
The study highlights that the direct anterior approach (DAA) for total hip arthroplasty (THA) in patients with avascular necrosis (AVN) is a safe and effective procedure, demonstrating low complication rates and significant improvements in functional outcomes. These insights are particularly relevant in the context of managing AVN-related hip pathologies in low- and middle-income countries.
Dr. Supreet Bajwa, Wockhardt Hospital, 1877, Dr. Anandrao Nair Marg, Near Agripada, Mumbai Central, Maharashtra, India. E-mail: supreetbajwa90@gmail.com
Abstract
Purpose: Early complications following direct anterior approach (DAA) total hip arthroplasty (THA) in avascular necrosis (AVN) pose challenges due to altered bone quality and anatomical variations. This study evaluates early complications, functional outcomes, and management strategies in 250 DAA THA cases at a resource-limited centre.
Materials and Methods: A retrospective analysis was conducted on patients (18–65 years) who underwent DAA THA for AVN between January 2022 and December 2023. Exclusion criteria included prior hip surgeries, congenital deformities, and significant comorbidities. The surgical protocol focused on minimal tissue disruption and precise implant placement, aided by intraoperative fluoroscopy. Data on demographics, surgical details, complications, and functional outcomes (Harris hip score [HHS] and Western Ontario and McMaster Universities Osteoarthritis Index [WOMAC]) were collected at 2 and 6 weeks and 1 year postoperatively.
Results: The cohort included 197 males (78.8%) and 53 females (21.2%), with a mean age of 41.1 ± 14.4 years. The mean surgical time (incision to closure) was 73.7 ± 20.7 min/hip. Early complications occurred in 5.6% of cases: dislocation (0.4%), superficial infections (1.2%), lateral femoral cutaneous nerve injuries (3.2%), and limb length discrepancies (0.8%), all of which were successfully managed. Functional outcomes improved significantly, with HHS increasing from baseline 39.98 to 96.8 and WOMAC scores decreasing from baseline 58.9 to 9.2 in 1 year.
Conclusion: DAA THA is a safe and effective procedure for AVN, with low complications and significant functional improvement. Surgeon experience, meticulous technique, and standardised protocols optimise outcomes, supporting its viability in resource-constrained settings, though further research is needed.
Keywords: Direct anterior approach, total hip arthroplasty, avascular necrosis, early complications, India
Total hip arthroplasty (THA) is globally acknowledged as a highly effective surgical procedure for addressing advanced hip pathologies, including osteoarthritis and avascular necrosis (AVN) [1]. Among the various surgical approaches, the direct anterior approach (DAA) has gained prominence due to its potential advantages, such as reduced post-operative pain, lower dislocation rates, and accelerated recovery times. These benefits have contributed to its increasing adoption, particularly in Asian countries [2]. However, the implementation of DAA in resource-limited settings poses distinct challenges, where factors such as patient selection, surgical expertise, and post-operative care play pivotal roles in determining outcomes [3]. Early complications associated with DAA THA, including iatrogenic femoral fractures, dislocations, and wound-related issues, are critical to address to optimise patient care and refine surgical techniques [4]. This is especially relevant in the context of AVN, a condition that predominantly affects young and middle-aged individuals and often progresses to femoral head collapse if left untreated [5]. In India, AVN represents a leading indication for THA, accounting for a substantial proportion of procedures, thereby underscoring the need for tailored surgical strategies for this demographic [1]. The aetiology of AVN is multifactorial, involving genetic predisposition; lifestyle factors such as alcohol consumption, corticosteroid use, and traumatic injuries; and, more recently, complications related to COVID-19 [6]. The progressive nature of AVN leads to severe pain, functional impairment, and eventual joint destruction, necessitating timely surgical intervention [7]. While DAA offers potential advantages, its steep learning curve and technical demands can result in complications, particularly during the initial phases of implementation, especially in settings with limited surgical training and infrastructure [8]. Effective management of early complications in DAA THA requires a comprehensive understanding of patient-specific factors, surgical techniques, and post-operative protocols. Previous studies have highlighted the importance of surgeon experience, meticulous patient selection, and refined surgical techniques in minimising complications [3,9]. However, there is a notable gap in the literature regarding outcomes of DAA THA in low- and middle-income countries, particularly in the context of AVN [3]. This highlights the need for region-specific studies to address the unique challenges and opportunities presented by DAA. The aim of this study was to evaluate the incidence, pattern, and management of early complications following DAA THA in a consecutive cohort of patients with AVN in an Indian tertiary care setting and to assess associated early functional recovery using standardised outcome measures.
