged people and the dominant limb have an increased probability of tears due to degeneration and overuse. More importantly, both patient cohorts had matching features at baseline, such as pain score (VAS: 7.8 ± 0.9 in Group A vs. 7.6 ± 1.0 in Group B; P = 0.42). Post-operative outcomes in the present study demonstrated significant pain reduction in both groups, with mean VAS scores improving to 2.1 ± 0.8 in the acromioplasty group and 2.3 ± 0.9 in the non-acromioplasty group at 6 months (P = 0.38). Similarly, functional outcomes improved markedly, with Constant-Murley scores increasing from 42.5 ± 5.2 to 78.6 ± 6.3 in Group A and from 43.1 ± 5.0 to 76.9 ± 6.8 in Group B (P = 0.29). UCLA scores were also comparable between groups (30.2 ± 3.5 vs. 29.5 ± 3.8; P = 0.47). ROM parameters showed improvement in both groups, with no statistically significant differences in abduction (150° vs. 145°; P = 0.18), flexion (155° vs. 150°; P = 0.15), or external rotation (55° vs. 52°; P = 0.21). These findings collectively indicate that acromioplasty did not provide additional clinical or functional benefit in the short-term post-operative period. These results are in strong agreement with the randomised controlled trial by MacDonald et al. [11], which demonstrated that both Western Ontario Rotator Cuff (WORC) and American Shoulder and Elbow Surgeons (ASES) scores improved significantly over time in both groups (P < 0.001), with no significant differences between patients undergoing rotator cuff repair with or without acromioplasty at any follow-up interval. This consistency reinforces the conclusion that functional recovery is largely driven by tendon repair rather than subacromial decompression. Long-term evidence further supports these findings. Woodmass et al. [12] reported no significant difference in WORC scores between the two groups at a mean follow-up of over 11 years (P = 0.30), indicating that the absence of acromioplasty does not adversely affect long-term functional outcomes. Similarly, Waterman et al. [13], in a study with a mean follow-up of 7.5 years, found no statistically significant differences in ASES (P = 0.33), VAS pain (P = 0.79), Constant (P = 0.17), or UCLA scores (P = 0.19) between the groups. These findings closely mirror the present study results, where no significant differences were observed in similar outcome measures. Meta-analytic evidence also supports the lack of clinically meaningful benefit of acromioplasty. Sayampanathan et al. [14], in a meta-analysis involving 3,034 shoulders, reported no significant differences in ASES (standardised mean difference [SMD] 0.09; P = 0.36) or UCLA scores (SMD 0.17; P = 0.17) between the two groups. Although a statistically significant difference in the constant score was observed (SMD 0.25; P = 0.03), the magnitude of this difference was not clinically significant. This finding aligns with the present study, where a slight numerical advantage was observed in Constant scores in the acromioplasty group (78.6 vs 76.9), but without statistical significance (P = 0.29). However, an important aspect highlighted in both previous literature and the present study is the trend toward higher reoperation rates in patients who did not undergo acromioplasty. In the current study, re-tear rates were equal in both groups (8%), but previous studies suggest a different trend. MacDonald et al. reported a higher rate of additional surgery in the non-acromioplasty group (9%) compared to the acromioplasty group. Similarly, Woodmass et al. [12] observed a significantly higher reoperation rate in the non-acromioplasty group (16% vs. 2%) over long-term follow-up. Furthermore, Maguire et al. [15] reported reoperation rates of 15% in the non-acromioplasty group compared to 4.1% in the acromioplasty group (P = 0.031), particularly in patients with type III acromion. These findings suggest that while functional outcomes may be similar, acromioplasty may reduce the likelihood of revision surgery in selected patients. In the present study, complication