
Compared to steroid injection, platelet-rich plasma injection provides greater intermediate to long-term pain relief and good elbow function in lateral epicondylitis, allowing for a quicker recovery and higher quality of life.
Dr. Vejaya Kumar, Department of Orthopaedics, Vinayaka Mission’s Medical College and Hospital, Vinayaka Mission’s Research Foundation (Deemed to be University), Puducherry, India. E-mail: dr.vejay87@gmail.com
Abstract
Introduction: Tennis elbow or lateral epicondylitis is a degenerative condition of the common extensor origin of the lateral humeral epicondyle. This study compared the therapeutic effects of platelet-rich plasma (PRP) and corticosteroid injections for the treatment of lateral epicondylitis.
Materials and Methods: In this prospective, randomised trial, 100 patients with lateral epicondylitis were assigned to either PRP injection (PRPI) (n = 50) or steroid injection (SI) (n = 50). Outcomes were assessed at baseline, 1, 3, 6 months, and 1 year using the patient-rated tennis elbow evaluation (PRTEE) and disabilities of the arm, shoulder and hand (DASH) questionnaires, evaluating pain, function and disability.
Results: The groups’ baseline scores were similar. SI significantly improved PRTEE scores at 1 month, demonstrating superior short-term pain alleviation. At 6 months, however, PRPI showed noticeably improved results, with lower PRTEE and DASH scores signifying better pain reduction and functional recovery. There were no discernible changes between the groups at 3 months or a year. While both treatments had similar results at the last follow-up, PRPI generally demonstrated a trend toward better maintained long-term improvement.
Conclusion: SIs deliver rapid but temporary symptom relief, while platelet-rich plasma injections yield greater sustained improvements at intermediate to long-term follow-up for lateral epicondylitis. For long-term symptom management and functional rehabilitation, PRPI might be a better choice.
Keywords: Tennis elbow, lateral epicondylitis, patient-rated tennis elbow evaluation, disabilities of the arm, shoulder and hand score, platelet-rich plasma, steroid injection.
Tennis elbow, or lateral epicondylitis, is a degenerative condition of the common extensor origin of the lateral humeral epicondyle. It is an incidence in the general population that peaks in the fourth to fifth decade and ranges from 2% to 4% of the general population [1,2]. It is prevalent in those whose jobs necessitate frequent rotating motion of the forearm, such as sports persons, technicians, electricians, household workers, software professionals, and knitters contributing a greater portion. Reduced grip strength, work limitation and outer elbow pain are the main complaints. The term given to the pathology of lateral epicondylitis is “angiofibroblastic degeneration”, which is actually a tendinosis with a fibroblastic and vascular response [3]. Observation, analgesics, activity modification, orthosis, and physiotherapy are the mainstays of non-operative treatment [4]. Other such non-operative therapies included injection of corticosteroid, botulinum toxin, hyaluronic acid with chondroitin sulphate injections, autologous blood injections and platelet-rich plasma (PRP) therapy. However, there is a subset of individuals who require surgical intervention when they do not respond to non-operative therapies or due to recurrences. Injection corticosteroids were frequently used in the past, but their effects were transient and eventually caused tendon degeneration [5,6]. Numerous studies have demonstrated that PRP can alleviate patients’ symptoms over the long term [7,8,9,10]. This study compared the therapeutic effects of PRP and corticosteroid injections for the treatment of lateral epicondylitis.
Study design and setting:
This prospective, randomised, parallel-group clinical study was conducted at the Department of Orthopaedics, Vinayaka Mission’s Medical College and Hospital, Karaikal, India, between April 2023 and April 2024. Ethical committee approval was obtained (Ref: VMMCH/IEC/2023–24/07), and all participants provided written informed consent in accordance with the Declaration of Helsinki.
Study population:
Patients are selected based on our criteria as mentioned.
Inclusion criteria:
- Age between 18 and 70 years
- Unilateral involvement
- Clinical diagnosis of lateral epicondylitis (Local tenderness, Positive Cozen’s test, Reduced grip strength due to painful and restricted wrist extension.
- Failed conservative treatment with analgesics, physiotherapy and braces and symptoms lasting at least 3 months or longer;
- Willingness to participate and provide informed consent.
Exclusion criteria:
- History of elbow-fractures, recent trauma or surgery.
