
No matter what type of pediatric Monteggia fracture you are presented with, if a stable closed reduction cannot be achieved then do not hesitate in performing a stable open reduction and internal fixation, as restoring the anatomy will guarantee excellent end results.
Ehab S Saleh, MD. 3535 West 13-Mile Road, Suite 744, Royal Oak. MI 48073. E-mail: ehab.saleh3@beaumont.org
Abstract
Introduction: Monteggia fracture-dislocations are rare and complex injuries that usually involve a fracture of the proximal ulna associated with a proximal radioulnar and radiocapitellar joint dislocations. These injuries comprise <1% of all pediatric forearm fractures. We report on a pediatric Monteggia fracture-dislocation variant that included an irreducible divergent ulnohumeral joint dislocation, an irreducible anterior radial head dislocation, and a proximal and distal radius and ulna fracture.
Case Report: A 6-year-old female came to our emergency room with a right elbow and forearm pain and deformity after a fall from a slide on the same day. X-rays revealed a divergent ulnohumeral joint dislocation, an anterior radiocapitellar joint dislocation, a proximal radioulnar joint dislocation, and a proximal and distal ulna and radius fracture. Closed reduction under sedation in the emergency room was not successful, with persistent ulnohumeral, ulnoradial, and radiocapitellar joint dislocations. The patient was taken to the operating room the next morning. She underwent open reduction and internal fixation of the proximal ulna fracture with a one-third tubular locking plate, and radial head dislocation open reduction. A stable reduction of the ulnohumeral joint was only possible after the fixation of the proximal ulna fracture. The most stable position for the radiocapitellar joint after its open reduction was at 70o of elbow extension and full forearm supination; the patient was casted in that position for 6 weeks.
Conclusion: Pediatric Monteggia fracture-dislocations are rare and complex childhood fractures, and new variants of this injury can have even more complex presentations. Open reduction and stable internal fixation addressing all components of this injury will lead to an excellent outcome.
Keywords: Pediatric monteggia fracture-dislocation, new type four variant, divergent ulnohumeral joint dislocation, irreducible dislocation.
In 1814, Giovanni Battista Monteggia, an Italian surgeon, first described the injury that now bears his name as a fracture of the proximal third of the ulna and an anterior dislocation of the radial head [1].
In 1962, Jose Luis Bado, a Uruguayan orthopedic surgeon, published his classic monograph on the classification of Monteggia lesions. Bado described in this monograph the types of fracture-dislocation of the proximal radioulnar joint, with a focus on type I Monteggia fracture with anterior dislocation of the radial head and fracture of the proximal ulna. He also discussed the other Monteggia fracture-dislocation types where the radial head dislocates posteriorly or laterally [2].
A Monteggia fracture-dislocation variant with a divergent elbow dislocation has not been reported in a pediatric patient before and was only reported once in an adult patient [3].
To our knowledge, no report has described the combination of injuries sustained by this pediatric patient which in its totality constitute a new Monteggia type 4 variant.
A 6-year-old female came to our emergency room with a right elbow, forearm, and wrist pain, swelling, and deformity after she fell from a slide on the same day. X-rays revealed a divergent ulnohumeral joint dislocation, anterior radiocapitellar joint dislocation, a proximal radioulnar joint dislocation, a proximal ulna angulated greenstick fracture with extension into the olecranon, a same level proximal radius minimally displaced fracture, a distal radius Salter-Harris type 2 fracture, and a distal ulna buckle fracture (Fig. 1, 2, 3).