Study design:
This retrospective study was conducted at a tertiary care centre in India, analysing 250 cases of DAA THA performed for AVN between January 2022 and December 2023. Patient data were collected from electronic medical records, including operative reports and follow-up assessments. Since this was a retrospective analysis, no direct patient contact occurred; ethical approval was waived by the Institutional Review Board, while written informed consent was obtained preoperatively for the use of anonymised clinical data in research. The study adhered to the principles outlined in the Declaration of Helsinki, ensuring patient confidentiality and data integrity.
Patient selection:
Patients were identified through a retrospective review of hospital records based on predefined eligibility criteria. A total of 250 consecutive patients who met the inclusion criteria were selected. Inclusion criteria included a documented diagnosis of AVN based on clinical evaluation and imaging (magnetic resonance imaging or radiographs) and an age between 18 and 65 years at the time of surgery. Exclusion criteria were patients with a history of previous hip surgeries recorded in the medical database; presence of congenital hip deformities documented in pre-operative assessments; and significant comorbidities contraindicating THA, including advanced cardiovascular disease, uncontrolled diabetes, or severe renal dysfunction, as noted in pre-operative evaluations.
Surgical technique:
All primary THA during the study period were performed via the DAA procedure, as it represents the standard surgical approach routinely practised at our institution, ensuring procedural consistency and uniform perioperative protocols. All surgeries were performed by a single surgeon, experienced in DAA protocol. The technique emphasised minimal soft-tissue disruption and precise implant positioning. Spinal or epidural anaesthesia was uniformly administered, with no regional blocks used. Patients were positioned supine on a specialised fracture table, an Innovative Orthopaedic Technologies (IOT) purist (IOT Orthopaedics, Switzerland) equipped with a leg position traction system. Intra-articular pericapsular injections of local anaesthetics (ropivacaine or bupivacaine), ketorolac, and epinephrine were administered, with dosages tailored to individual body weight by the anaesthesiologist. A single pre-operative dose of antimicrobial prophylaxis was administered. Intraoperative fluoroscopy was utilised to ensure accurate placement of the femoral stem and acetabular cup, assess hip offset, and verify leg length. Implant selection and fixation methods were determined by the surgeon’s preference and patient-specific factors [8].
Data collection:
Demographic data, including age, gender, and body mass index (BMI), were obtained along with surgical details, immediate post-operative complications, and functional outcomes. Complications such as dislocation, infection, nerve injury, and leg length discrepancies (LLD) were systematically documented.
Outcome measures:
Functional outcomes were assessed using the Harris Hip Score (HHS) and the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC). Evaluations were conducted preoperatively, immediately postoperatively, and at 2 weeks, 6 weeks, and 1 year post-surgery.
Patient demographics and surgical details:
A retrospective analysis of 250 patients who underwent DAA THA for AVN was conducted. The most common aetiologies of AVN in this cohort were post-COVID-related AVN (44.8%), idiopathic causes (27.6%), and chronic alcohol or steroid use (27.6%) (Table 1).
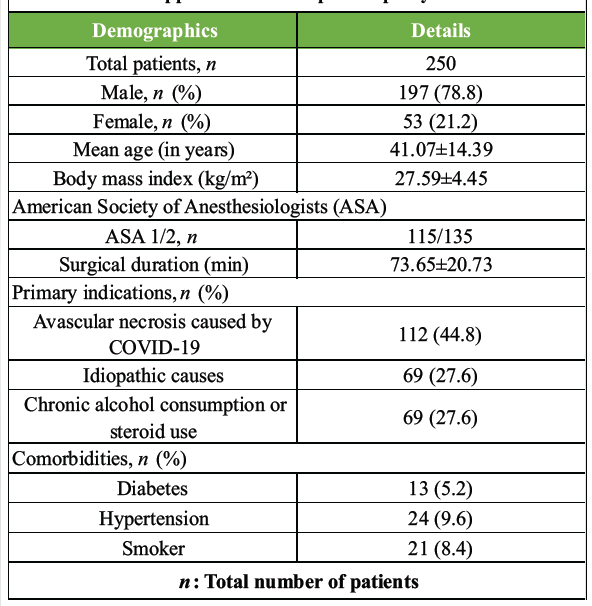
Table 1: Demographic details of patients undergoing Direct anterior approach for total hip arthroplasty.
The cohort comprised 197 males (78.8%) and 53 females (21.2%) (Fig. 1), with a mean age of 41.1 ± 14.4 years, ranging from 18 to 65 years, representing a diverse demographic profile.