- Radiographic evidence of elbow osteoarthritis
- Rheumatoid arthritis or other systemic inflammatory conditions
- Contraindications to steroid injection (SI) (immunocompromised, Uncontrolled Diabetes Mellitus, Local infection, Poor nutrition and poor skin condition)
- Inability to comply with the study protocol.
Sample size calculation:
Based on the parameters drawn from Gosens et al. [11], a mean difference of 16.8 points (pooled standard deviation ± 23.8) in DASH scores between the PRP and corticosteroid groups at 52 weeks was anticipated. To detect this difference with 90% power and a 5% significance level (two‐sided), a minimum sample size of 42 patients per group was calculated using nMaster 2.0. Accounting for an expected dropout rate of 15%, 50 participants were recruited per group, totalling 100 patients.
Randomisation and allocation:
Participants were randomised into two groups: Group 1- PRP injection (PRPI) (n = 50) and Group 2- SI (n = 50) – using a computer-generated sequence with allocation concealment through sealed envelopes. Due to the nature of interventions, blinding of patients and clinicians was not possible; however, outcome assessments were performed by a blinded independent evaluator. Although the intervention could not be blinded for practical reasons, our study employed blinded outcome assessors, reducing the risk of detection bias and increasing internal validity.
Interventions:
Group 1 – PRP I group:
PRP was prepared using the commercial PRP kit (Sensdermics, Chennai, TN, India) according to the manufacturer’s guidelines. Using a 20 G needle, 16 mL of venous blood collected from the patient’s antecubital vein was transferred into two tubes with anticoagulant acid citrate dextrose (ACD) solution with separator gel (Figs. 1 and 2).
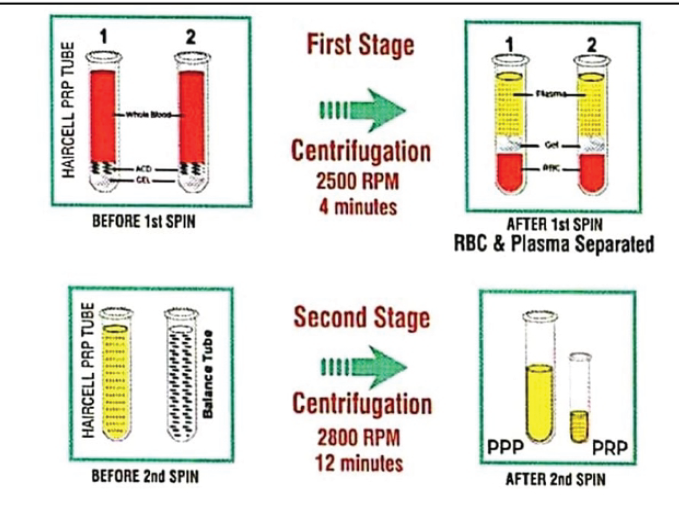
Figure 1: Schematic overview of the steps involved in the platelet-rich plasma preparation.
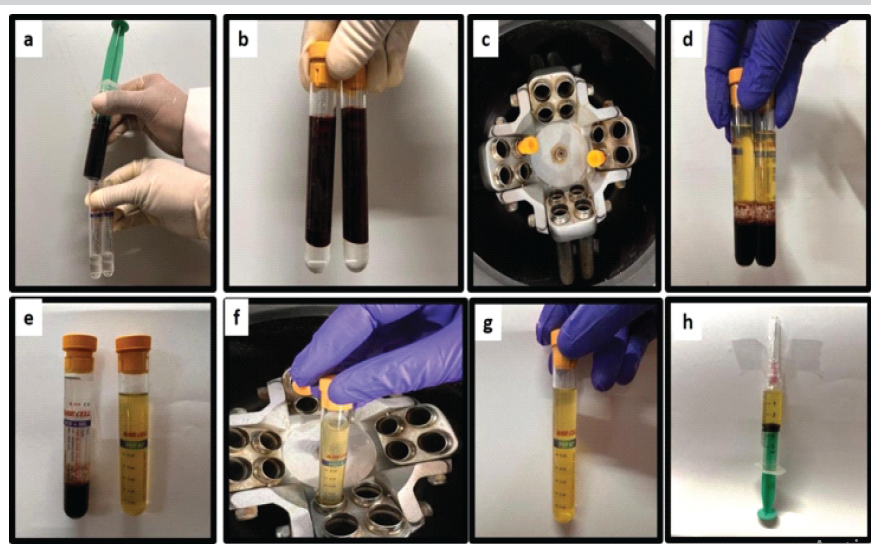
Figure 2: Platelet-rich plasma preparation. (a) 16 mL of blood is collected in a syringe. (b) 8 mL of blood is transferred to each tube. (c) First centrifugation- 2500 rpm for 4 mi. (d) After the first centrifugation, the red blood cells are separated from the supernatant plasma containing platelets by the Gel. (e) Plasma with platelets is collected from those 2 tubes and transferred into a processing tube after the first spin. (f). Second centrifugation – 2800 rpm for 12 min. (g) Plasma after the second spin with a high concentration of platelets at the bottom. (h) Platelet-rich plasma collected in syringe.
