
Sprengel's shoulder is a clinical diagnosis, but higher images are mandatory for timely and early surgery to get better outcomes.
Dr. Sitsabesan Chokkalingam, Department of Orthopedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. E-mail: sabesan101@gmail.com
Abstract
Introduction: Sprengel’s deformity (SD) is a rare congenital condition in children characterised by failure of caudal descent, resulting in a high scapula, a cosmetic deformity with functional limitation of the shoulder movements. It is frequently associated with vertebral and other anomalies.
Materials and Methods: A retrospective case series of six children aged <17 years diagnosed with SD over 10 years who presented to our tertiary care referral centre was included in our study. The exclusion criteria were adults with Sprengel and children with syndromic SD due to their different spectrum of possible intervention, timing of surgery, and their outcomes. Clinical assessment using Cavendish and Rigault’s systems and radiological evaluation using plain radiographs, computerised tomographic scans, and magnetic resonance imaging were performed. Surgical management by Woodward’s procedure was undertaken in a 9-year-old case. The outcomes were assessed based on cosmetic improvement, shoulder abduction, and its complications. Current concepts of SD in diagnosis, different radiographic indices, and various surgical options from the systematic review were discussed.
Results: The study included six children aged 2–9 years. Four patients had associated omo-vertebral anomalies, five had congenital spinal anomalies, and three had scoliosis. The Cavendish grade ranged from II to IV. Woodward’s surgical corrective procedure resulted in significant improvement in shoulder abduction and cosmetic appearance. No major neurovascular complications were observed.
Conclusion: Early diagnosis and appropriate surgical intervention in moderate-to-severe SD provide satisfactory cosmetic and functional outcomes. A comprehensive evaluation for associated anomalies is essential for optimal management.
Keywords: Sprengel’s deformity, Cavendish classification, Rigault’s grade, Woodward’s procedure, omo-vertebral bodies, migration index, Broca’s index.
Sprengel’s deformity (SD) is a rare disorder with an incidence rate of 0.3/10,000 live births and a bilateral involvement in 6–16% of cases [1]. The condition was first described in 1891 by the German surgeon Otto Gerhard Karl Sprengel. The congenital elevation of the scapula results from failure of its normal caudal descent in the 9th–12th week of embryonic development. It is frequently associated with a spectrum of congenital anomalies. The scapula is typically dysplastic, with a reduced vertical height and relatively increased horizontal length, often associated with medial rotation and superior displacement. Most cases are sporadic, with no identifiable inheritance pattern. However, SD can be associated with congenital syndromes, most notably Klippel–Feil syndrome, Turner syndrome, Trisomy 18, and DiGeorge syndrome. In children with moderate-to-severe SD, surgical correction has been shown to significantly improve cosmetic appearance and shoulder function. Early diagnosis, including prenatal detection, is essential for timely intervention and optimal outcomes. In this case series, we describe our approach to clinical assessment, radiological evaluation, and management of children with SD. The study highlights current concepts, evidence-based diagnostic strategies, surgical interventions, and clinical outcomes of Woodward’s procedure. Clinical features and grading of SD differ based on age, severity of the deformity, and associated anomalies. Prenatal diagnosis is possible using foetal ultrasonography or magnetic resonance imaging (MRI), with scapular elevation, cervical spine asymmetry, and vertebral arch discontinuity detectable as early as the second trimester [2,3]. In childhood, the spectrum of features includes a high-riding scapula, medial rotational deformity of the scapula, hypoplastic scapula, rib abnormalities, omo-vertebral bone (connecting the scapula to the spine), scoliosis, torticollis, and facial asymmetry with restricted scapulo-thoracic movement. Syndromes associated with SD include Klippel–Feil, with 20–42% cervical vertebral fusions. The rare features in SD include talipes equinovarus, hallux valgus, shortening and limb length discrepancy, congenital dislocation of the hips, hand anomalies, underdeveloped mammary glands, dextrocardia, floating kidney, congenital hernia, anal ectopy, and iniencephaly [4]. The Cavendish classification grades the severity of SD from mild to severe deformity [5]. Post-operative results can be compared, but the functional outcome of shoulder abduction is not included in this grading system. Grade 1 = (very mild) Shoulders are level with no visible deformity when dressed. Grade 2 = (mild) slight prominence of the superomedial aspect of the scapula visible as a neck lump when dressed. <2 cm elevation; Grade 3 = (moderate) shoulder asymmetry 2–5 cm; Grade 4 = (severe) >5 cm scapular elevation with superior scapula near the neck. Rigault’s grading method is based on plain AP radiographs, where the scapular position is correlated with the cervico-thoracic vertebrae [6]. Grade 1: Superomedial angle of scapula between T2 and T4 transverse processes; Grade 2: Scapular superomedial angle between C5 and T2; Grade 3: Superior scapular angle above C5. Diagnostic modalities include plain radiographs of both shoulders in postero-anterior view for scapular elevation (T1-T3 level or above, normally T7) and scapular hypoplasia. Woodward’s oblique view is recommended for Omo-vertebral bodies. The radiographic indices are “Broca’s shoulder index” (Fig. 1a), a ratio of the scapula’s horizontal breadth to its vertical height, which is low in SD and an indicator of scapular dysmorphology (normal range 68–71) [7]. It remains a useful index in children younger than 8 years. The “superior scapular migration index” (Fig. 1b), “rotational deformity index” (Fig. 2a), and altered supra-/subscapular angles (Fig. 2b) can also be monitored and help to assess the progress and outcome of the corrective surgery.