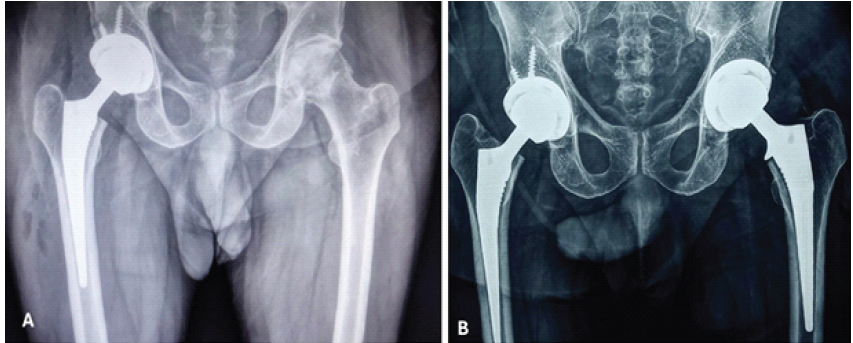
Figure 1: Post-operative anteroposterior pelvic radiographs (a) of a patient with limb length discrepancy following right total hip arthroplasty using an uncemented, collarless femoral stem and acetabular cup. The contralateral (left) hip remains native and shows degenerative changes. Follow-up X-ray at 6 weeks after completion of staged bilateral total hip arthroplasty (b). The left hip has now been replaced using a collared uncemented femoral stem. Both implants appear well-positioned with restored hip biomechanics and limb length symmetry.
The mean BMI of the participants was 27.6 ± 4.5 kg/m2. The mean surgical duration (incision-to-closure) was 73.7 ± 20.7 min/hip, with a range from 39 to 110 min/hip, reflecting the variability and complexity of individual cases (Table 1).
Immediate post-operative outcomes:
All patients were mobilised within 24 h postoperatively, with the majority achieving independent ambulation by the 2-week follow-up. Early complication rates were observed in 5.6% of patients, encompassing one case of dislocation, three superficial infections (1.2%), and eight instances of lateral femoral cutaneous nerve (LFCN) issues (3.2%). In addition, LLD was observed in two patients (0.8%) (Table 2).
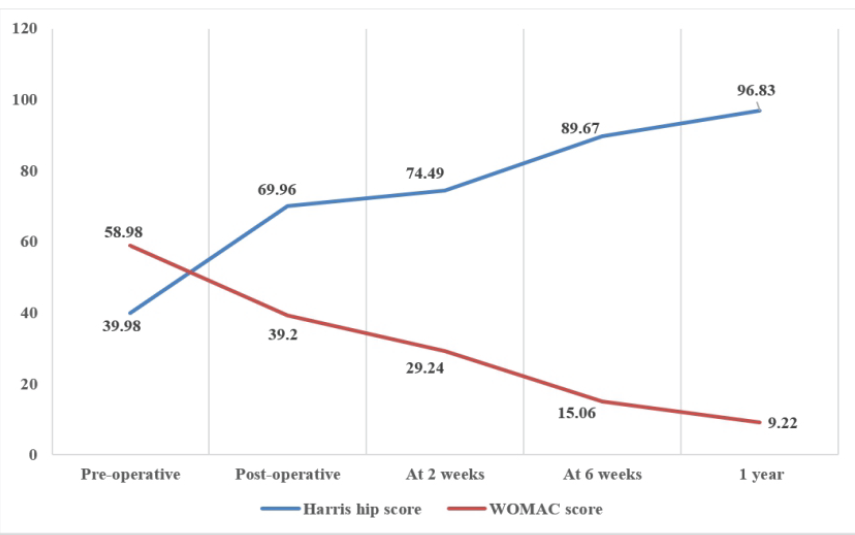
Figure 2: Functional outcomes of patients undergoing direct anterior approach for total hip arthroplasty using the Harris Hip Score and Western Ontario and McMaster Universities Osteoarthritis Index scores.
The dislocation was successfully managed with closed reduction under general anaesthesia, whereas the superficial infections were effectively treated with antibiotic therapy. Intraoperative fluoroscopy was utilised to ensure accurate implant positioning (Fig. 1), with no reported cases of malalignment.
Functional outcomes:
Significant improvements in functional outcomes were observed in all patients following DAA THA, as evaluated using the HHS and the WOMAC score. Pre-operative HHS scores averaged 39.9 ± 6.1, indicating significant hip dysfunction. Immediate post-operative HHS scores improved to an average of 69.9 ± 5.6 (P < 0.0001), demonstrating early functional recovery. Progressive improvement was observed at subsequent follow-ups, with mean HHS scores reaching 74.5 ± 5.6 at 2 weeks, 89.7 ± 2.8 at 6 weeks, and 96.8 ± 1.5 at 1-year post-surgery (Fig. 2). Similarly, WOMAC scores, which averaged 58.9 ± 5.7 preoperatively, showed a marked decline to 39.2 ± 5.7 immediately postoperatively, further decreasing to 29.2 ± 5.7 at 2 weeks, 15.1 ± 3.3 at 6 weeks, and 9.2 ± 3.6 at 1 year (P < 0.0001) (Fig. 2). The consistent and significant decrease in WOMAC scores highlights a progressive reduction in pain and functional limitations.
