
Complex femur shaft fractures in children are rare injuries and which are difficult to manage and restoration of the anatomical alignment is the main goal in the management of these fractures.
Dr. Shrihari L Kulkarni, Department of Orthopaedics, SDM College of Medical Sciences and Hospital, Shri Dharmasthala Manjunatheshwara University, Dharwad, Karnataka, India. E-mail: shrihari1711@gmail.com
Abstract
Introduction: Complex femur fractures are defined as combined fractures of shaft and proximal of or the distal femur. Restoration of anatomical alignment is the primary goal of the management of these fractures. In this report, we describe the management of complex femur shaft fractures in three pediatric patients.
Case Report: This report includes three patients. The first patient was a 10-year-boy with comminuted proximal femur shaft fracture extending into the subtrochanteric area, managed with minimally invasive sub-muscular plating. The second patient was a 12-year-boy with comminuted femur shaft extending into subtrochanteric area, treated with combined retrograde and anterograde Titanium Elastic Nail System. A 12-year-old boy with femur shaft with intertrochanteric fracture managed with K-wire fixation for intertrochanteric fracture and plating with dynamic compression plate for femur shaft was our third patient. All patients had excellent radiological and functional outcome.
Conclusion: Complex femur shaft fractures in children are very rare and challenging injuries. With proper pre-operative planning and use of appropriate implants excellent outcomes can be obtained.
Keywords: Complex femur fractures, pediatric orthopedics, sub-muscular plating, titanium elastic nailing.
Femur shaft fractures (including subtrochanteric and supra-condylar) account for 1.6% of all pediatric fractures. The most common femur shaft fracture pattern in children (more than 50%) is simple transverse, closed and non-comminuted. Complex femur fractures in children are rare and occur due to high-energy trauma such as road traffic accident or fall from height [1,2].