Another 2 mL of the venous blood was collected and sent to the hospital laboratory for determination of platelets and leucocyte count. The collected blood in the two disposable separation tubes (ADC-GEL tubes) underwent first-stage centrifugation at 2500 rpm for 4 min at room temperature. Centrifugal force separates the blood components into two distinct layers based on their particular densities. The heaviest particles, the red blood cells, remain in the bottom of the tube; the least dense plasma, along with the platelets, remains at the top, both separated by the gel. Plasma (around 10 mL) from both tubes was transferred to a single PRP processing tube, followed by the second stage centrifugation at 2800 rpm for 12 min along with the balance tube. After the second spin, platelet-poor plasma that remained in the top (6–7 mL) was extracted and discarded. Following this, PRP that remains in the bottom (3–4 mL) was transferred to the PRP collection tube. No activating agent was added to the PRP before administration. Preparation time was about 25 min. The concentration of platelets is checked, and it is usually 4–5 times higher than in whole blood. Under strict aseptic precautions, the maximal tender point was identified by the surgeon’s thumb, and PRP of 2 mL was injected into the most tender point (usually in the tendon sheath of the extensor carpi radialis brevis) (Fig. 3).
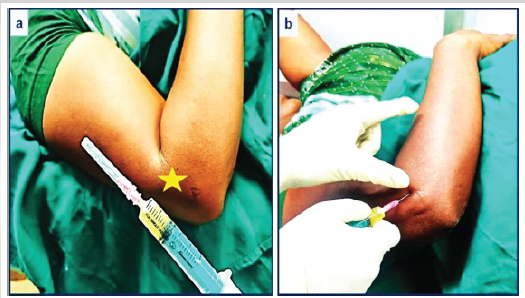
Figure 3: (a and b) Platelet-rich plasma preparation injected in the most tender spot (marked as a yellow star) of the lateral epicondyle under sterile precautions.
Group 2 – SI group:
The steroid group received a single injection (2 mL) of 40 mg Triamcinolone (1 mL) with 2% Lignocaine (1 mL) in the lateral epicondyle at the most tender spot. As there is no generally accepted protocol, we have restricted the use of SI to a single shot because there may be degenerative changes or metabolic side effects of steroid with repeated administration.
Post-injection protocol:
Patients are recommended to reduce the usage of their affected elbow during the next 24 h. Both groups were given weak analgesics like paracetamol only for intolerable pain when needed. Ice was applied post-injection.
Home exercise programme:
Gentle range of motion exercises were initiated by 48 h of injection, based on patient tolerance stretching and strengthening exercises were added gradually. Both groups of participants were engaged in the identical home exercise regimen presented by a physiotherapist. Exercises were performed daily with written/visual instructions, and adherence was tracked using self-reported logs reviewed at follow-ups. We recognise the possibility of reporting bias in self-reported exercise adherence logs. To minimize this bias, we employed concurrent verification through acknowledgement by patient bystanders or family members.
Outcome measures:
Outcomes were assessed at baseline, 1 month, 3 months, 6 months, and 1 year. The primary measures were the patient-rated tennis elbow evaluation (PRTEE) and disabilities of the arm, shoulder and hand (DASH) questionnaires, evaluating pain, function and disability. PRTEE and DASH are widely accepted and validated tools in lateral epicondylitis research.
Statistical analysis:
The Statistical Package for the Social Sciences 23 program was utilised for data analysis. Serial analysis within the groups was conducted using the paired t-test. The groups were compared using the unpaired t-test. Results were considered significant if P < 0.05, and the test was run at a 95% confidence range. The Chi-square test was used to compare two groups’ baseline patterns.
Participant characteristics:
Baseline demographic and clinical characteristics of patients in the PRPI group (n = 50) and SI group (n = 50) were compared (Table 1).