Closed reduction under sedation in the emergency room was not successful, with persistent ulnohumeral, and radiocapitellar joint dislocations (Fig. 4).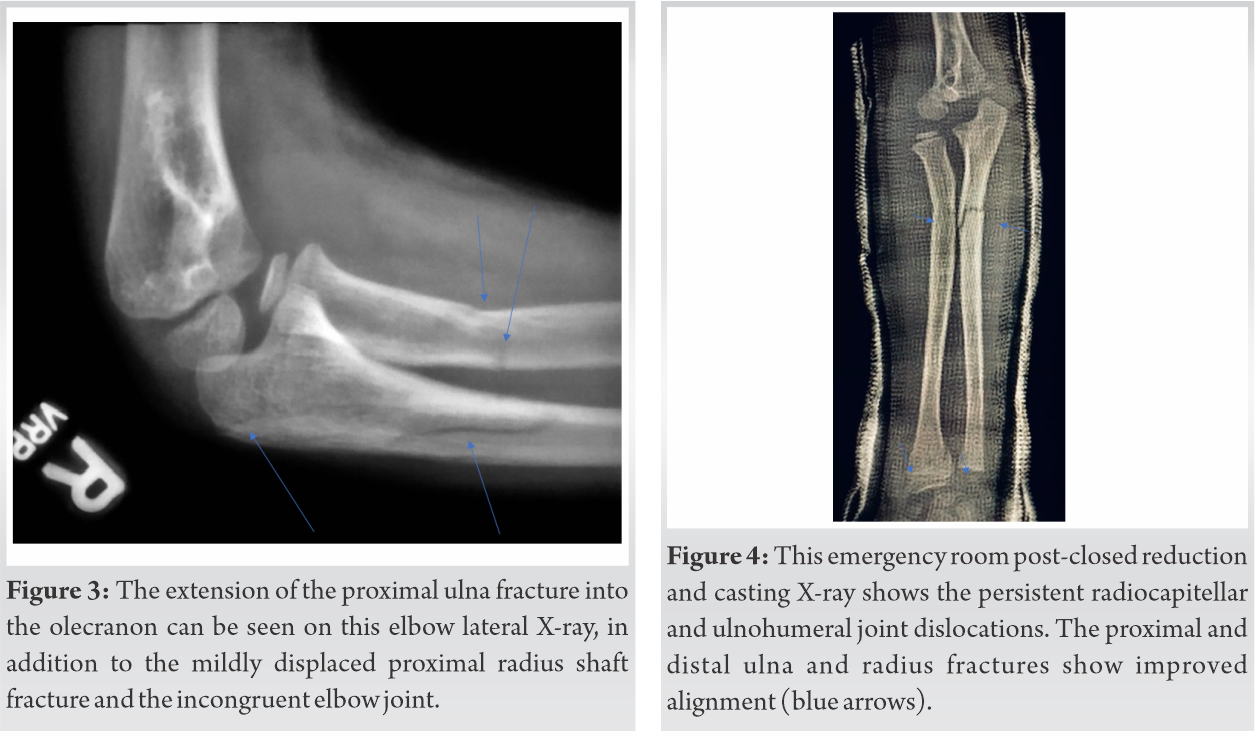
The patient was taken to the operating room the next morning. Under general anesthesia, the proximal ulna fracture was addressed first and was fixed with a 3.5 mm one-third tubular locking plate. The fracture extension into the olecranon process did not allow for fixation with a flexible nail. After fixation of the proximal ulna, the divergent elbow dislocation was easily reduced by closed manipulation. Closed reduction of the radial head was not successful. An open reduction of the radial head did show that the obstacle to reduction was the annular ligament, which was subluxed from around the head of the radius and interposed between the radial head and the capitellum. Two 2-0 Tycron sutures were used to tag the annular ligament and apply gentle traction on it. A hemostat was used to dilate the annular ligament and bring it over to its anatomic location around the radial head. The proximal radius and the distal radius and ulna fracture were stable and in anatomic alignment and did not require internal fixation.
The most stable elbow position for the radiocapitellar joint intraoperatively following its open reduction was in 70° of elbow extension and full forearm supination, so the patient was casted in that position for 6 weeks (Fig. 5). We felt that the radiocapitellar joint was stable enough without adding a smooth trans-capitellar Kirschner wire.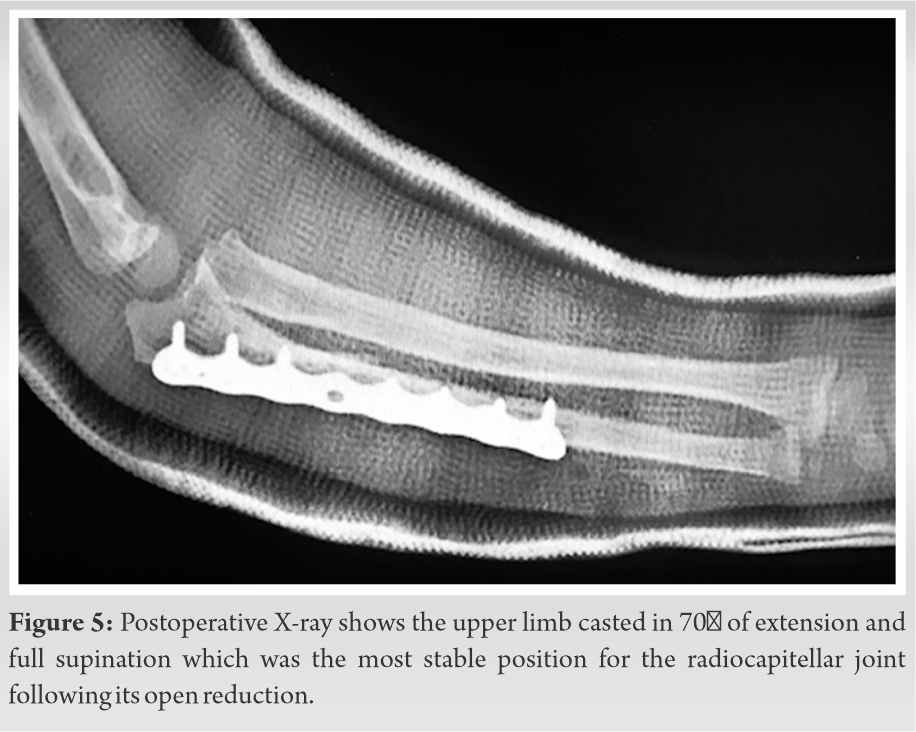
The cast was removed after 6 weeks, and she gradually regained range of motion and strength with a home exercise program.