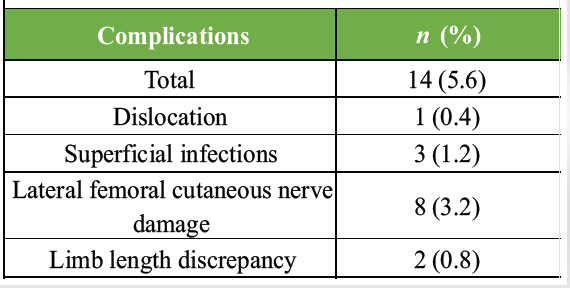
Table 2: Early post-operative complication rates in the direct anterior approach for total hip arthroplasty
The management of early complications following DAA THA in patients with AVN of the femoral head presents unique challenges, particularly in resource-limited healthcare systems such as India. This study, based on a series of 250 AVN cases treated with DAA THA, provides valuable insights into early complications and mitigation strategies. As the adoption of minimally invasive surgical techniques continues to expand globally, studies are essential to ensure that the benefits of these approaches are realised across diverse patient populations and healthcare systems. The findings contribute to the growing literature on DAA THA, particularly in the context of AVN, and offer practical recommendations for surgeons operating in similar settings. The overall complication rate observed in our study was 5.6%, which falls within acceptable limits as per the international standards. A recent study reported a cumulative incidence of major surgical complications of 6.9%, with a 1-year revision rate of 0.1% [10]. Apart from a single patient who suffered from a dislocated hip, no major complications requiring admission were noted in any of our patients. Variability in early complication rates for DAA THA has been documented across different studies. For instance, a retrospective analysis involving 91 patients reported a complication rate of 15.4% [9], whereas a larger series of 525 THA cases documented a total complication rate of 15% [11]. In addition, community-based orthopaedic surgeons adopting the DAA without formal residency or fellowship training have reported short-term major complication rates as high as 9% [12]. These discrepancies highlight the importance of surgical expertise, perioperative protocols, and institutional resources in optimising patient outcomes. Our findings noted a total complication rate of 5.6% with no component revisions at 1 year. The implementation of proactive management strategies, such as enhanced recovery after surgery protocols and immediate post-operative care adjustments, along with the surgeon’s expertise, may have played a critical role in minimising the complication rates falling within this acceptable range.
Incidence of nerve damage:
The LFCN is a purely sensory nerve, and injury to this structure typically presents as numbness, paraesthesia, or, in severe cases, painful neuroma in the anterolateral thigh, resembling meralgia paresthetica [9]. Although LFCN injury does not result in functional deficits, it can significantly impair patients’ quality of life due to persistent sensory disturbances [13,14]. In our study, the incidence of LFCN injury following DAA THA was significantly lower (3.2%), with half of the affected patients achieving complete recovery within 3 months. This contrasts with the widely reported incidence rates ranging from 12% to 81% in other studies [12,13]. LFCN injury may result from various factors, including direct transection by a surgical blade, excessive stretching due to retractor placement, compression by surgical instruments, or entrapment within scar tissue formation [14]. To mitigate this risk, the fascia should be incised 1 cm lateral to the intermuscular plane to safeguard the nerve branches [14]. A thorough understanding of the LFCN’s anatomical course and its variations is essential. Comparative studies have highlighted considerable variability in LFCN injury rates. For instance, Goulding et al. reported LFCN injury in 81% of patients, with persistent symptoms at a mean follow-up of 13.4 months [15], whereas Homma et al. documented a 31.9% incidence, with 32% of cases demonstrating spontaneous recovery over an average of 6.4 months [14]. In a retrospective study of 91 patients, LFCN complications were reported in three patients (3.3%), with transient paraesthesia resolving within 3 months in two cases and persistent numbness in one case, without functional limitations due to the purely sensory nature of the LFCN [9]. Similarly, a study comparing the DAA with the posterolateral approach in 133 patients observed a 3.13% incidence of LFCN complications [16]. In a randomised controlled trial comparing bikini-incision DAA with the posterolateral approach in 106 patients, a 12% incidence of LFCN dysesthesia was reported, with five patients experiencing numbness persisting until 1-year follow-up [17]. In contrast, our study observed a significantly lower incidence of 3.2%, with half of the affected patients achieving complete recovery within 3 months without any intervention. The other two patients had persistent sensory loss around the surgical scar, which also needed no additional intervention. Preventive measures, such as meticulous skin-fascia incision, careful subcutaneous dissection, and avoidance of excessive retraction between the sartorius and tensor fascia lata muscles, are critical to minimising the risk of LFCN injury [9]. For patients presenting with a painful neuroma, conservative medications such as gabapentinoids can be prescribed. If unsuccessful, radiofrequency ablation of the LCFN can be performed under ultrasonographic guidance.
