
Retained extensor function, strength, and movement on physical exam allows a conservative vs surgical approach to the point of care of a patient despite the extent of patellar tendon rupture and tibial avulsion fracture.
Dr. Baraa Musallam, Department of Surgery and Anesthesia, Midwestern University, 555 31st St, Downers Grove, IL 60515. E-mail: Musallam.40@gmail.com
Abstract
Introduction: This study highlights the case of a 75-year-old female patient with a history of bilateral knee replacements who presented with a subacute patellar tendon rupture that occurred after falling on her left knee.
Case Report: The patient had a left total knee replacement one year previously and came in for her one-year follow-up. She presented 3 weeks after her injury with a high-riding patella and a small tibial tubercle avulsion fracture on X-ray, yet she did not experience much pain nor any loss of active extension of her left knee. Despite the severity and subacute presentation of the patient’s patellar tendon injury, conservative measures that included physical and occupational therapy was recommended instead of surgery due to her paradoxical retention in gross function of her left knee.
Conclusion: Showcasing this patient’s case may provide further understanding of patellar tendon ruptures and tibial avulsion fractures, specifically factors that allow the patient to retain strength and extensor function in her knee to curb the need for surgery.
Keywords: Patellar Tendon, Tibial Avulsion Fracture, Osteoporosis
The purpose of this study was to highlight a unique subacute patellar tendon rupture case that presented with a small tibial tubercle avulsion and high riding patella, yet strength and full extension was present in her afflicted knee. The patella tendon is involved in extension of the knee and significant injury to the structure results in limitation in movement as well as deformity [1]. Tibial avulsion fractures are mostly seen in adolescents but are rare in adults [2]. Tibial avulsion fractures are associated with a patellar ligament rupture, and its treatment involves open reduction and internal fixation using screws, wires, or plates [2][3]. However, chronic injuries may require reconstruction of the patellar tendon due to marked deformity and limitations in motion [4][5]. Isolated patellar tendon ruptures are classified as acute or chronic in order to dictate the treatment of the injury; acute partial ruptures may be initially managed with conservative measures, but acute complete ruptures require primary surgical correction with suture anchoring if the ends of the tendon can be approximated [1][6]. The 75-year-old female patient with bilateral total knee replacement presented with a rare subacute patellar tendon rupture and tibial avulsion fracture case that was treated with conservative measures instead of the current recommendations to pursue surgery.
The patient is a 75-year-old female with a past medical history of hypertension, chronic obstructive lung disease, and emphysema. She has a past surgical history of bilateral total knee replacements: the right knee was replaced two years ago, and the left knee was replaced one year ago. There were no complications with either procedure. She presented for her yearly follow-up complaining of new onset of 1 out of 10 left knee pain with mild weakness and difficulty climbing stairs. The patient stated that she fell 3 weeks prior to her visit, complaining of moderate pain and swelling for 1-2 weeks that subsided substantially. She did not seek immediate medical attention. Before her fall, she was functioning normally with no pain. On exam, she had a slightly antalgic gait, ambulating without any assistive devices. She had full range of motion and strength of both hips, knees, and ankles with mild swelling and ecchymosis over the left tibial tubercle and minimal tenderness (as seen in Fig. 1-2). 
This activity focused on a unique patellar tendon rupture with a tibial avulsion fracture case that was presented in a subacute manner. Despite the presentation of the patient’s injury, she retained gross movement with extensor function and notable strength in her quadriceps. She also was able to ambulate and perform straight leg raises with her affected knee. Injuries to the extensor mechanism can involve fracture of the patella, tear of the patellar tendon, and tear of the quadriceps tendon [6]. Of the three injuries, patellar tendon ruptures comprise 0.5% of the population and have the lowest prevalence; quadriceps tendon tears have 1.3% prevalence and patella fractures occur twice as likely than patellar tendon ruptures [6]. Patellar tendon ruptures occur more likely in males over 40 than women, which may be due to males being physically stronger [6]. Women also experience protection from tendon rupture due to tendon laxity and hormonal changes during menses [6]. The patellar tendon can weaken due to chronic inflammation, medical conditions, and medications such as rheumatoid arthritis, systematic lupusery thematous, diabetes, chronic kidneys disease, fluoroquinolones, corticosteroids, etc. [9]. The medial and lateral patellar retinaculum provide minor stabilization to the patella, which can allow for extension as well as straight leg raises that are diminished after patellar tendon rupture [6] [9]. Avulsion fracture of the tibial tubercle is also a rare injury, more so with an associated patellar ligament rupture, which occurs most commonly in athletic adolescents due to an open physis [2] [3]. The first reported case was identified by Mayba