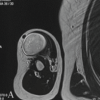
At her 10 months follow-up, her elbow, forearm, and wrist range of motion were normal, and her X-rays showed a well-aligned elbow joint (Fig. 6a, 6b). The plate was removed 2 months later.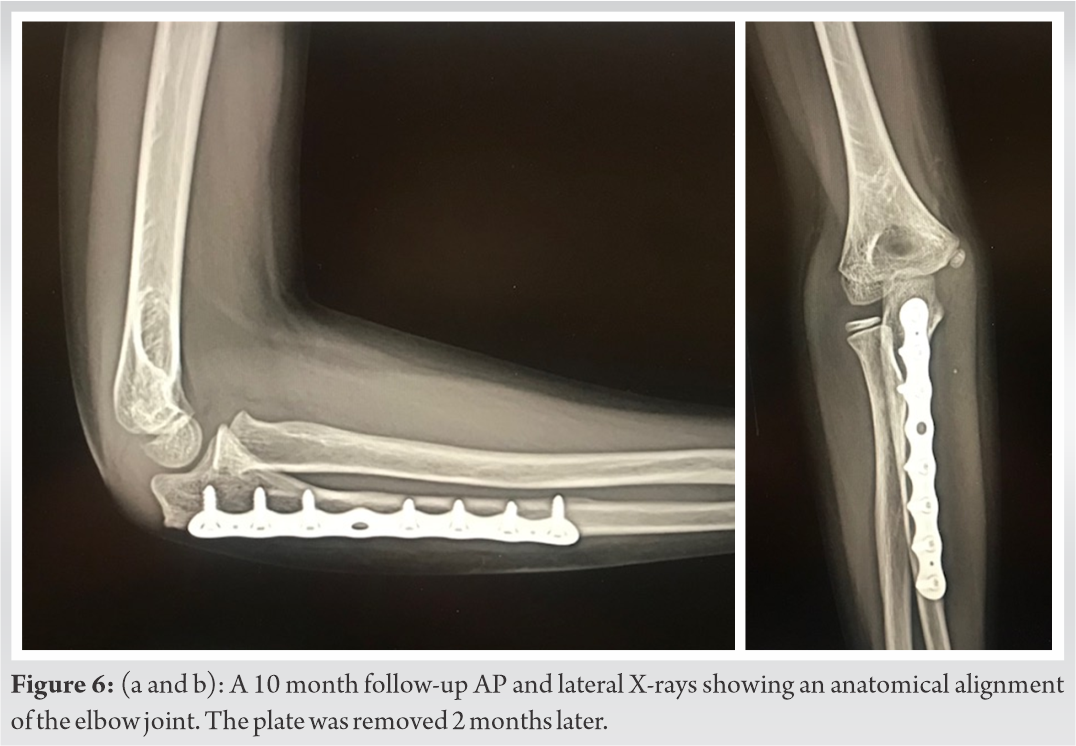
Bado classified the Monteggia lesion into four types, also including type one and type two equivalent lesions. He has described seven Type 1 equivalent injuries, including type 1 equivalent number six, which consists of posterior dislocation of the elbow and a fracture of the ulnar diaphysis with or without a fracture of the proximal radius, and type 1 equivalent number seven, which is associated with various wrist lesions including a Galeazzi lesion. He also stated that Monteggia types three and four have no equivalents [4].
It is accepted that good results can be achieved after closed reduction and casting in a child with Monteggia fracture, as the type of fractures in this age group is usually either a plastic deformation, a buckle fracture, or a greenstick fracture, which are usually stable after a closed reduction. This is contrary to the situation in adults, where plate and screw fixation of the ulna is usually needed [5].