Complex femur fractures are defined as combined fractures of shaft and proximal or distal femur. Orthopedic trauma association (OTA) Type C fractures, i.e., multi-fragmentary fractures (oblique, spiral, or irregular) and segmental femur fractures are also considered as complex femur fractures in adults. Whereas, in children, OTA 32-D4.2 and 5.2 are considered to be complex fractures [3,4].
Management of these fractures is very challenging. Most of these fractures are managed surgically as they are inherently unstable. The primary goal in the management of these fractures is the restoration of the anatomical alignment. In this report, we describe the management of complex femur fractures in pediatric patients.
Case 1 (Fig. 1)
A 10-year-old boy presented to us with an injury to his right thigh following fall while playing. The proximal third of the thigh was swollen with painful restricted movements in the right hip and inability to bear weight on the affected limb. On examination, the limb was externally rotated and shortened with diffuse tenderness in the proximal femur. Radiographs showed a comminuted proximal femur shaft fracture extending into the sub-trochanteric area with a vertical slit in the distal fragment (OTA 32-D5.2) [4]. After informed consent from the parents, under spinal anesthesia, with a patient in the left lateral position, minimally invasive submuscular bridge plating was done with 11 holed, 4.5 mm locking plate. The plate was bent proximally to match the contour of the trochanteric flare. The limb was immobilized post-operatively for 3 weeks.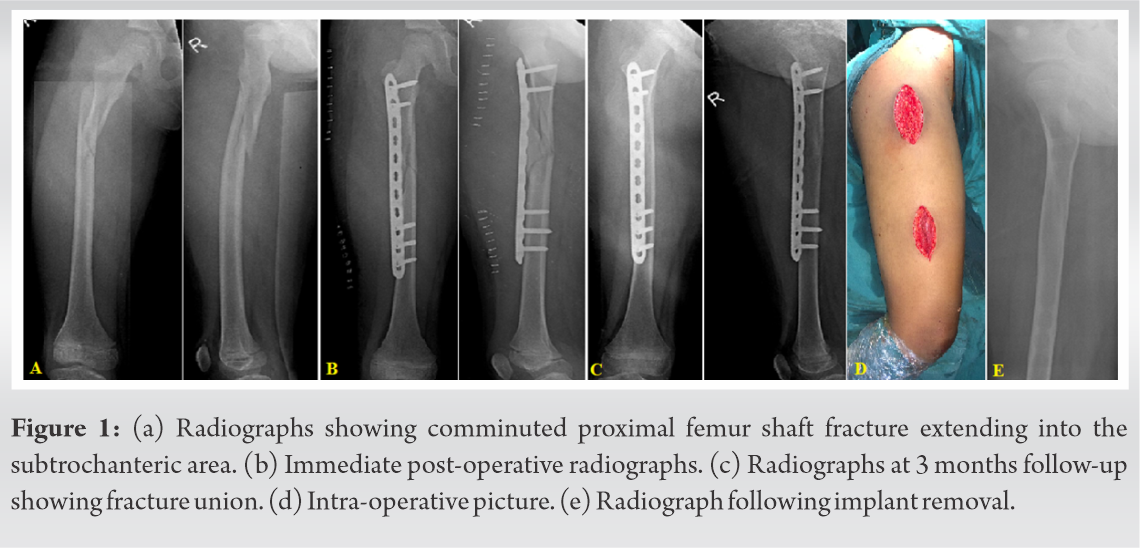
Mobilization of the hip and knee were started at 3 weeks while keeping the child non-weight bearing. At 9 weeks, fracture showed union at which time full weight-bearing mobilization was started. Patient was followed up regularly and implant removal was done at 9 months. Six weeks after removal of the implant, the child returned back to his pre-fracture level of activity, and presently at 2-year follow-up* he continues to be free of any symptoms or complications related to the femur fracture.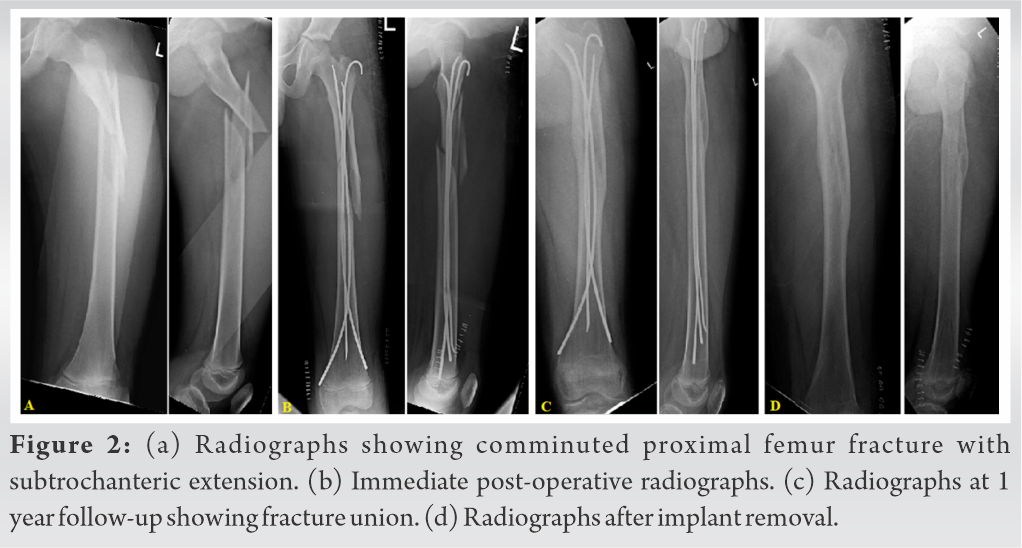