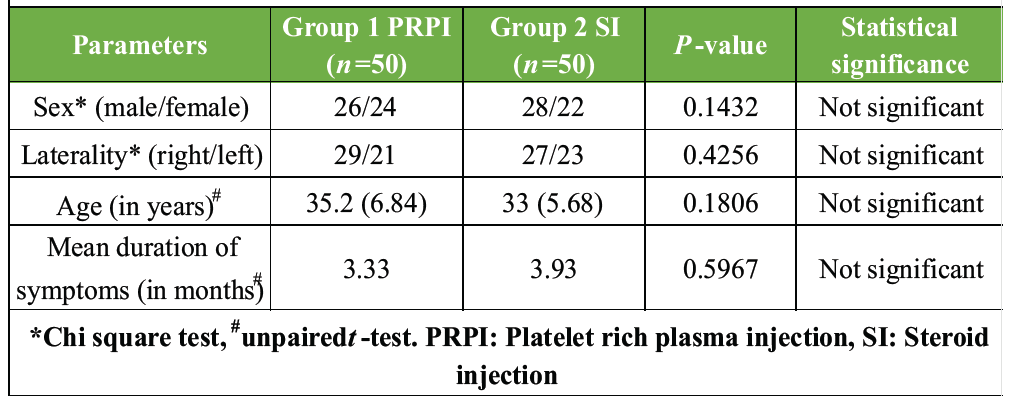
Table 1: Pre-injection sociodemographics features of both groups
There were no statistically significant differences between the groups with respect to sex distribution (male/female: 26/24 vs. 28/22; P = 0.1432), laterality (right/left: 29/21 vs. 27/23; P = 0.4256), mean age (35.2 ± 6.84 vs. 33.0 ± 5.68 years; P = 0.1806), or mean duration of symptoms (3.33 vs. 3.93 months; P = 0.5967). These findings indicate that the two groups were comparable at baseline, minimising the potential influence of demographic and clinical confounders on study outcomes.
PRTEE and DASH scores:
Clinical outcomes were assessed using the PRTEE and DASH scores at baseline, 1 month, 3 months, 6 months, and 1 year following injection. The mean PRTEE scores between the PRPI and SI groups at baseline and during post-injection follow-up were compared (Table 2 and Graph 1).
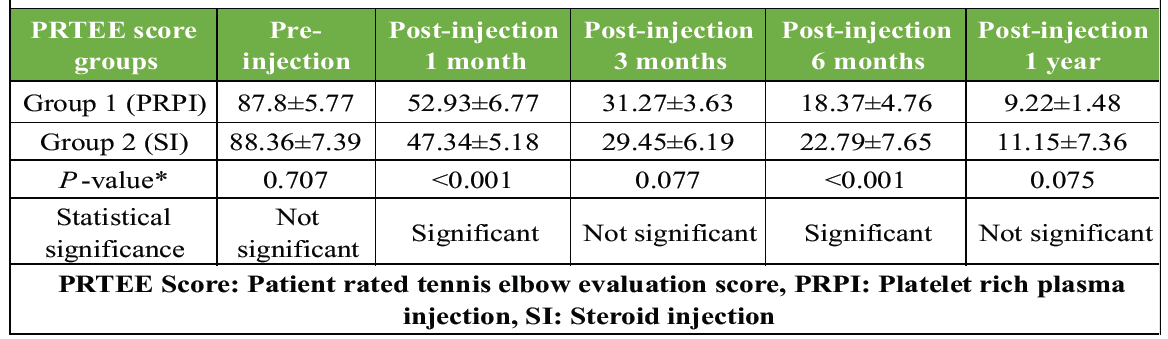
Table 2: Comparison of mean PRTEE scores at pre-injection and post-injection follow-up
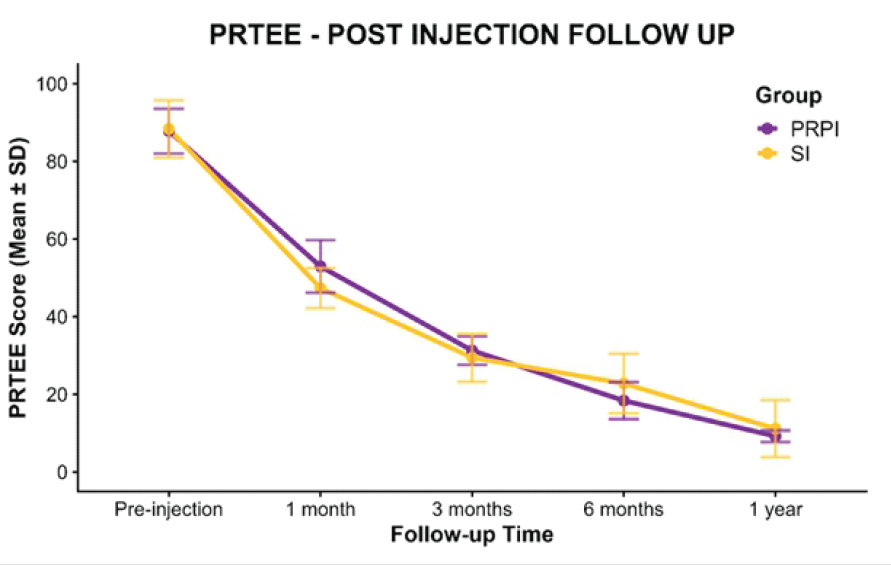
Graph 1: Line graph showing mean patient-rated tennis elbow evaluation scores over time with standard deviation error bars for the platelet-rich plasma injection and steroid injection groups.