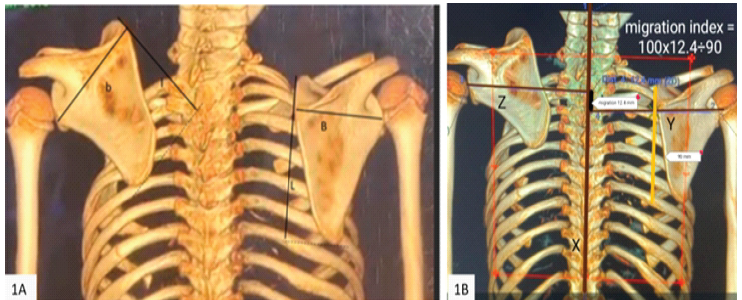
Figure 1: (a) Broca’s scapular index: A ratio of the scapula’s horizontal breadth to its vertical height and an indicator of the extent of scapular dysmorphology. It is calculated by the formula (×100 breadth/length), and on the normal side, it is between 68 and 71. Sprengel’s side shows a lower index due to scapular dysplasia with increased width and reduced height. A useful index in the age before 8 years and complements other grading of the Sprengel’s deformity. (b) Superior scapular migration index: It is the proportionate level of superior migration to the normal vertical height of the scapula. Calculated by (×100 A/B) where X = Midline vertebral axis; Y = Perpendicular line from the center of glenoid to the vertebral axis (normal scapular side); Z = Perpendicular line from the center of glenoid to vertebral axis on (Sprengel’s side); A = Distance between the points where the perpendicular lines intersect the vertical axis; B = Vertical height of the normal scapula.
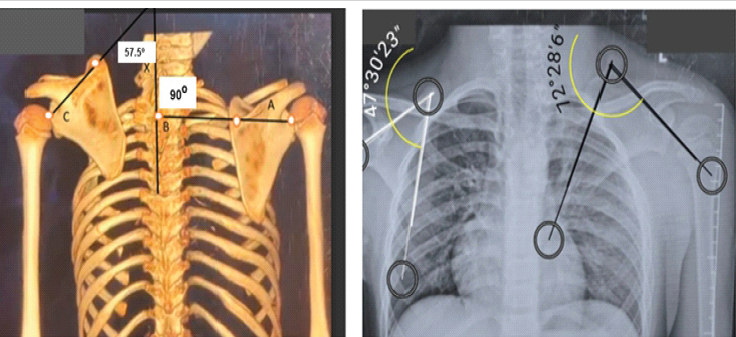
Figure 2: (a) Rotational deformity index: to calculate the degree of scapular superomedial rotation. Angles < asset-backed securities index (ABX) divided by < credit default swap index (CDX); where X = Central vertebral axis (VA); Line AB = Center of glenoid on the normal side through spinous process base to VA; Line CD = Center of glenoid on the Sprengel’s side through spinous process base to VA; Angle < ABX is on the normal side (57.5°) and angle < CDX on the Sprengel’s side (90°). (b): Supra spinous angle and subscapular angles: It is an acute angle connecting the scapular axis formed by the line connecting (superior to the inferior angle of scapula) and the horizontal line through the superior border of the supraspinous fossa. Similar to this, the subscapular angle is measured relative to the subscapular fossa’s inferior margin. Normal value range for these is 30–50°, and on Sprengel’s side, it exceeds 50° due to the tilt and the rotation of the scapula.