rates were low and comparable between groups, with stiffness observed in 10%, infection in 4%, and re-tear in 8% of cases. A majority (78%) had no complications, indicating that both procedures are safe and effective. These findings are consistent with previous studies, which have also reported similar complication and re-tear rates between groups. The findings of this study strongly support the notion that routine acromioplasty is not necessary in all patients undergoing arthroscopic rotator cuff repair.” The lack of any difference between the two groups concerning pain relief (VAS 2.1 and 2.3), function (Constant score 78.6 and 76.9; UCLA 30.2 and 29.5), and ROM points to the importance of tendon healing and repair in the postoperative period compared to subacromial decompression. Nevertheless, the higher incidence of reoperations in previous studies in the non-acromioplasty group implies that acromioplasty could be considered in some cases, especially those with certain morphologies of the acromion, such as Types II or III. The present study evaluated outcomes at a short-term follow-up of 6 months. Although significant improvements in pain and function were observed, longer follow-up is necessary to determine the effect of acromioplasty on tendon healing, re-tear rates, degenerative progression, and revision surgery. Therefore, in conclusion, the current study, along with other literature data, implies that surgeons need not perform acromioplasty systematically but selectively, considering the peculiarities of each patient. Further studies with a higher number of participants and extended periods of observation are needed to provide further clarification on this issue and develop more exact surgical techniques. The strengths of this study include its prospective design and standardised functional assessment. However, limitations include the relatively small sample size, short follow-up period, and non-randomised group allocation. Larger randomised studies with longer follow-up are required.
ARCR, both with and without acromioplasty, has been found to be effective in reducing pain, improving function, and increasing ROM in patients with rotator cuff tears. While there was a slight improvement in the results of those who underwent acromioplasty, no statistical significance could be established, which means that acromioplasty does not provide any additional benefit over rotator cuff repair alone. There was also no difference between the two procedures in terms of safety. Hence, the procedure of acromioplasty need not always be included in rotator cuff repairs.
Routine acromioplasty is not required during arthroscopic rotator cuff repair. Selective use based on acromial anatomy may optimize surgical outcomes.
References
- 1. Abrams GD, Gupta AK, Hussey KE, Tetteh ES, Karas V, Bach BR Jr, et al. Arthroscopic repair of full-thickness rotator cuff tears with and without acromioplasty: randomised prospective trial with 2-year follow-up. Am J Sports Med 2014;42:1296-303. [Google Scholar] [PubMed]
- 2. Menekse S. Comparison of outcomes between open and arthroscopic rotator cuff repair. Adv Orthop 2024;2024:5575404. [Google Scholar] [PubMed]
- 3. American Academy of Orthopaedic Surgeons. Management of Rotator Cuff Injuries: Evidence-Based Clinical Practice Guideline. United States: American Academy of Orthopaedic Surgeons; 2019. [Google Scholar] [PubMed]
- 4. Balke M, Schmidt C, Dedy N, Banerjee M, Bouillon B, Liem D. Correlation of acromial morphology with impingement syndrome and rotator cuff tears. Acta Orthop 2013;84:178-83. [Google Scholar] [PubMed]
- 5. Shin SJ, Oh JH, Chung SW, Song MH. The efficacy of acromioplasty in the arthroscopic repair of small- to medium-sized rotator cuff tears without acromial spur: a prospective comparative study. Arthroscopy 2012;28:628-35. [Google Scholar] [PubMed]
- 6. Budoff JE, Nirschl RP, Guidi EJ. Débridement of partial-thickness tears of the rotator cuff without acromioplasty. Long-term follow-up and review of the literature. J Bone Joint Surg Am 1998;80:733-48. [Google Scholar] [PubMed]