Case 2 (Fig. 2)
A 12-year-old presented with pain in the left thigh and inability to bear weight following fall from a bicycle. Physical examination revealed a diffuse swelling in the thigh with ecchymosis on the lateral aspect of the proximal thigh. The limb appeared externally rotated and deformed. X-rays revealed comminuted left femur shaft fracture extending into the sub-trochanteric area (OTA 32–D5.2) [4]. After obtaining informed consent from the parents the patient was taken up for surgery. With the patient in the supine position, closed reduction and fixation with Titanium Elastic Nail System (TENS) was performed. Two 3.5mm nails were passed retrogradely with entry just above the physeal line on medial and lateral supracondylar aspect. One 3 mm nail was passed anterogradely with entry from the tip of the greater trochanter to achieve a better stability considering the fracture configuration. Post-operatively limb was immobilized with a high groin slab for 6 weeks. Mobilization of the hip and knee was started at 6 weeks while keeping the patient non-weight bearing. At 12 weeks, fracture showed signs of satisfactory union at which partial weight-bearing mobilization was started progressing to full weight bearing by 4 months. The TENS nails were removed at 1 year and presently at 3-year follow-up* he continues to be free of any symptoms or complications related to the femur fracture.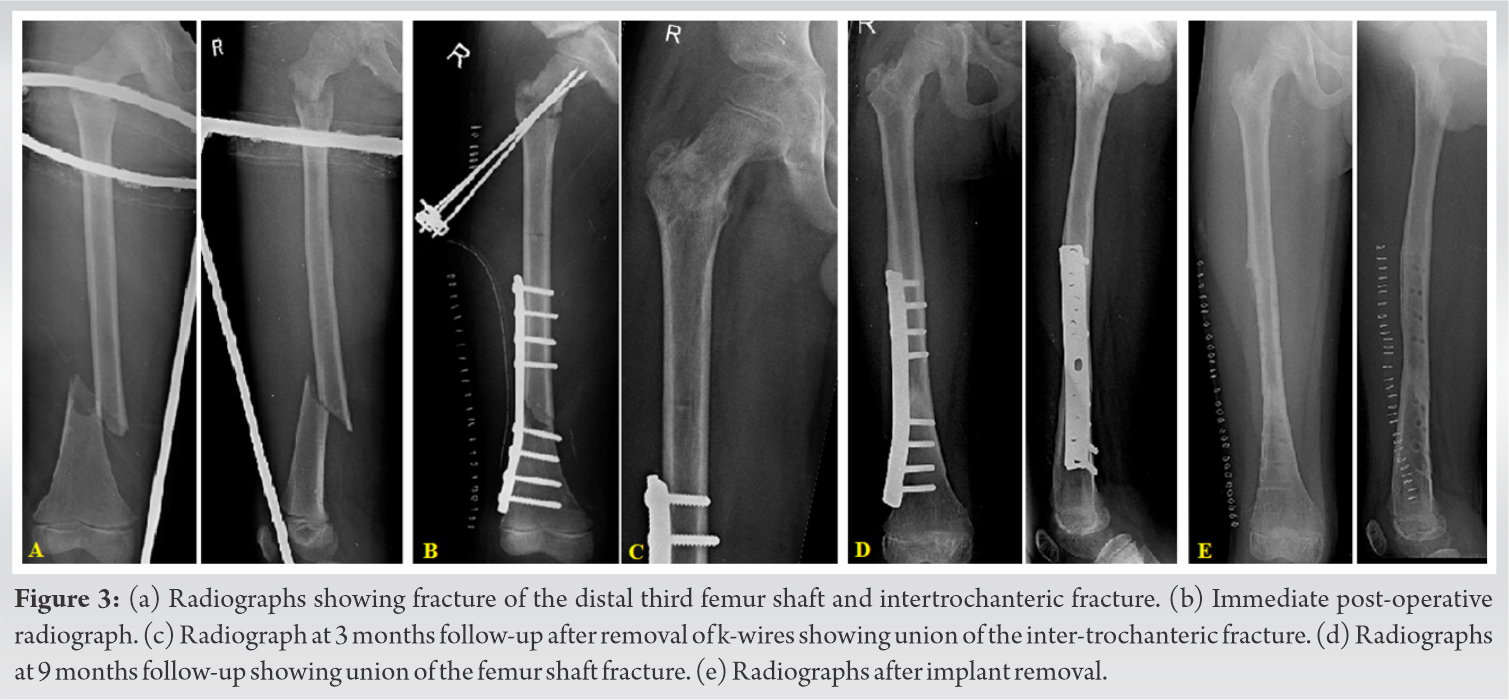
Case 3 (Fig. 3)
A 12-year-old boy who was hit by truck presented to us with pain, swelling in the right thigh, and inability to move the hip and knee. On examination, the right thigh was diffusely swollen with tenderness in the hip and distal third of the thigh. The limb was externally rotated and shortened. Patient also had head injury which was managed conservatively. X-rays showed right femur shaft fracture in the distal one-third along with Delbet type IV fracture of the right hip [5]. Informed consent was obtained from parents and the patient was taken up for surgical fixation.