A computed tomographic (CT) scan will be a better tool to assess the superior migration and rotation of the dysplastic scapula. The 3D reconstruction measures the “Sprengel’s curve concept”, explaining the inverse relation between rotation and superior displacement (Chol et al. [8]), where the migration appears lesser when the rotation is severe. An MRI scan remains the gold standard to detect associated spinal column anomalies and for the detection of the omovertebral fibrous bands. The “Ra’s eye sign” describes the omo-vertebral body surrounded by fat on the MR scan [9]. A lateral position in the MR scanner with the affected side up is recommended to view the entire stretch of the Omo-vertebral body (OB), and sedated MRI may be warranted in smaller children for better artefact suppression. The prenatal ultrasound in combination with MRI helps in the diagnosis of SD with the elevated scapula, omo-vertebral bone, and associated anomalies [10]. Indications for termination under the Pregnancy Act, when sought, need to have the differentiation of isolated from syndromic SD associated with Klippel–Feil syndrome (KFS), scoliosis, spinal neural tube disorders, and tethered cord [11]. Hence, a prenatal MRI should be considered the gold standard investigation of choice. Differential diagnosis includes birth-related nerve palsy to the serratus anterior, trapezius, and rhomboids, which produce medial or lateral winging and scapular dyskinesia. Moro reflex on the affected side with Horner’s syndrome or phrenic nerve palsy will be seen in extensive brachial plexus palsy [12]. KFS is an autosomal dominant or recessive inherited [13] disorder due to mutations in the GDF6, GDF3, and MEOX1 genes, which includes a triad of a short webbed neck, low hairline, and restricted neck movements. Children with KFS have a spectrum of other anomalies, inclusive of SD of shoulder in 50% of cases and congenital scoliosis in 50% of cases. Atlanto-axial instability in 50%, renal disease in 30%, deafness in 30% of cases, cardiovascular anomalies in 4–14%, and renal disorders and metabolic disorders inclusive of rickets, scapular fractures from birth injury and skeletal dysplasia such as achondroplasia will present with short-neck features. Observation suffices for mild cases without functional deficit and for children under 6 years. Several operative techniques have been described for correction of Sprengel’s deformity, including scapular osteotomy, Green’s procedure, and Woodward’s procedure [14,15]. Procedures described at various time frames (8–11 years) aim to lower the scapula, resect the omo-vertebral bar, and improve cosmesis and function of the shoulder. The various surgical options are mentioned in Table 1,2.