in 1982 during which the mechanism of injury was theorized to occur through significant and continued contraction of the quadriceps muscle with a fixed foot or an external force causing contraction [3] [10]. The injury can present with a gap along the patella ligament and significant limitations in the extensor mechanism. Radiography provides a diagnostic clue for the injury, and diagnostic arthroscopy or MRI can assist with diagnosis [2]. The gold standard for the treatment of chronic ruptures is tendon reconstruction utilizing the contralateral patellar tendon, ipsilateral semitendinosus ligament, Achilles allograft, or artificial ligament [5]. Complications of patellar tendon rupture include dysfunction of the extensor mechanism, infection of the injury, and requirement of tendon reconstruction if surgery is performed after quadriceps tendon contraction [8]. The prognosis for patellar tendon rupture is good if treated early, which can be complicated with delayed diagnosis and intervention [7]. However, this patient paradoxically possessed gross extensor mechanism and straight leg raises with a complete subacute patellar tendon rupture and small tibial avulsion fracture that displaced the patella superiorly. As such, observation and physical and occupational therapy was successful. Immediate surgical repair as indicated by the literature was unnecessary. Further, due to the patient’s current menopausal state and rare injury, an osteoporosis workup was performed. Osteoporosis is a skeletal disorder associated with decreased bone strength due to a shift towards bone resorption and away from bone deposition [11]. Postmenopausal women are at an increased risk of osteoporosis due to decreased estrogen with 26% of women ≥65 years and >50% of women aged ≥85 year developing osteoporosis. Osteoporosis is associated with an increased risk of fracture due to decreased bone strength. Secondary causes of osteoporosis can occur due to different diseases, medications, and lifestyles, so a proper history, physical, and labs are needed to rule out other causes [12]. A fracture involving the vertebrae, proximal femur, distal forearm, or shoulder in a patient older than 50 years, with or without trauma, should be worked up for osteoporosis. The current guidelines by the World Health Organization (WHO) define osteoporosis as bone mineral density >2.5 SD below a young normal adult and osteopenia as bone mineral density between 1 and 2.5 SD below [14].. Bone mineral density is preferentially assessed by dual x-ray absorptiometry, which is used to assist with screening for osteoporosis in all women starting at the age of 65 as per American Association of Clinical Endocrinology (AACE) as well as to diagnose the condition [11]. Fracture Risk Assessment Tool Model (FRAX) is also needed to assess the 10-year probability of a hip fracture or a major osteoporotic fracture [12]. Risk factors for fragility fractures include prior fragility fracture, low estrogen levels, glucocorticoid therapy, low body mass index, all risk factors for falling, smoking, alcohol, and poor calcium intake. Hip and vertebral fractures are the most common fractures [11]. The current treatment for osteoporosis involves a pyramid approach that starts with calcium, vitamin D, physical activity, and fall prevention. Second line therapy addresses secondar y causes of osteoporosis. Finally, pharmaceuticals are effective in improving fracture risk in postmenopausal osteoporosis that include bisphosphonates, SERMs, calcitonin, and teriparatide [11]. However, AACE guidelines for pharmacological treatment of osteoporosis include women with postmenopausal osteoporosis, women with borderline-low bone mineral density (defined as a T-scores ≤1.5) if risk factors are present, or in women that fail nonpharmacologic therapy [15]. Denosumab, which is a human monoclonal antibody approved by the FDA that targets a key protein mediator of bone resorption, is used for the treatment of postmenopausal women with osteoporosis who are at a high risk for fracture by effectively reducing bone resorption, increasing bone mineral density, and reducing the rates of vertebral, nonvertebral, and hip fractures [13]. After assessment with and discussion with the patient with reference to the guidelines, denosumab was agreed upon as the initial treatment for her newly diagnosed postmenopausal osteoporosis.
The patient presented with a unique case of retained strength and extensor movement in her left knee despite a significant patellar tendon rupture and small tibial avulsion fracture following a subacute injury. The patient’s case demonstrates the effectiveness of conservative measures to sufficiently treat a patellar tendon rupture and tibial avulsion fracture with retained function. Perhaps, intact medial and lateral patellar retinaculum may be responsible for her preserved extensor mechanism. Additionally, physical and occupational therapy aided her recovery. Continued follow up is necessary to find the underlying causes for her presentation, which can further future treatments for patellar tendon ruptures with tibial avulsion fractures and similar knee pathologies.
The purpose of the case report is to highlight the patient’s unique presentation of a patellar tendon rupture and small tibial avulsion fracture with a retention of extensor function. The successful conservative treatment used for this patient may guide the point of care for similar injuries. The case report also serves to recommend treating the patient and their symptoms rather than their imaging.