Baseline PRTEE scores were comparable between the groups (87.8 ± 5.77 vs. 88.36 ± 7.39; P = 0.707). A statistically significant difference was observed at 1 month, favouring the SI group (47.34 ± 5.18 vs. 52.93 ± 6.77; P < 0.001). At 3 months, the difference between groups was not significant (P = 0.077). At 6 months, the PRPI group demonstrated significantly lower PRTEE scores compared to the SI group (18.37 ± 4.76 vs. 22.79 ± 7.65; P < 0.001). By 1 year, both groups showed sustained improvement with no statistically significant difference between them (P = 0.075). Overall, both treatments resulted in substantial reductions in PRTEE scores over time. Although improvements were observed in both groups, the PRPI group demonstrated slightly greater long-term improvement, particularly at the 6-month and 1-year follow-up assessments. The comparison of mean DASH scores between the PRPI and SI groups is presented in Table 3 and Graph 2.
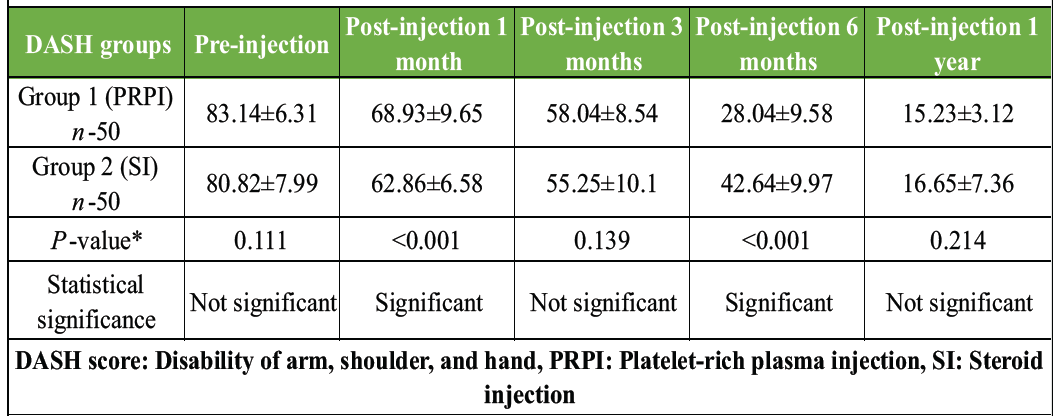
Table 3: Comparison of mean DASH score at pre-injection and post-injection follow-up
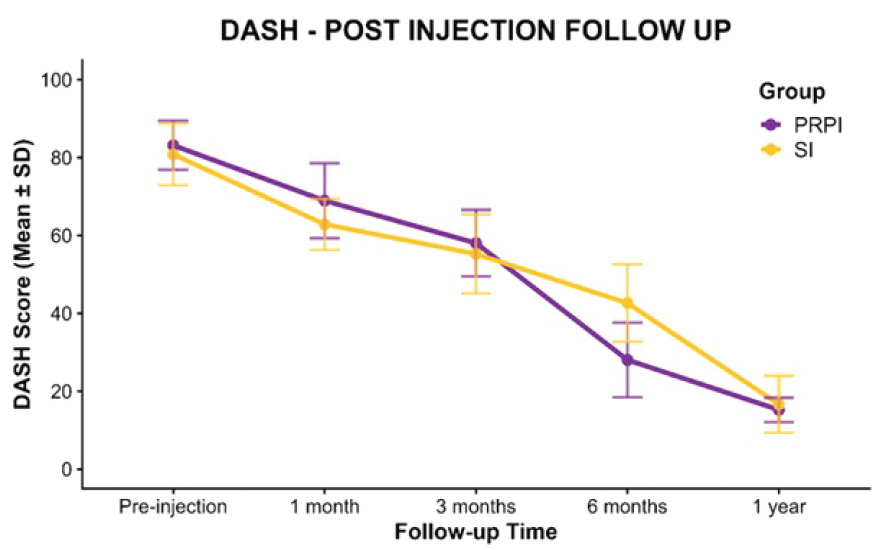
Graph 2: Line graph showing mean disability of arm, shoulder, and hand scores over time with standard deviation error bars for the platelet-rich plasma injection and steroid injection groups.