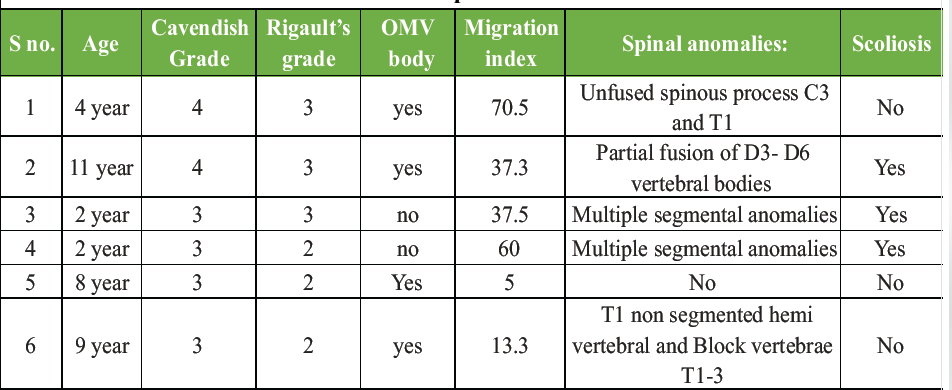
Table 1: Retrospective case series
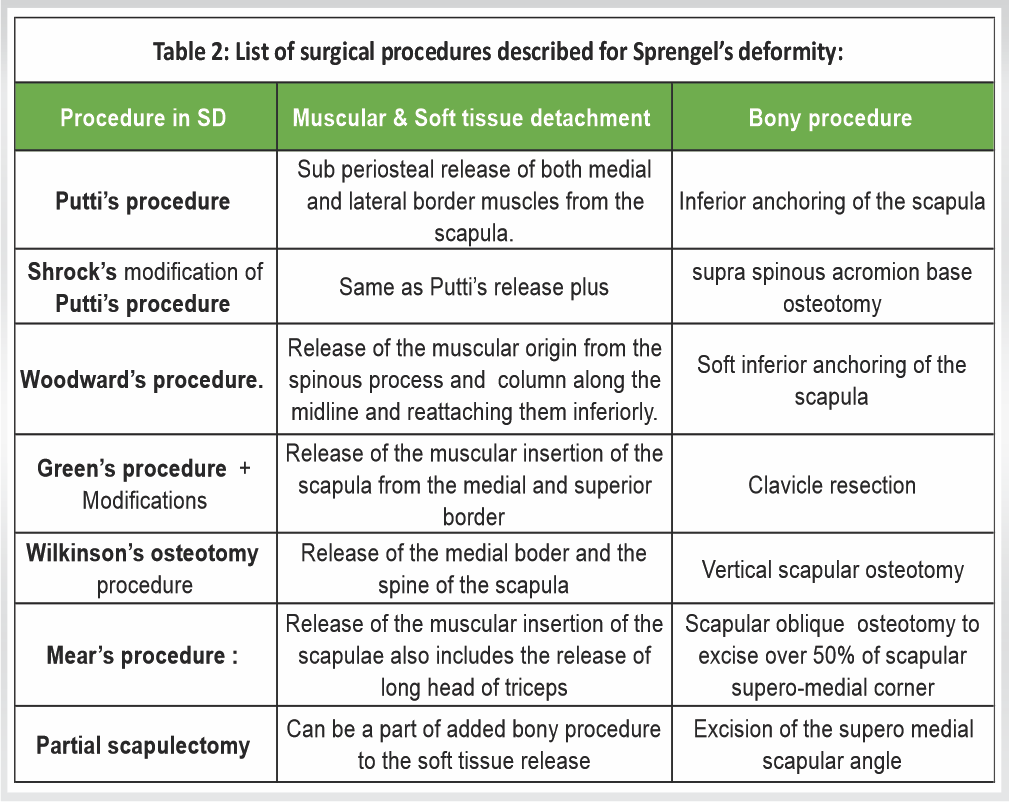
Table 2: List of surgical procedures described for Sprengel’s deformity.
In this retrospective case series, medical records and imaging data of paediatric patients diagnosed with SD were reviewed. Selection criteria included children aged ≤18 years with a clinical and radiological diagnosis of SD. Exclusion criteria were Sprengel’s in adults and syndromic-associated SD. Patients with incomplete clinical or imaging records were excluded. A total of six paediatric patients met the inclusion criteria and were analysed for their severity of deformity (Cavendish and Rigault grading) and for their other radiological features. Detailed clinical assessment focused on shoulder symmetry, scapular position, cosmetic appearance, and associated scoliosis. Shoulder abduction was measured clinically and documented pre- and post-intervention, where applicable. Radiological assessment included plain radiographs, anteroposterior views of both shoulders, X-rays of cervical, thoracic, and whole spine scoliograms, CT scans, and MRIs as indicated. Picture archiving and communication system imaging were used to evaluate the migration index, scapular rotation index, Broca’s index for scapular dysplasia, and associated congenital anomalies were recorded. The other senior author cross-checked the data at different time intervals, thereby eliminating the intraobserver bias.
- Scapular position and morphology
- Presence of omo-vertebral bone
- Congenital vertebral anomalies (including hemivertebrae, unsegmented bars, fused posterior elements, and spina bifida occulta)
- Rib anomalies
- Associated spinal deformities such as scoliosis
- Neural axis abnormalities, including tethered cord.
SD was graded using the Cavendish classification, and scapular elevation was assessed using the Rigault grading. Surgical intervention was considered based on the age, severity of deformity, functional limitation, cosmetic concerns, and willingness for informed consent for surgery. Woodward’s procedure was performed in a selected case of a 9-year-old boy. The intraoperative surgical steps using an extensile posterior approach (Figs. 3, 4, 5, 6, and 7). Exposure from mid-cervical to the lower border of the thoracic spine. The operative details include detachment of the trapezius and rhomboids from the spinous process, superomedial scapular release, scapular inferior repositioning, and distal plication. The documented operative records and the patient were followed up for outcome analysis.