References
- 1.Zhou M, Zou W. Application of suture bridge technique in the treatment of acute patellar ligament injury. Orthop J Sports Med. 2020 Sep 30;8(9 suppl7). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC75431 73/. [Google Scholar | PubMed]
- 2.Clarke DO, Franklin SA, Wright DE. Avulsion Fracture of the Tibial Tubercle Associated With Patellar Tendon Avulsion. Orthopedics. 2016 May 1;39(3). https://pubmed.ncbi.nlm.nih.gov/27088354/ [Google Scholar | PubMed]
- 3.Woolnough T, Lovsted G, MacDonald A, Johal H, Al-Asiri JA. Combined Tibial Tubercle Fracture With Patellar Tendon Avulsion in an Adult: A Rare Case and Novel Fixation Technique. Cureus. 2020 May 2;12(5):e7929. https://pubmed.ncbi.nlm.nih.gov/32494537/ [Google Scholar | PubMed]
- 4.Panagopoulos A, Antzoulas P, Giakoumakis S, Konstantopoulou A, Tagaris G. Neglected Rupture of the Patellar Tendon After Fixation of Tibial Tubercle Avulsion in an Adolescent Male Managed With Ipsilateral Semitendinosus Autograft Reconstruction. Cureus. 2021 Jun 1;13(6): e15368. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC82491 41/ [Google Scholar | PubMed]
- 5.Harato K, Kobayashi S, Udagawa K, Iwama Y, Masumoto K, Enomoto H, Niki Y. Surgical Technique to Bring Down the Patellar Height and to Reconstruct the Tendon for Chronic Patellar Tendon Rupture. Arthrosc Tech. 2017 Oct 16;6(5): e1897–e1901. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC57994 93/. [Google Scholar | PubMed]
- 6.Hsu H, Siwiec RM. Patellar Tendon Rupture. 2022 Apr 30. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan. https://www.ncbi.nlm.nih.gov/books/NBK513275/. [Google Scholar | PubMed]
- 7.Harato K, Kobayashi S, Udagawa K, Iwama Y, Masumoto K, Enomoto H, Niki Y. Surgical Technique to Bring Down the Patellar Height and to Reconstruct the Tendon for Chronic Patellar Tendon Rupture. Arthrosc Tech. 2017 Oct 16;6(5):e1897-e1901. https://pubmed.ncbi.nlm.nih.gov/29430392/. [Google Scholar | PubMed]
- 8.Volk WR, Yagnik GP, Uribe JW. Complications in brief: Quadriceps and patellar tendon tears. Clin Orthop Relat Res. 2014 Mar;472(3):1050-7. https://pubmed.ncbi.nlm.nih.gov/24338040/. [Google Scholar | PubMed]
- 9.Pope JD, El Bitar Y, Plexousakis MP. Quadriceps Tendon Rupture. 2022 May 1. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan. https://pubmed.ncbi.nlm.nih.gov/29494011/ [Google Scholar | PubMed]
- 10.Mayba II. Avulsion fracture of the tibial tubercle apophysis with avulsion of patellar ligament. J Pediatr Orthop. 1982 Aug;2(3):303-5. https://pubmed.ncbi.nlm.nih.gov/7130389/ [Google Scholar | PubMed]
- 11.Gass M, Dawson-Hughes B. Preventing osteoporosis-related fractures: an overview. Am J Med. 2006 Apr;119(4 Suppl 1):S3-S11. https://pubmed.ncbi.nlm.nih.gov/16563939/ [Google Scholar | PubMed]
- 12.Sözen T, Özışık L, Başaran NÇ. An overview and management of osteoporosis. Eur J Rheumatol. 2017 Mar;4(1):46-56. https://pubmed.ncbi.nlm.nih.gov/28293453/ [Google Scholar | PubMed]
- 13.Chitre M, Shechter D, Grauer A. Denosumab for treatment of postmenopausal osteoporosis. Am J Health Syst Pharm. 2011 Aug 1;68(15):1409-18. https://pubmed.ncbi.nlm.nih.gov/21785030/ [Google Scholar | PubMed]
- 14.World Health Organization. (1994). Assessment of fracture risk and its application to screening for postmenopausal osteoporosis : report of a WHO study group [meeting held in Rome from 22 to 25 June 1992]. World Health Organization. https://apps.who.int/iris/handle/10665/39142 [Google Scholar | PubMed]
- 15.Hodgson SF, Watts NB, Bilezikian JP, Clarke BL, Gray TK, Harris DW, et al. AACE Osteoporosis Task Force. American Association of Clinical Endocrinologists medical guidelines for clinical practice for the prevention and treatment of postmenopausal osteoporosis: 2001 edition, with selected updates for 2003. Endocr Pract. 2003 Nov-Dec;9(6):544-64. https://pubmed.ncbi.nlm.nih.gov/14715483/ [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above
August 1, 2026 Radiological Outcomes of Reamed Short Proximal Femoral Nailing in Intertrochanteric Fractures in Patients Aged 50 Years and Above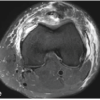 July 1, 2026 Bilateral Patellar Tendon and Unilateral Syndesmotic Injury in a Recreational Athlete
July 1, 2026 Bilateral Patellar Tendon and Unilateral Syndesmotic Injury in a Recreational Athlete July 1, 2026 Aseptic Discitis with Instability after Posterior Spine Surgery
July 1, 2026 Aseptic Discitis with Instability after Posterior Spine Surgery July 1, 2026 Retrograde Nailing of an Unstable Distal-Third Femoral Shaft Fracture Using Pure Indirect Reduction: A Case Report in Osteoporotic Bone
July 1, 2026 Retrograde Nailing of an Unstable Distal-Third Femoral Shaft Fracture Using Pure Indirect Reduction: A Case Report in Osteoporotic Bone