Both groups showed progressive improvement in DASH scores over time. There was no significant difference between groups at baseline, 3 months, and 1 year follow-up (P = 0.111, 0.139, and 0.214, respectively). However, significant differences were observed at 1 month and 6 months post-injection (P < 0.001), with the PRP group demonstrating lower DASH scores, indicating better functional outcomes compared with the SI group during these periods. At 1-year follow-up, both groups achieved comparable improvements in upper limb function.
Complications:
One patient in the SI group developed a flare-up of symptoms lasting for a few days, which resolved with a course of analgesics and icing. Recurrence of symptoms occurred in three patients during late follow-up, which was treated successfully with PRPI. No other serious complications were observed in our study.
Several studies compare the outcomes of using PRP and steroid treatments for tendinopathy in the lateral epicondyle of the humerus [4,11,12,13,14]. Our study is in accordance with multiple studies like Kivrak and Ulusoy, which have ensured baseline comparability between PRPI and SI groups regarding age, sex distribution, symptom duration, and affected side. This minimises confounding in outcome assessment [15,16]. Similar to our findings, Kemp et al. [17] found SI consistently provides superior short-term pain relief and functional improvement compared to PRPI in lateral epicondylitis. At 1 month: the SI group had significantly lower PRTEE/DASH scores than the PRPI [15,16,17]. But PRPI demonstrates greater efficacy at intermediate (3–6 months) and long-term (≥6 months) follow-up. At 6 months: the PRPI group had significantly lower PRTEE/DASH scores than the SI group [15,16]. By 1 year: Both groups showed sustained improvement with no significant difference; however, some studies, like Gosens et al., report continued superiority of PRPI at longer follow-up [11]. Meta-analyses confirm that while SI is best for short-term relief (<12 weeks), PRPI is superior for intermediate/long-term outcomes [17,18,19]. Both treatments are generally safe: We have reported minor complications with SI (e.g., transient flare-ups), but no serious adverse events were observed [15]. Recurrence rates may be higher with SI; recurrent cases often respond to subsequent PRPI [15]. No significant difference in adverse event rates between groups across studies [20,21]. The evidence robustly supports that SIs offer rapid symptom relief, but their effects diminish over time; platelet-rich plasma injections provide more durable improvements in pain and function at intermediate- to long-term follow-up for conditions like lateral epicondylitis and osteoarthritis [15,16,17]. These findings are consistent across multiple high-quality meta-analyses and systematic reviews [17,18,19]. The safety profile is favourable for both interventions, with rare serious complications. However, the magnitude of long-term functional improvement with PRPI may not always reach minimal clinically important differences for all patients [22]. There is also considerable heterogeneity in study protocols regarding preparation methods for PRP, dosing regimens for steroids, patient selection criteria, and outcome measures used – limiting direct comparability across studies [23]. Our study’s results thus corroborate the increasing amount of data indicating that PRPI delivers long-lasting clinical improvement and reduced recurrence rates, whereas SIs offer quicker symptomatic relief. For individuals with chronic lateral epicondylitis seeking long-term symptom relief and functional improvement, PRPI may therefore be a better course of treatment. While our study demonstrates significant findings on lateral epicondylitis injections, it’s important to note our limitations; it is a single-institution study with a relatively small sample size (n-100) and a lack of ultrasound assessment. Future research could benefit from larger, multicentre studies to further validate these findings.