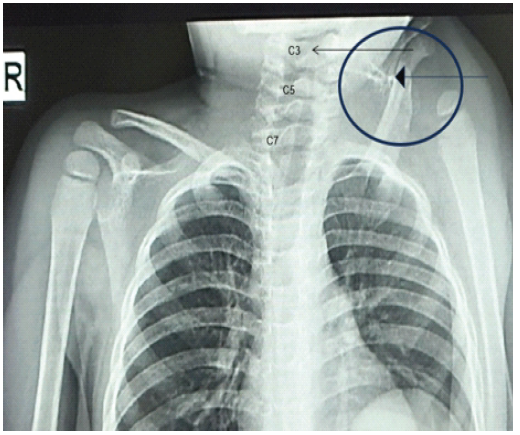
Figure 3: Case example of a 2-year-old with Grade 4 Sprengel’s deformity (Rigault). The scapula at the C3 level also demonstrates the omo-vertebral body on the left side, along with the unfused spinous process of C3 and T1.
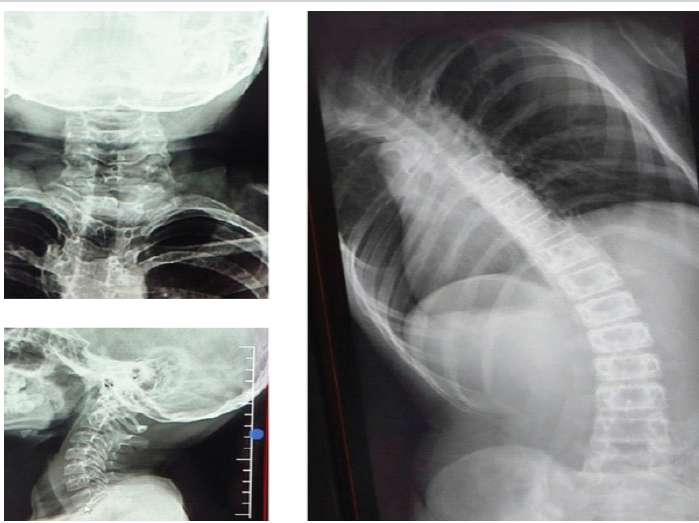
Figure 4: Case example of a 2-year-old with Grade 4 Sprengel’s deformity and omovertebral body, along with unfused spinous process of C3 and T1.
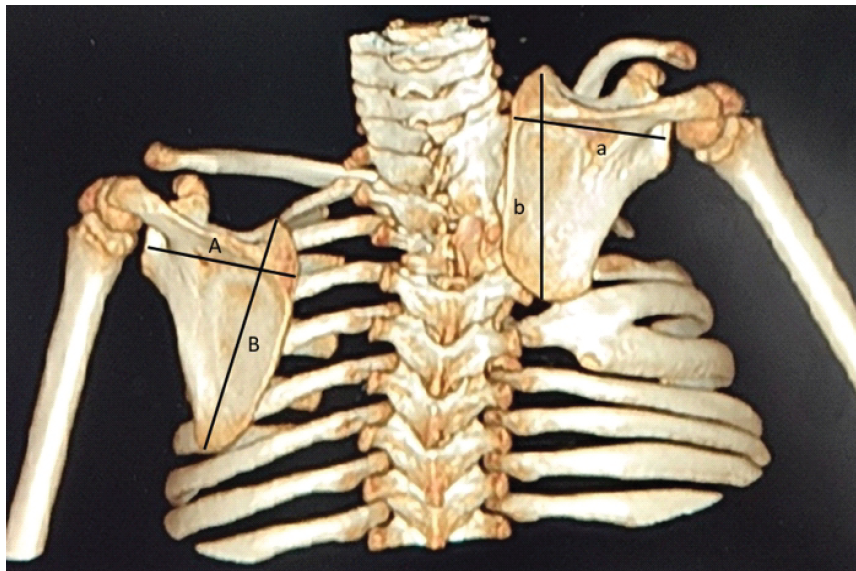
Figure 5: Case example of a 2-year-old: Sprengel’s deformity Grade 4 with cervico-thoracic scoliosis, dysplastic scapula resulting in low Broca’s index and high migration index 60.