The patient was placed on the fracture table and the intertrochanteric fracture was addressed first. Closed reduction was achieved with traction and internal rotation. The fracture was fixed using three 2.5 mm k-wires, inserted from the lateral cortex into the neck of the femur. The fracture reduction and the position of the K-wires was confirmed by the C-arm. K-wires were connected by L-shaped connecting rod with JESS clamps. TENS would have been ideal for fixation of the fracture of the shaft of the femur, but in this case, due to the presence of K-wires in the proximal femur, fixation with TENS would not have been feasible. Open reduction and internal fixation with 9 holed 4.5 mm broad dynamic compression plate (DCP) was done for the femur shaft fracture. Postoperatively, the limb was immobilized with a high groin slab, and patient was followed up regularly.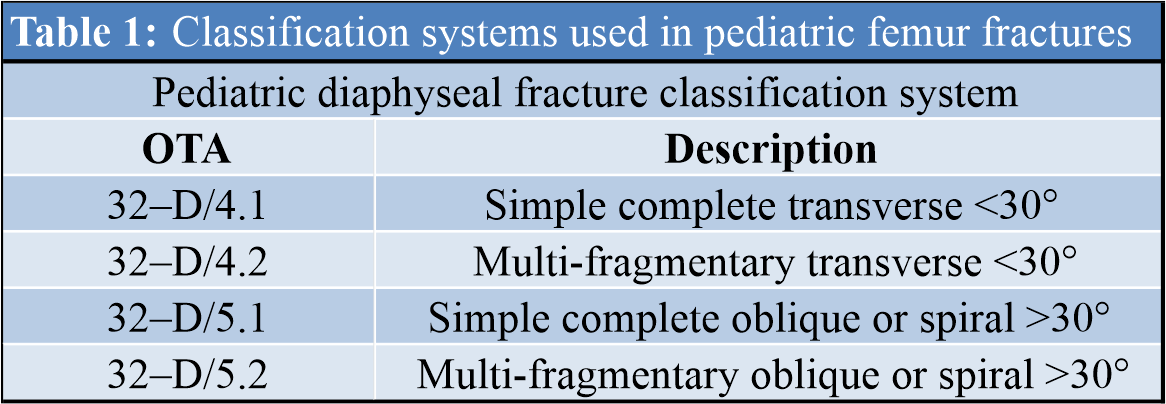
The intertrochanteric fracture united at 8 weeks at which time the K-wires were removed and bedside mobilization of the hip and knee was started. At 12 weeks follow-up, the femoral shaft fracture also united allowing partial weight-bearing which was progressed to full weight-bearing over the next month. The DCP in the femur was removed at 1 year and at 3-year follow-up* he continues to be free of any symptoms or complications related to the femur fracture.
*All latest follow-ups were done on phone due to ongoing Covid-19 pandemic.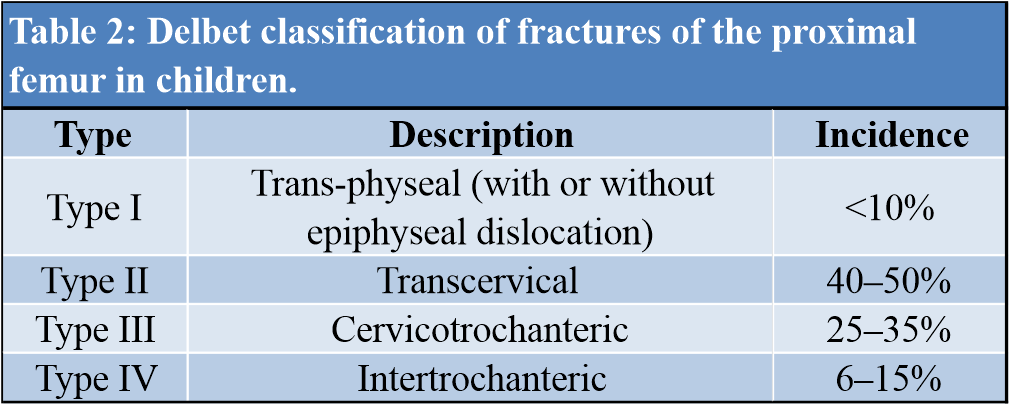
Femur shaft fractures are the most common fractures requiring hospitalization in children. The management of these fractures mainly depends on the age of the child. Weight of the child, fracture configuration, associated injuries/polytrauma, experience of the treating surgeon, and the cost of the treatment are other factors influencing the treatment [6]. Surgical management is the mainstay in the management of the complex femur fractures. These are very unstable fractures occurring due to high-energy trauma.