Leg length discrepancy (LLD):
Leg length discrepancy is a well-documented complication following THA, with reported incidence rates ranging from 1% to 27% and discrepancies between 3 and 70 mm [18]. While most patients tolerate LLD up to 10 mm, larger discrepancies can lead to dissatisfaction [18,19]. THA more often results in limb lengthening rather than shortening, with ≥1 cm LLD in up to 50% of cases [18]. However, only 15–20% of these cases require corrective interventions, such as shoe lifts [18]. For discrepancies ranging from 2 to 5 cm, conservative management with shoe lifts or insoles is typically employed [20]. The primary limitation of insole-based LLD correction is the available shoe volume. Heel wedge insoles can compensate for up to 2 cm of discrepancy, while closed shoes incorporating a sole lift can correct differences up to 5 cm. However, when the discrepancies exceed 5 cm, more invasive interventions, such as intramedullary lengthening nails, may be necessary, as shoe lifts ≥5 cm can lead to instability [20]. Comparative studies have highlighted the superiority of the DAA in minimising LLD. For instance, a study of 121 patients reported LLD in 8% of DAA cases versus 28% in the anterolateral approach (ALA) group, with no DAA patient exhibiting LLD >1.5 cm [21]. A meta-analysis further supported these findings, revealing LLD >10 mm in 1.2% of DAA cases, compared to 3.7% for the posterior approach (PA) and 11.4% for ALA [20]. In our study, LLD due to stem subsidence occurred in two patients (0.8%), a rate lower than previously documented incidences. Neither patient required any further intervention as the stems stabilised after the initial check. Both underwent a staged THA on the opposite side, and the LLD was subsequently corrected. To minimise the risk of LLD, intraoperative fluoroscopy has been shown to significantly enhance leg length control, particularly in the supine position, which allows for more precise radiographic and clinical assessments during surgery [22]. A retrospective study measured LLD using a single intraoperative fluoroscopic image and reported an LLD of 2.4 ± 2.1 mm, with 1.2% of patients exhibiting LLD >10 mm [23]. Similarly, another retrospective study comparing the DAA and posterolateral approaches revealed a statistically significant reduction in LLD within the DAA group, with a median LLD of 0 mm (range: −5–4.5 mm) compared to 5 mm (range: 0–9 mm) in the posterolateral group [22]. While traditional methods (e.g., pins, callipers, rulers) have been used for intraoperative LLD correction, their accuracy remains underreported. However, meticulous planning and application of these techniques can reduce post-operative discrepancies, with studies reporting mean LLDs of 1–4.2 mm. Despite this, residual LLD persists in up to 13% of patients, with deviations ranging from 2.6 to 10 mm [18]. Advanced techniques such as tissue tension evaluation, transosseous pin measurements, pre-operative 2D/3D planning, and computer-assisted navigation have further improved the accuracy of LLD management [19]. A study demonstrated that 3D pre-operative planning offered higher accuracy compared to 2D templating in terms of implant size, positioning, and LLD prevention [19]. These advancements, combined with DAA and intraoperative fluoroscopy, not only reduce the incidence of post-operative LLD but also contribute to better functional outcomes and higher patient satisfaction by ensuring optimal limb alignment and stability. Our findings, along with these studies, reiterate that the DAA, when combined with intraoperative fluoroscopy and advanced planning techniques, significantly reduces the incidence of LLD.