In our case, closed reduction achieved good alignment of the proximal and distal ulna and radius shaft fracture but failed to reduce the associated elbow, proximal radioulnar, and radiocapitellar dislocations (Fig. 4). Intraoperatively, the proximal ulna fracture was found to be more unstable than what the plain X-rays suggested; the fracture was found to be with some comminution and an extension into the posterior olecranon. Stable reduction of the elbow joint was only possible after rigid fixation of the proximal ulna. The radial head obstacle to reduction was the entrapped annular ligament, and, even after open reduction, that joint was not completely stable through the full arc of elbow motion; its most stable position was in 700 of elbow extension and full forearm supination.
Pediatric Monteggia fracture-dislocations are rare and complex childhood fractures, and new variants of this injury can have more complex presentations. Open reduction and internal fixation addressing all components of the injury will lead to an excellent outcome [6,7,8,9,10].
No matter what type of pediatric Monteggia fracture you are presented with, if a stable closed reduction cannot be achieved then do not hesitate in performing a stable open reduction and internal fixation, as restoring the anatomy will guarantee excellent end results.
References
- 1.Andjelković S, Vučković Č, Milutinović S, Palibrk T, Kadija M, Bumbaširević M. giovanni battista monteggia (1762-1815). Srp Arh Celok Lek 2015;143:105-7. [Google Scholar | PubMed]
- 2.The Monteggia Lesion. By José Luis Bado, M.D., Professor of Surgery, University of Montevideo Medical School; Director, Institute for Orthopaedics and Traumatology, Montevideo, Uruguay. Translated from the Spanish by Ignacio V. Ponseti, M.D. 10 x 7 in. Pp. ix+78, with 59 figures. 1962. Springfield, Illinois: Charles C. Thomas, Publisher. Oxford: Blackwell Scientific Publications Ltd. Price 54s. J Bone Joint Surg Br Vol 1962;44-B:968-8. [Google Scholar | PubMed]
- 3.Laratta JL, Yoon RS, Frank MA, Koury K, Donegan DJ, Liporace FA. Divergent elbow dislocation with radial shaft fracture, distal ulnar deformation, and distal radioulnar joint instability: An unclassifiable Monteggia variant. J Orthop Traumatol 2014;15:63-7. [Google Scholar | PubMed]
- 4.Bado JL. The Monteggia lesion. Clin Orthop Relat Res 1967;50:71-86. [Google Scholar | PubMed]
- 5.Ring D, Waters PM. Operative fixation of Monteggia fractures in children. J Bone Joint Surg Br 1996;78:734-9. [Google Scholar | PubMed]
- 6.Hart CM, Alswang J, Bram J, Kim ST, Arkader A, Silva M. Operative versus nonoperative management of acute pediatric monteggia injuries with complete ulna fractures. J Pediatr Orthop 2021;41:412-6. [Google Scholar | PubMed]
- 7.Zheng ET, Waters PM, Vuillermin CB, Williams K, Bae DS. Surgical reconstruction of missed monteggia lesions in children. J Pediatr Orthop 2020;40:e916-21 [Google Scholar | PubMed]
- 8.Foran I, Upasani VV, Wallace CD, Britt E, Bastrom TP, Bomar JD, et al. Acute pediatric monteggia fractures: A conservative approach to stabilization. J Pediatr Orthop 2017;37:e335-41. [Google Scholar | PubMed]
- 9.Bae DS. Successful strategies for managing monteggia injuries. J Pediatr Orthop 2016;36:S67-70. [Google Scholar | PubMed]
- 10.Ramski DE, Hennrikus WP, Bae DS, Baldwin KD, Patel NM, Waters PM, et al. Pediatric monteggia fractures: A multicenter examination of treatment strategy and early clinical and radiographic results. J Pediatr Orthop 2015;35:115-20. [Google Scholar | PubMed]

Related Articles in Journal of Orthopaedic Case Reports
 January 1, 2026 Intratendinous Lipoma of Biceps Long Head: A Case Report and Current Concepts Review of Musculoskeletal Lipomas
January 1, 2026 Intratendinous Lipoma of Biceps Long Head: A Case Report and Current Concepts Review of Musculoskeletal Lipomas February 1, 2026 A Humeral Shaft Non-union Treated With Proximal Tibia Cancellous Autograft and Fibular Strut Allograft: A Case Report
February 1, 2026 A Humeral Shaft Non-union Treated With Proximal Tibia Cancellous Autograft and Fibular Strut Allograft: A Case Report September 5, 2019 Reluctance to Cite our Peers in articles: Story of Academic Betrayals
September 5, 2019 Reluctance to Cite our Peers in articles: Story of Academic Betrayals April 10, 2016 Treatment of Humeral Fracture after Shoulder Arthroplasty using Functional Brace: A Case Report
April 10, 2016 Treatment of Humeral Fracture after Shoulder Arthroplasty using Functional Brace: A Case Report