There is no universal classification available for the pediatric shaft femur fractures. Usually, descriptive classification on the basis of fracture configuration, comminution, and open/closed is used [1].
According to OTA, pediatric shaft femur fractures are classified as category 32-D (Table 1). They are further sub-classified as simple i.e., 32-D 4.1 (complete transverse with an obliquity of 30° or less) and 32-D 5.1 (complete oblique or spiral more than 30) and complex i.e., 32-D 4.2 (multi-fragmentary transverse 30 or less) and 32-D 5.2 (multi-fragmentary oblique or spiral more than 30) fractures [4].
Fractures around the hip in children are divided into four types as described by Delbet (Table. 2). Type I: Trans-epiphyseal separation (<10%). Subtypes are IA (without dislocation) and IB (with dislocation). Type II: Transcervical fracture. This is the most common type of pediatric hip fracture (40–50%). Type III: Cervico-trochanteric fracture (25–35%). Type IV: Intertrochanteric fracture. This fracture between the greater and lesser trochanters accounts for 6–15% of all pediatric hip fractures and has the best outcome [5].
Complex femur fractures were classified by Juskovic et al. into three types (Tables 1 and 3). Type I: Combined fractures of the shaft and proximal femur, Type II: Segmental femur fractures, and Type III: Combined fractures of the shaft and distal femur [7].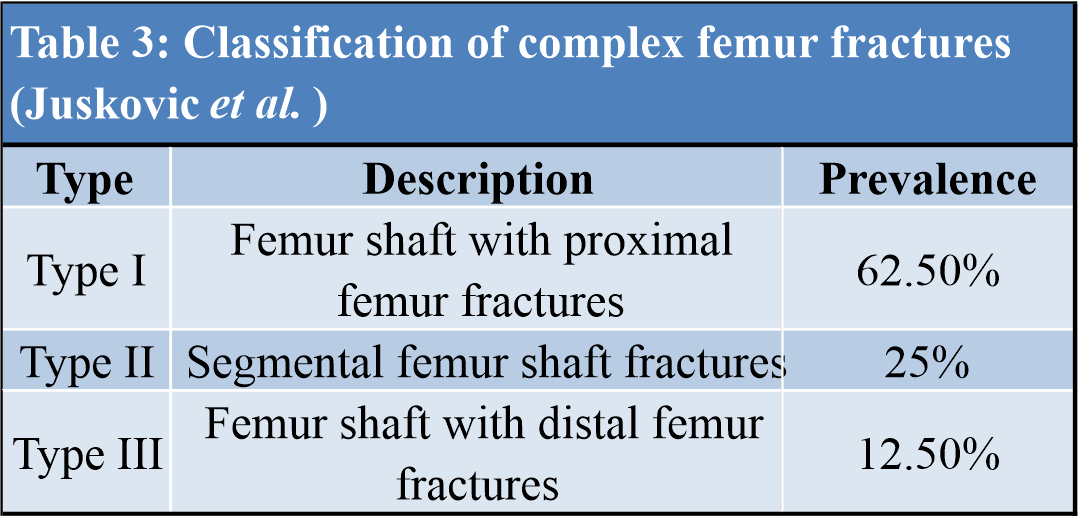
Ipsilateral femoral neck with shaft fracture is a very rare injury pattern with an incidence of about 0.7%. The rate of missed diagnosis is about 11–33% in adults and its further higher in pediatric patients as the children may be unable to report hip pain and often have multiple injuries [8]. Early operative stabilization of both fractures is the most favored modality of the treatment. Anatomical fixation with separate implants and a longer period of immobilization provides the best result. For undisplaced or minimally displaced fracture of neck closed reduction and percutaneous fixation can be done followed by definitive stabilization of the shaft. Open reduction is advocated for the displaced fractures. Depending upon the age of the patient and the fracture type smooth pins, cannulated screws and pediatric hip screw can be various options for the fixation on the neck fractures. Rigid fixation of the shaft using plate and screws is preferred over the flexible nails as these nails may be obstructed by the implants in the neck [2,9]. Our patient had Delbet Type IV fracture with a femur shaft at distal one-third, as it was minimally displaced closed reduction and fixation was done using smooth pins which were later connected to each other by L-rod for more stability and shaft was fixed rigidly with plate and screws.