- 7. Cheng C, Chen B, Xu H, Zhang Z, Xu W. Efficacy of concomitant acromioplasty in the treatment of rotator cuff tears: A systematic review and meta-analysis. PLoS One 2018;13:e0207306. [Google Scholar] [PubMed]
- 8. Mohtadi NG, Hollinshead RM, Sasyniuk TM, Fletcher JA, Chan DS, Li FX. A randomised clinical trial comparing open to arthroscopic acromioplasty with mini-open rotator cuff repair for full-thickness rotator cuff tears: disease-specific quality of life outcome at an average 2-year follow-up. Am J Sports Med 2008;36:1043-51. [Google Scholar] [PubMed]
- 9. Coleman BD, Khan HM, Maffulli N, Cook JL, Wark JD. Studies of surgical outcome after patellar tendinopathy: Clinical significance of methodological deficiencies and guidelines for future studies. Victorian Institute of Sport Tendon Study Group. Scand J Med Sci Sports 2000;10:2-11. [Google Scholar] [PubMed]
- 10. Khazzam M. Settling the controversy of acromioplasty during rotator cuff repair: Commentary on an article by Jarrett M. Woodmass, MD, FRCSC, et al.: “Arthroscopic rotator cuff repair with and without acromioplasty in the treatment of full-thickness rotator cuff tears. Long-term outcomes of a multicenter, randomised controlled trial”. J Bone Joint Surg Am 2022;104:2130. [Google Scholar] [PubMed]
- 11. MacDonald P, McRae S, Leiter J, Mascarenhas R, Lapner P. Arthroscopic rotator cuff repair with and without acromioplasty in the treatment of full-thickness rotator cuff tears: A multicentre, randomised controlled trial. J Bone Joint Surg Am 2011;93:1953-60. [Google Scholar] [PubMed]
- 12. Woodmass JM, Al Khatib L, McRae S, Lapner P, Mascarenhas R, Neogi D, et al. Arthroscopic rotator cuff repair with and without acromioplasty in the treatment of full-thickness rotator cuff tears: Long-term outcomes of a multicentre, randomised controlled trial. J Bone Joint Surg 2022;104:2101-7. [Google Scholar] [PubMed]
- 13. Waterman BR, Newgren J, Gowd AK, Cabarcas B, Lansdown D, Bach BR, et al. Randomised trial of arthroscopic rotator cuff with or without acromioplasty: No difference in patient‐reported outcomes at long‐term follow‐up. Arthroscopy 2021;37:3072-8. [Google Scholar] [PubMed]
- 14. Sayampanathan AA, Silva AN, Chye AT. Rotator cuff repairs with and without acromioplasties yield similar clinical outcomes: a meta-analysis and systematic review. Arthroscopy 2021;37:1950-7. [Google Scholar] [PubMed]
- 15. Maguire JA, Dhillon J, Scillia AJ, Kraeutler MJ. Rotator cuff repair with or without acromioplasty: A systematic review of randomized controlled trials with outcomes based on acromial type. Am J Sports Med 2024;52:3404-11. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Humeral Avulsion of Glenohumeral Ligament Lesion – A Case Report and Surgical Considerations
July 1, 2026 Humeral Avulsion of Glenohumeral Ligament Lesion – A Case Report and Surgical Considerations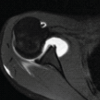 April 1, 2026 Rare Presentation of Chronic Anterior Instability with Concomitant Triad of Anterior Labral Periosteal Sleeve Avulsion, Hill–Sachs, and Humeral Avulsion of the Glenohumeral Ligament Lesions: A Case Report
April 1, 2026 Rare Presentation of Chronic Anterior Instability with Concomitant Triad of Anterior Labral Periosteal Sleeve Avulsion, Hill–Sachs, and Humeral Avulsion of the Glenohumeral Ligament Lesions: A Case Report November 1, 2025 Functional Outcome of Arthroscopic Single-row Rotator Cuff Repair Using the PENN Shoulder Score – A Prospective Cohort Study
November 1, 2025 Functional Outcome of Arthroscopic Single-row Rotator Cuff Repair Using the PENN Shoulder Score – A Prospective Cohort Study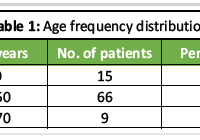 September 1, 2025 Clinical and Functional Outcomes of Proximal Humerus Internal Locking System Plate Fixation in Proximal Humerus Fractures: A Short-term Follow-up
September 1, 2025 Clinical and Functional Outcomes of Proximal Humerus Internal Locking System Plate Fixation in Proximal Humerus Fractures: A Short-term Follow-up