SIs deliver rapid but temporary symptom relief, while platelet-rich plasma injections yield greater sustained improvements at intermediate to long-term follow-up for lateral epicondylitis. Both modalities are safe when administered appropriately; recurrence is more common after steroids but can be managed effectively with subsequent interventions like PRPI.
Patients with lateral epicondylitis showed improvements in pain and function with both steroid injection and platelet-rich plasma injection (PRPI). While PRPI showed better long-term improvement during follow-up, steroid injection offered better short-term symptom relief. For long-term symptom management and functional rehabilitation, PRPI might be a better choice.
References
- 1. Tosti R, Jennings J, Sewards JM. Lateral epicondylitis of the elbow. Am J Med 2013;126:357.e1-6. [Google Scholar] [PubMed]
- 2. Sanders TL Jr., Kremers HM, Bryan AJ, Ransom JE, Smith J, Morrey BF. The epidemiology and health care burden of tennis elbow: A population-based study. Am J Sports Med 2015;43:1066-71. [Google Scholar] [PubMed]
- 3. Henry M, Stutz C. A unified approach to radial tunnel syndrome and lateral tendinosis. Tech Hand Up Extrem Surg 2006;10:200-5. [Google Scholar] [PubMed]
- 4. Krogh TP, Fredberg U, Stengaard-Pedersen K, Christensen R, Jensen P, Ellingsen T. Treatment of lateral epicondylitis with platelet-rich plasma, glucocorticoid, or saline: A randomized, double-blind, placebo-controlled trial. Am J Sports Med 2013;41:625-35. [Google Scholar] [PubMed]
- 5. Gautam VK, Verma S, Batra S, Bhatnagar N, Arora S. Platelet-rich plasma versus corticosteroid injection for recalcitrant lateral epicondylitis: Clinical and ultrasonographic evaluation. J Orthop Surg (Hong Kong) 2015;23:1-5. [Google Scholar] [PubMed]
- 6. Say F, Gürler D, Inkaya E, Bülbül M. Comparison of platelet-rich plasma and steroid injection in the treatment of plantar fasciitis. Acta Orthop Traumatol Turc 2014;48:667-72. [Google Scholar] [PubMed]
- 7. Creaney L, Wallace A, Curtis M, Connell D. Growth factor-based therapies provide additional benefit beyond physical therapy in resistant elbow tendinopathy: A prospective, single-blind, randomised trial of autologous blood injections versus platelet-rich plasma injections. Br J Sports Med 2011;45:966-71. [Google Scholar] [PubMed]
- 8. Murray DJ, Javed S, Jain N, Kemp S, Watts AC. Platelet-rich-plasma injections in treating lateral epicondylosis: A review of the recent evidence. J Hand Microsurg 2015;7:320-5. [Google Scholar] [PubMed]
- 9. Behera P, Dhillon M, Aggarwal S, Marwaha N, Prakash M. Leukocyte-poor platelet-rich plasma versus bupivacaine for recalcitrant lateral epicondylar tendinopathy. J Orthop Surg (Hong Kong) 2015;23:6-10. [Google Scholar] [PubMed]
- 10. Ahmad Z, Brooks R, Kang SN, Weaver H, Nunney I, Tytherleigh-Strong G, et al. The effect of platelet-rich plasma on clinical outcomes in lateral epicondylitis. Arthroscopy 2013;29:1851-62. [Google Scholar] [PubMed]
- 11. Gosens T, Peerbooms JC, Van Laar W, Den Oudsten BL. Ongoing positive effect of platelet-rich plasma versus corticosteroid injection in lateral epicondylitis: A double-blind randomized controlled trial with 2-year follow-up. Am J Sports Med 2011;39:1200-8. [Google Scholar] [PubMed]
- 12. Peerbooms JC, Sluimer J, Bruijn DJ, Gosens T. Positive effect of an autologous platelet concentrate in lateral epicondylitis in a double-blind randomized controlled trial: Platelet-rich plasma versus corticosteroid injection with a 1-year follow-up. Am J Sports Med 2010;38:255-62. [Google Scholar] [PubMed]
- 13. Coombes BK, Bisset L, Vicenzino B. Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: A systematic review of randomised controlled trials. Lancet 2010;376:1751-67. [Google Scholar] [PubMed]