Femur shaft fractures extending to the subtrochanteric area pose challenges due to the muscle forces acting (Fig. 4). The quadriceps and hamstring which span the proximal femur contribute to the femoral shortening. When the integrity of trochanters is maintained, the proximal fragment is externally rotated, flexed, and abducted due to pull by short external rotators, iliopsoas, and hip abductors, respectively. The hip adductors medialize the distal fragment of the shaft [10]. Closed reduction and fixation with elastic nails, minimally invasive submuscular plating, and open plate internal fixation are various surgical options for management. Fixation with TENS is more suitable in younger children with low body weight which has advantages of minimum blood loss and lower operating time. Loss of reduction mainly in length unstable fractures and requirement of prolonged immobilization are its important disadvantages. These disadvantages can be overcome by advancing the lateral nail into or just distal to the greater trochanter apophysis and advancing the medial nail into the femoral neck just short of the femoral physis. Anterograde nailing is preferred in length unstable fractures. Combination of retrograde and anterograde nailing was done in our case which add to the extra stability that has not been described in literature [11]. Older and obese children benefit from plate fixation. Open plating has disadvantages such as need for extensive soft tissue dissection, prolonged operating time, greater blood loss, and disruption of the periosteal blood supply increasing the risk of delayed union or non-union. Whereas, submuscular plating which functions as internal “external fixator” uses a minimally invasive technique. Fracture is reduced by indirect reduction techniques leading to minimum damage to the periosteal blood supply. Maximum biomechanical stability can be obtained longer plates and fewer screws which increases the working length of the plate. One of our patients with comminuted fracture extending into subtrochanteric was managed with this technique had excellent result [12,13].
Segmental fractures are very rare in children, they are caused by very high-velocity trauma accompanied by massive soft tissue damage, and most of the times they are open fractures. All open segmental fractures are best managed by thorough wound debridement and stabilization with an external fixator. Closed segmental fractures are best managed by TENS, submuscular plating, or intramedullary locking nails depending on the age and weight of the patient. These patients are best treated in fracture table using traction to achieve proper length, rotation and alignment. Sometimes segmental fractures may require open reduction to get the normal anatomical alignment. Plating can be good option in segmental fractures when the peri-trochanteric area is involved. Distal femur involvement occurs in about 12% of femur shaft fractures. An external fixator can be considered till the callus forms then the patient can be mobilized. Plate fixation can be a good option for management when there is enough space for screws between fracture and the physis [14,15].
Prospective studies with higher number of patients have been performed in adults, the same would be difficult in children as these are very uncommon injuries. Patients with complex femur shaft fractures require long-term follow-up to look for complications like limb length discrepancy, disruption of growth plate, angular or rotational deformities, muscle weakness, and re-fracture [16].
Complex femur fractures in children are rare injuries and are often difficult to treat. With proper pre-operative planning, following basics of fracture fixation, and use of appropriate implant for fracture fixation excellent functional results can be obtained. Long-term follow-up is a necessary in children as these fractures are susceptible for delayed complications.
Pediatric complex femur shaft fractures are rare. Peri-trochanteric fractures occurring along with femur shaft are often missed in the primary survey, as attention is directed to the shaft fracture and deformity. Thorough clinical and radiological assessment is required to avoid missing these fractures and the operating surgeon must have all kinds of implants options available for the optimal management of these fractures.