Management of dislocations and infections:
Dislocation and infection are among the most prevalent early post-operative complications following THA, with dislocations often resulting from low-energy trauma [4]. Reported dislocation rates for the anterior approach range from 0.6% to 1.5% [4]. Comparative studies have consistently demonstrated lower dislocation rates with the DAA compared to other approaches. For instance, one study found a dislocation rate of 1.1% for the PA versus 0.7% for the DAA [24], whereas another reported no dislocation for DAA THAs compared to 4% for PA THA [25]. Our study observed a dislocation rate of 0.4%, with no revisions. The single dislocation event occurred following high-intensity trauma and was successfully managed with closed reduction without any further episodes of dislocation or need for component revisions. In case of anterior dislocation, the authors advocate immediate closed reduction if within 6 weeks of surgery, provided the components, especially the acetabular shell, are not in excessive anteversion. If excessively anteverted, component exchange or application of a lipped liner or a constrained polyethylene liner can be attempted to salvage the hip. Although dislocation in our study was observed within the 1st post-operative year, late-onset occurrences remain a potential long-term complication. Patients undergoing THA, irrespective of surgical approach, should be counselled that the risk of prosthetic dislocation remains beyond the immediate post-operative period. Structured patient education regarding prolonged dislocation risk can help minimise this complication by promoting adherence to activity modifications and avoidance of high-risk positions that predispose to hip instability [24]. The reduced dislocation rate associated with the DAA may be attributed to its muscle-preserving nature, which enhances dynamic stabilisation of the hip joint [25]. Conversely, the DAA THA is associated with higher reoperation risks due to wound complications, such as haematomas, delayed healing, and infections [4]. Comparative studies indicate higher rates of prolonged wound drainage, superficial infections, and deep infections with DAA relative to the direct lateral approach [26], though some reports note no minor wound complications in DAA cases compared to an 11% rate in mini-posterior THA [27]. Obesity further amplifies these risks, contributing to delayed healing, surgical site infections, and increased reoperation rates [3]. In our cohort, superficial wound infections occurred in 1.2% of cases, all of which were managed successfully with dressings and oral antibiotics, with no instances of deep infection reported.
Functional outcomes:
Early functional outcomes following the DAA for THA, compared to other surgical approaches, have been extensively studied. In a prospective randomised controlled trial comparing the DAA and the posterolateral approach for THA, the DAA group exhibited a tendency toward higher HHS than the posterolateral approach group up to 3 months postoperatively [17]. Similarly, the WOMAC scores indicated that the DAA group maintained superior outcomes relative to the posterolateral approach group during the first 3 months following surgery. A meta-analysis comparing HHS outcomes between the DAA and conventional approaches reported that the HHS at 1 year postoperatively ranged from 92 to 97 across randomised controlled trials, with no significant differences observed between the DAA and conventional approaches [28]. Similarly, a single-centre study demonstrated significant functional improvement following THA via the DAA, with the mean HHS increasing from 33.2 ± 2.5 preoperatively to 93.9 ± 2.1 at the 1-year follow-up [3]. These findings highlight the consistent and substantial functional recovery achievable with the DAA. Our study findings align with these results [3,28], demonstrating a significant improvement in functional outcomes following THA via the DAA. The increased HHS at 1-year follow-up indicates near-complete restoration of hip function, whereas the decreased WOMAC scores reflect substantial improvements in pain, stiffness, and functional limitations. These outcomes underscore the efficacy of the DAA in achieving excellent early- and mid-term functional results, consistent with the literature.
Limitations:
Despite its strengths, this study has several limitations. The retrospective design inherently introduces selection bias and limits the ability to establish causal relationships. The absence of a control group comparing DAA with other approaches restricts the generalisability of findings. In addition, reliance on electronic medical records may lead to underreporting of complications, particularly those that resolved spontaneously without formal documentation. Another limitation is the relatively short follow-up duration of 1 year, which precludes assessment of long-term survivorship and implant-related complications. Nonetheless, this study has several strengths. The large sample size of 250 patients provides robust data on clinical and functional outcomes. The standardised surgical protocol followed by an experienced orthopaedic surgeon ensures consistency in technique and perioperative care. The use of validated functional outcome measures (HHS and WOMAC) at multiple post-operative intervals strengthens the reliability of functional assessments. Furthermore, the incorporation of intraoperative fluoroscopy and structured complication documentation enhances the accuracy of surgical outcome evaluation. These methodological strengths make the findings relevant for orthopaedic surgeons considering DAA THA, particularly in an Indian clinical setting.
Future directions:
Future studies should focus on prospective, comparative analyses between DAA and other surgical approaches, such as the posterolateral and ALAs, to further validate the superiority of DAA in AVN patients. Longer-term follow-up studies are warranted to assess implant survival rates, long-term functional outcomes, and potential late complications such as aseptic loosening and periprosthetic fractures. In addition, research on the impact of patient-specific factors, such as obesity, muscle strength, and pre-operative functional status, on surgical outcomes could provide further insights into optimising patient selection criteria. The role of advanced intraoperative technologies, including robotic-assisted navigation and 3D preoperative planning, in further improving implant positioning and reducing complications should also be explored. Finally, studies evaluating the cost-effectiveness of DAA in comparison to other approaches will be essential in guiding healthcare policy and resource allocation, particularly in emerging economies such as India.