Figure 6: Pre-operative clinical pictures of a 9-year-old boy showing high-riding scapula, restricted shoulder abduction of 40°, and altered scapulothoracic rhythm.
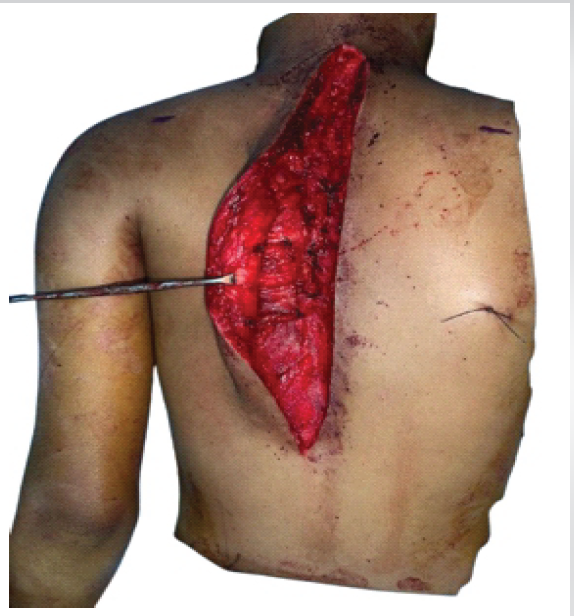
Figure 7: Intraoperative picture of Woodward’s procedure with an extensile posterior approach from mid cervical spine to lower thoracic vertebrae for the muscular releases.
Data were analysed descriptively due to the small sample size. Continuous variables were summarised as ranges, and categorical variables were presented as frequencies. Post-operative outcomes were assessed clinically and radiologically. Primary outcome measures were improvement in cosmetic appearance, change in shoulder abduction, and occurrence of perioperative and post-operative complications. The age range at presentation was between 2 and 11 years, with a mean age of 6 years. Despite the presence of spinal anomalies in over 80% of cases, the neurological examinations were normal in all the cases, and all were unilateral SD cases. The non-operative cases had a Cavendish grade of 3–4 (moderate to severe) and Rigault grades 2–3. These are expected to worsen with progressive growth. They decided on non-surgical due to social and financial reasons. The radiological features of OB were seen in over 60% of cases and scoliosis in 50% of cases, the most common being cervico-thoracic scoliosis, and only one of our case series had dorsal scoliosis secondary to partial fusion of D3-6 (Fig. 4). The children with scoliosis invariably had a spectrum of multiple cervical spinal anomalies. Even at early years (2 years of age), the plain radiographs show the OM associated with SD (Fig. 3). CT scans with 3D showed a Broca’s index of an average of 40 (normal 68–71), a rotational index of an average of 2.2 and a migration index of an average of 36. SD with severe scapular rotation showed a higher rotational index and a low migration index, explained by the reverse concept. In addition, CT showed other associated anomalies (Fig. 5). Functional outcome scoring in SD is commonly assessed using Cavendish classification for cosmetic severity and Rigault’s grading by radiological methods. Additional shoulder range of movement in specific abduction is a key determinant outcome factor (shoulder abduction >120 – mild/no limitation; 90–120 – moderate limitation; and <90 – severe limitation). The operated case of SD had a pre-operative Cavendish Grade 3 and Rigault’s Grade 2. The preoperative clinical appearance demonstrated a high-riding scapula with restricted shoulder abduction of 40 degrees and altered scapulothoracic rhythm (Fig. 6). His migration index measured 13.3 (Fig. 1b), showing an inverse relation to the rotational index of 1.67 (Fig. 2a); his Cavendish grade improved to Grade 3-1, showed good cosmetic correction, and shoulder abduction movement improved from 40° to 90°. His post-operative period was uneventful, and he recovered without any complications. Postoperative clinical assessment demonstrated improved shoulder symmetry and correction of deformity (Fig. 8). Modified Japanese Orthopaedic Association type functional evaluation of shoulder – no pain with good cosmetic correction, with improved range of shoulder movements in his activities of daily living.

Figure 8: Post-operative clinical assessment for correction of the shoulder.