References
- 1.Flynn JM, Skaggs D. Femoral shaft fractures. In: Flynn JM, Skaggs D, Waters P, editors. Rockwood and Wilkins’ Fractures in Children. 9th ed. Philadelphia, PA: Wolters Kluwer; 2014. p. 987-1026. [Google Scholar | PubMed]
- 2.Agarwal A, Agarwal R, Meena DS. Ipsilateral femoral neck and shaft fracture in children. J Trauma 2008;64:E47-53. [Google Scholar | PubMed]
- 3.Barei DP, Schildhauer TA, Nork SE. Noncontiguous fractures of the femoral neck, femoral shaft, and distal femur. J Trauma 2003;55:80-6. [Google Scholar | PubMed]
- 4.Slongo TF, Audigé L. Fracture and dislocation classification compendium for children: The AO pediatric comprehensive classification of long bone fractures (PCCF). J Orthop Trauma 2007;21:S135-60. [Google Scholar | PubMed]
- 5.Lasanianos NG, Kankaris NK. Trauma and Orthopaedic Classification: A Comprehensive Review Edition. London: St. Springer-Verlag; 2015. p. 321-3. [Google Scholar | PubMed]
- 6.Harvey AR, Bowyer GW, Clarke NM. The management of paediatric femoral shaft fractures. Curr Orthop 2002;16:293-9. [Google Scholar | PubMed]
- 7.Juskovic A, Pesic G, Kezunovic M, Jeremic J, Bulatovic N, Dasic Z. Treatment of complex femoral fractures with the long intramedullary gamma nail. Serbian J Exp Clin Res 2019;20:337-41. [Google Scholar | PubMed]
- 8.Caldwell L, Chan CM, Sanders JO, Gorczyca JT. Detection of femoral neck fractures in pediatric patients with femoral shaft fractures. J Pediatr Orthop 2017;37:e164-7. [Google Scholar | PubMed]
- 9.Singh J, Mukhopadhaya J. Dilemma for fracture fixation of paediatric ipsilateral neck with shaft femur fracture. Indian J Orthop 2021;55:81-92. [Google Scholar | PubMed]
- 10.Seeley M, Caird MS, Li Y. Subtrochanteric femur fractures in children. In: Pediatric Femur Fractures. United States: Springer; 2016. p. 99-115. [Google Scholar | PubMed]
- 11.Li J, Rai S, Ze R, Tang X, Liu R, Hong P. The optimal choice for length unstable femoral shaft fracture in school-aged children: A comparative study of elastic stable intramedullary nail and submuscular plate. Medicine 2020;99:e20796. [Google Scholar | PubMed]
- 12.Xu Y, Bian J, Shen K, Xue B. Titanium elastic nailing versus locking compression plating in school-aged pediatric subtrochanteric femur fractures. Medicine 2018;97:e11568. [Google Scholar | PubMed]
- 13.Kanlic EM, Anglen JO, Smith DG, Morgan SJ, Pesantez RF. Advantages of submuscular bridge plating for complex pediatric femur fractures. Clin Orthop Relat Res 2004;426:244-51. [Google Scholar | PubMed]
- 14.Flynn JM, Schwend RM. Management of pediatric femoral shaft fractures. J Am Acad Orthop Surg 2004;12:347-59. [Google Scholar | PubMed]
- 15.Tornetta P, Ritz G, Kantor A. Femoral torsion after interlocked nailing of unstable femoral fractures. J Trauma 1995;38:213-9. [Google Scholar | PubMed]
- 16.Bassett WP, Safier S, Herman MJ, Kozin SH, Abzug JM. Complications of pediatric femoral shaft and distal physeal fractures. Instr Course Lect 2015;64:461-70. [Google Scholar | PubMed]





A report of Three Cases. Journal of Orthopaedic Case Reports 2021 October, 11(10): 34-38.
Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 Diagnostic Dilemma in a Distal Femoral Intramedullary Lesion: Enchondroma Mimicking Low-Grade Chondrosarcoma with Discordant Biopsy Findings: A Case Report
July 1, 2026 Diagnostic Dilemma in a Distal Femoral Intramedullary Lesion: Enchondroma Mimicking Low-Grade Chondrosarcoma with Discordant Biopsy Findings: A Case Report August 1, 2026 Complex Irreducible Dislocation of the Fourth Toe Proximal Interphalangeal Joint in a 5-year-old Boy Fixed by Soft Anchor: A Case Report
August 1, 2026 Complex Irreducible Dislocation of the Fourth Toe Proximal Interphalangeal Joint in a 5-year-old Boy Fixed by Soft Anchor: A Case Report February 1, 2025 Tuberculous Osteomyelitis of the Coracoid Process Presenting as Shoulder Pain: A Case Report
February 1, 2025 Tuberculous Osteomyelitis of the Coracoid Process Presenting as Shoulder Pain: A Case Report January 6, 2019 JOCR Best Reviewers for the Year 2018-2019
January 6, 2019 JOCR Best Reviewers for the Year 2018-2019