This retrospective study focusing on managing early complications in DAA THA patients suffering from AVN in an Indian diaspora demonstrates that the approach offers excellent early functional recovery with a low complication profile. The findings reinforce the advantages of the DAA, including early mobilisation, reduced rates of LLD, and lower incidence of dislocations compared to conventional approaches. The overall complication rate of 5.6% is well within international standards, emphasising the role of standardised surgical techniques, intraoperative fluoroscopy, and enhanced perioperative management strategies in optimising patient outcomes. Moreover, significant improvements in HHS and WOMAC scores at all follow-up intervals underscore the long-term functional benefits of DAA THA. By systematically analysing complications such as LFCN injury, LLD, and superficial infections, this study provides valuable insights into effective mitigation strategies. These findings contribute to the growing body of evidence supporting the safety and efficacy of DAA THA, particularly in resource-limited settings.
This study demonstrates that the direct anterior approach (DAA) for total hip arthroplasty (THA) in patients with avascular necrosis (AVN) is a safe and effective technique, even in resource-limited settings. With a low complication rate (5.6%) and substantial improvement in functional outcomes (Harris hip score from 39.98 to 96.8), this study highlights the critical role of surgeon expertise, meticulous surgical technique, and standardised intraoperative protocols, including the use of fluoroscopy, in achieving optimal outcomes. The findings support the viability of DAA THA for AVN patients, particularly in low- and middle-income countries, offering a practical approach to improving post-operative recovery and quality of life.
References
- 1. Yakkanti RR, Haziza S, Wasserman NA, Annapareddy A, Ratnakar V, Karri SR, et al. Relative frequency of avascular necrosis of the hip as an indication for primary total hip arthroplasty in the USA vs. India. J Orthop 2022;36:1-6. [Google Scholar] [PubMed]
- 2. Rhatomy S, Rasyid FA, Phatama KY. The direct anterior approach in total hip arthroplasty: Publication trends of Asian countries on PubMed. Ann Med Surg (Lond) 2020;55:280-6. [Google Scholar] [PubMed]
- 3. Malhotra R, Batra S, Manhas V, George J, Biju A, Gautam D. Direct anterior approach in total hip arthroplasty: A single-centre experience. Hip Pelvis 2024;36:196-203. [Google Scholar] [PubMed]
- 4. Tay K, Tang A, Fary C, Patten S, Steele R, De Steiger R. The effect of surgical approach on early complications of total hip arthroplasty. Arthroplasty 2019; 1:5. [Google Scholar] [PubMed]
- 5. Petek D, Hannouche D, Suva D. Osteonecrosis of the femoral head: Pathophysiology and current concepts of treatment. EFORT Open Rev 2019;4:85-97. [Google Scholar] [PubMed]
- 6. Parikh S, Gomez O, Davis T, Lyon Z, Corces A. Avascular necrosis as a sequela of COVID-19: A case series. Cureus 2023;15:e35368. [Google Scholar] [PubMed]
- 7. Lohiya A Jr., Dhaniwala N, Dudhekar U, Goyal S, Patel SK. A comprehensive review of treatment strategies for early avascular necrosis. Cureus 2023;15:e50510. [Google Scholar] [PubMed]
- 8. Bajwa S. Surgical technique of direct anterior approach for primary total hip arthroplasty using a leg positioning traction system. J Ortho Case Rep 2023;13:112-21. [Google Scholar] [PubMed]
- 9. Dall’Oca C, Ceccato A, Cresceri M, Scaglia M, Guglielmini M, Pelizzari G, et al. Facing complications of the direct anterior approach in total hip arthroplasty during the learning curve. Acta Biomed 2020;91:103-9. [Google Scholar] [PubMed]
- 10. Barton KI, Steiner NJ, Boldt KR, Sogbein OA, Tsioros SM, Somerville L, et al. Major complications after total hip arthroplasty with the direct anterior approach at a high-volume Ontario tertiary care centre. Can J Surg 2023;66:E596-601. [Google Scholar] [PubMed]
- 11. Foissey C, Fauvernier M, Fary C, Servien E, Lustig S, Batailler C. Total hip arthroplasty performed by direct anterior approach – Does experience influence the learning curve? SICOT J 2020; 6:15. [Google Scholar] [PubMed]
- 12. Kagan R, Peters CL, Pelt CE, Anderson MB, Gililland JM. Complications and pitfalls of direct anterior approach total hip arthroplasty. Ann Joint 2018;3:37. [Google Scholar] [PubMed]