- 14. Lebiedziński R, Synder M, Buchcic P, Polguj M, Grzegorzewski A, Sibiński M. A randomized study of autologous conditioned plasma and steroid injections in the treatment of lateral epicondylitis. Int Orthop 2015;39:2199-203. [Google Scholar] [PubMed]
- 15. Kıvrak A, Ulusoy I. Comparison of the clinical results of platelet-rich plasma, steroid and autologous blood injections in the treatment of chronic lateral epicondylitis. Healthcare (Basel) 2023;11:767. [Google Scholar] [PubMed]
- 16. Ashwin VY, Krishnan MS, Pandian H, Kumar KV, Sheik M, Dondapati A. Lateral epicondylitis treated with platelet-rich plasma injection and corticosteroid injection. J Orthop Case Rep 2024;14:202-7. [Google Scholar] [PubMed]
- 17. Kemp JL, Olson MA, Tao MA, Burcal CJ. Platelet-rich plasma versus corticosteroid injection for the treatment of lateral epicondylitis: A systematic review of systematic reviews. Int J Sports Phys Ther 2021;16:597-605. [Google Scholar] [PubMed]
- 18. Houck DA, Kraeutler MJ, Thornton LB, McCarty EC, Bravman JT. Treatment of Lateral Epicondylitis With Autologous Blood, Platelet-Rich Plasma, or Corticosteroid Injections: A Systematic Review of Overlapping Meta-analyses. Orthop J Sports Med. 2019 Mar 14;7(3):2325967119831052. doi: 10.1177/2325967119831052. PMID: 30899764; PMCID: PMC6419259. [Google Scholar] [PubMed] [CrossRef]
- 19. 19. Arirachakaran A, Sukthuayat A, Sisayanarane T, Laoratanavoraphong S, Kanchanatawan W, Kongtharvonskul J. Platelet-rich plasma versus autologous blood versus steroid injection in lateral epicondylitis: Systematic review and network meta-analysis. J Orthop Traumatol 2015;17:101-12. [Google Scholar] [PubMed]
- 20. 20. Wang X, Zhang Y. Therapeutic interventions of platelet-rich plasma versus corticosteroid injections for lumbar radicular pain: A systematic review and meta-analysis. J Orthop Surg Res 2025;20:306. [Google Scholar] [PubMed]
- 21. 21. Muthu S, Viswanathan VK, Gangadaran P. Is platelet-rich plasma better than steroids as epidural drug of choice in lumbar disc disease with radiculopathy? Meta-analysis of randomized controlled trials. Exp Biol Med (Maywood) 2025;250:10390. [Google Scholar] [PubMed]
- 22. 22. Maroun R, Daher M, Boufadel P, Lopez R, Khan AZ, Abboud JA. Platelet rich plasma versus corticosteroids for lateral epicondylitis: A meta-analysis of randomized clinical trials. Clin Shoulder Elbow 2025;28:40-8. [Google Scholar] [PubMed]
- 23. 23. Collins T, Alexander D, Barkatali B. Platelet-rich plasma: A narrative review. EFORT Open Rev 2021;6:225-35. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 March 1, 2026 Clinical outcome of Intramedullary Screw Fixation in Metacarpal and Phalangeal Fractures
March 1, 2026 Clinical outcome of Intramedullary Screw Fixation in Metacarpal and Phalangeal Fractures January 1, 2026 Correlation of Serum Vitamin D Levels and Incidence of Lateral Epicondylitis of the Elbow: An Observational Study in Eastern India
January 1, 2026 Correlation of Serum Vitamin D Levels and Incidence of Lateral Epicondylitis of the Elbow: An Observational Study in Eastern India December 1, 2025 Platelet-Rich Plasma Injections are Associated with Higher Resource Utilization and Surgical Escalation Compared with Corticosteroids in Lateral Elbow Tendinopathy
December 1, 2025 Platelet-Rich Plasma Injections are Associated with Higher Resource Utilization and Surgical Escalation Compared with Corticosteroids in Lateral Elbow Tendinopathy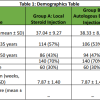 October 1, 2025 Comparison of Efficacy of Autologous Blood Injection versus Steroid Injection in Treatment of Lateral Epicondylitis: A Comparative Study
October 1, 2025 Comparison of Efficacy of Autologous Blood Injection versus Steroid Injection in Treatment of Lateral Epicondylitis: A Comparative Study