SD remains the most common congenital shoulder deformity, although it is a rare condition overall, with an incidence of 0.3/10000 live births. Its diagnosis is clinical, but often confirmation needs radiographs. In view of the frequent association with scoliosis, all cases of SD could be considered for a scoliogram in addition to both shoulder radiographs as first-line investigation. A CT scan helps to assess the degree of superior migration and rotational deformity. The higher the degree of scapular rotation, the lower the migration; hence, both the rotational and migration indices need to be assessed together. In addition to clinico-radiological grading with “Cavendish” and “Rigault’s system”, shoulder abduction should be included for functional assessment. An MRI scan becomes the gold standard to exclude the fibrous omo-vertebral bodies and to assess the associated spinal dysraphism. Non-operative treatment in severe cases was shown to deteriorate in shoulder function [16] with time. The surgical procedures meant for SD were not purely for cosmesis but also showed improvement in the shoulder abduction and elevation angles [12]. Overall, the surgical procedures are documented to be safe and achieve both cosmetic and functional improvements in over 98% of cases [17,18,19]. The ideal age for Sprengel correction is usually between 3 and 6 years and is acceptable up to 8 years, as it shows better anatomical definition and post-operative cosmetic improvement [17]. Complications and the outcomes from surgical interventions depend on the severity of the grade, age of intervention, the type of surgery, and the associated spinal anomalies. Interestingly, the Cavendish 3–4 deformity in patients younger than 8 years, when subjected to surgical correction, shows better correction and functional outcome [17]. Minor complications include scar-related wound breakdown, necrosis, keloids, heterotrophic ossification, and scar cosmesis. The other typical ones are incomplete deformity correction, progression of scoliosis, and the need for revision surgery. The unusual ones include brachial plexus palsy, pleural lesions, and the rotary subluxation [18] after surgical relocation of SD. The SD associated with cervico-thoracic anomalies should be considered a complex type of SD that needs surveillance till growth maturation. The systematic review has shown both Green’s and Woodward’s procedures aimed at anatomical relocation of the scapula to be the most frequently performed surgeries in SD [17]. Woodward’s procedure has been shown to restore cosmetic correction and, in the long term, shoulder function [20].
Limitations of the study:
This retrospective study has a small sample size with a heterogeneous age group of SD that precludes statistical analysis. Furthermore, it has selection bias from a single centre, without a long-term follow-up till skeletal maturity.
Despite the heterogeneity of the associated anomalies in SD, the age of intervention and the type of procedure for individual cases in children carry a different outcome after surgical intervention.
The diagnosis of Sprengel’s deformity is clinical, but further investigations are recommended at the earliest assessment. An MRI for its associated spinal dysraphism and a CT scan for its rotational deformity become mandatory. Pre-operative grading of SD, along with the functional range of shoulder movements, should be used in severity assessment. Moderate-to-severe grades of SD need surgical intervention and surveillance till growth maturity becomes inevitable in cases associated with fused and hemi-fused cervical and thoracic vertebrae.
References
- 1. Kulkarni ML. Sprengel’s deformity. Indian Pediatr 1994;31:865-8. [Google Scholar] [PubMed]
- 2. Chinn DH. Prenatal ultrasonographic diagnosis of Sprengel’s deformity. J Ultrasound Med 2001;20:693-7. [Google Scholar] [PubMed]
- 3. Samartzis D, Herman J, Lubicky JP, Shen FH. Sprengel’s deformity in Klippel-Feil syndrome. Spine (Phila Pa 1976) 2007;32:E512-6. [Google Scholar] [PubMed]