- 13. Gerry AS, Iturregui JM, Carlson BJ, Hassebrock JD, Christopher ZK, Spangehl MJ, et al. Increased risk of lateral femoral cutaneous nerve injury in patients with previous hip arthroscopy who underwent a direct anterior approach total hip arthroplasty. Arthrosc Sports Med Rehabil 2022;5:e103-8. [Google Scholar] [PubMed]
- 14. Homma Y, Baba T, Sano K, Ochi H, Matsumoto M, Kobayashi H, et al. Lateral femoral cutaneous nerve injury with the direct anterior approach for total hip arthroplasty. Int Orthop 2016;40:1587-93. [Google Scholar] [PubMed]
- 15. Goulding K, Beaulé PE, Kim PR, Fazekas A. Incidence of lateral femoral cutaneous nerve neurapraxia after anterior approach hip arthroplasty. Clin Orthop Relat Res 2010;468:2397-404. [Google Scholar] [PubMed]
- 16. Lu S, Li Y, Chai W, Yang Y, Bi Z, Wang H, et al. Clinical efficacy of the direct anterior approach versus the posterior lateral approach for total hip replacement in middle-aged and elderly patients with femoral neck fracture. Sci Rep 2025;15:5273. [Google Scholar] [PubMed]
- 17. Jin X, Chen G, Chen M, Riaz MN, Wang J, Yang S, et al. Comparison of postoperative outcomes between bikini incision via direct anterior approach and posterolateral approach in simultaneous bilateral total hip arthroplasty: A randomised controlled trial. Sci Rep 2023;13:7023. [Google Scholar] [PubMed]
- 18. Desai AS, Dramis A, Board TN. Leg length discrepancy after total hip arthroplasty: A review of literature. Curr Rev Musculoskelet Med 2013;6:336-41. [Google Scholar] [PubMed]
- 19. Tassinari L, Di Martino A, Brunello M, Rossomando V, Traina F, Faldini C. Leg length discrepancy after total hip arthroplasty performed by direct anterior approach: A systematic review comparing surgical approaches and strategies for prevention. EFORT Open Rev 2024;9:733-44. [Google Scholar] [PubMed]
- 20. Vogt B, Gosheger G, Wirth T, Horn J, Rödl R. Leg length discrepancy – treatment indications and strategies. Dtsch Arztebl Int 2020;117:405-11. [Google Scholar] [PubMed]
- 21. Dunn H, Rohlfing G, Kollmorgen R. A comparison of leg length discrepancy between direct anterior and anterolateral approaches in total hip arthroplasty. Arthroplasty 2020;2:30. [Google Scholar] [PubMed]
- 22. Wu PK, Chang WS, Chen KT, Huang PC, Ho CH, Chien CS, et al. Does the utilisation of fluoroscopy affect the accuracy of prosthesis position in patients undergoing hip replacement surgery via the direct anterior approach compared to the posterolateral approach for an experienced surgeon? A single-centre retrospective study. BMC Musculoskelet Disord 2024;25:816. [Google Scholar] [PubMed]
- 23. Caus S, Reist H, Bernard C, Blankstein M, Nelms N. Reliability of a simple fluoroscopic image to assess leg length discrepancy during direct anterior approach total hip arthroplasty. World J Orthop 2021;12:850-8. [Google Scholar] [PubMed]
- 24. Christensen TH, Egol A, Pope C, Shatkin M, Schwarzkopf R, Davidovitch RI, et al. How does surgical approach affect characteristics of dislocation after primary total hip arthroplasty? J Arthroplasty 2023; 38: 7 Suppl 2:S300-5. [Google Scholar] [PubMed]
- 25. Tsukada S, Wakui M. Lower dislocation rate following total hip arthroplasty via direct anterior approach than via posterior approach: five-year-average follow-up results. Open Orthop J 2015;9:157-62. [Google Scholar] [PubMed]
- 26. Aggarwal VK, Elbuluk A, Dundon J, Herrero C, Hernandez C, Vigdorchik JM, et al. Surgical approach significantly affects the complication rates associated with total hip arthroplasty. Bone Joint J 2019;101-B:646-51. [Google Scholar] [PubMed]
- 27. Poehling-Monaghan KL, Kamath AF, Taunton MJ, Pagnano MW. Direct anterior versus miniposterior THA with the same advanced perioperative protocols: Surprising early clinical results. Clin Orthop Relat Res 2015;473:623-31. [Google Scholar] [PubMed]
- 28. Miller LE, Gondusky JS, Kamath AF, Boettner F, Wright J, Bhattacharyya S. Influence of surgical approach on complication risk in primary total hip arthroplasty. Acta Orthop 2018;89:289-94. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes
May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes March 1, 2026 Day-Care Direct Anterior Total Hip Arthroplasty in Urban India: Patient Education, Apprehensions, and Outcomes
March 1, 2026 Day-Care Direct Anterior Total Hip Arthroplasty in Urban India: Patient Education, Apprehensions, and Outcomes July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach
July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study
June 1, 2026 Functional Outcomes of Total Hip Arthroplasty using Modified Harris Hip Score and Oxford Hip Score: A Prospective Study