- 4. Kadavkolan AS, Bhatia DN, Dasgupta B, Bhosale PB. Sprengel’s deformity of the shoulder: Current perspectives in management. Int J Shoulder Surg 2011;5:1-8. [Google Scholar] [PubMed]
- 5. Cavendish ME. Congenital elevation of the scapula. J Bone Joint Surg Br 1972;54:395-408. [Google Scholar] [PubMed]
- 6. Rigault P, Pouliquen JC, Guyonvarch G, Zujovic J. Congenital elevation of the scapula in children. Anatomo-pathological and therapeutic study of 27 cases. Rev Chir Orthop Reparatrice Appar Mot 1976;62:5-26. [Google Scholar] [PubMed]
- 7. Horwitz AE. Congenital elevation of the scapula (Sprengel’s deformity). J Bone Joint Surg 1908;2:260-311. [Google Scholar] [PubMed]
- 8. Cho TJ, Choi IH, Chung CY, Hwang JK. The Sprengel deformity: Morphometric analysis using 3D-CT and its clinical relevance. J Bone Joint Surg Br 2000;82:711-8. [Google Scholar] [PubMed]
- 9. Dilli A, Ayaz UY, Damar C, Ersan O, Hekimoglu B. Sprengel deformity: Magnetic resonance imaging findings in two pediatric cases. J Clin Imaging Sci 2011;1:13. [Google Scholar] [PubMed]
- 10. Bisht RU, Belthur MV, Singleton IM, Goncalves LF. Prenatal diagnosis of Sprengel’s deformity in a patient with Klippel-Feil syndrome. Clin Imaging 2021;78:45-50. [Google Scholar] [PubMed]
- 11. Jaczyńska R, Bekiesinska-Figatowska M, Sobieraj P, Issat T, Gos M, Obersztyn E. Prenatal and neonatal ultrasound and magnetic resonance imaging diagnosis of Sprengel’s deformity with unusual associations. Fetal Diagn Ther 2023;50:269-75. [Google Scholar] [PubMed]
- 12. Khabyeh-Hasbani N, O’Brien DM, Meisel EM, Koehler SM. Current concepts in brachial plexus birth injuries: A comprehensive narrative review. Plast Reconstr Surg Glob Open 2024;12:e6083. [Google Scholar] [PubMed]
- 13. Menger RP, Rayi A, Notarianni C. Klippel-Feil syndrome. In: StatPearls. TreasureIsland, FL: StatPearls Publishing; 2025. [Google Scholar] [PubMed]
- 14. Sulamaa M, Wallgren GR. Congenital high scapula (Sprengel’s deformity). Acta Orthop 1954;24:195-206. [Google Scholar] [PubMed]
- 15. Wilkinson JA, Campbell D. Scapular osteotomy for Sprengel’s shoulder. J Bone JointSurg Br 1980;62-B:486-90. [Google Scholar] [PubMed]
- 16. Vuillermin C, Wang KK, Williams KA, Hresko MT, Waters PM. Sprengel’s deformity: An analysis of surgically and nonsurgically treated patients. J Shoulder Elbow Surg 2021;30:e1-9. [Google Scholar] [PubMed]
- 17. Zarantonello P, Di Gennaro GL, Todisco M, Cataldi P, Stallone S, Evangelista A, et al. Surgical treatment of Sprengel’s deformity: A systematic review and meta-analysis. Children (Basel) 2021;8:1142. [Google Scholar] [PubMed]
- 18. Kim JK, Cho TJ, Lee K, Moon HJ, Park MS, Yoo WJ, et al. Atlantoaxial rotatory subluxation after surgical relocation of Sprengel deformity: A case report. J Pediatr Orthop B 2012;21:276-9. [Google Scholar] [PubMed]
- 19. Ahmad AA. Surgical correction of severe Sprengel deformity to allow greater postoperative range of shoulder abduction. J Pediatr Orthop 2010;30:575-81. [Google Scholar] [PubMed]
- 20. Siu KK, Ko JY, Huang CC, Wang FS, Chen JM, Wong T. Woodward procedure improves shoulder function in Sprengel deformity. Chang Gung Med J 2011;34:403-9. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Bilateral Sprengel’s Deformity Treated with Bilateral Modified Woodward Procedure: A Case Report
April 1, 2026 Bilateral Sprengel’s Deformity Treated with Bilateral Modified Woodward Procedure: A Case Report October 8, 2012 The Pelvic Digit: A Rare Congenital Anomaly as a Cause of Hip Pain
October 8, 2012 The Pelvic Digit: A Rare Congenital Anomaly as a Cause of Hip Pain April 1, 2026 Non-neoplastic Orthopedic Pathology – A Systematic Review
April 1, 2026 Non-neoplastic Orthopedic Pathology – A Systematic Review October 10, 2021 Calcaneal Osteomyelitis Treated with Antibiotic Mixed Calcium Sulphate Pellets. A Case Report
October 10, 2021 Calcaneal Osteomyelitis Treated with Antibiotic Mixed Calcium Sulphate Pellets. A Case Report