
This article throws light on the fact that certain unusual pathogens can also cause few common infections. Usage of appropriate diagnostic tests helps in targeted therapy and better patient outcome. Understanding the antibiotic susceptibility patterns also helps in looking out for future drug resistance mechanisms which have a huge role to play in deciding on empirical treatment.
Dr. Malavalli Venkatesh Bhavana, Department of Laboratory Medicine-Microbiology, Manipal Hospital, Bengaluru - 560 017, Karnataka, India. E-mail: bhavana224@gmail.com
Abstract
Introduction: Osteomyelitis is one of the infrequent presentations of Salmonella infection. Most of the case reports are among adult patients. It is very rare in children, and is most often associated with hemoglobinopathies or other predisposing clinical conditions.
Case Report: In this article, we present a case of osteomyelitis caused by Salmonella enterica serovar Kentucky, in a previously healthy 8-year-old child. Further, this isolate had an unusual susceptibility pattern; it showed resistance to the third-generation cephalosporins, akin to ESBL production among Enterobacterales.
Conclusion: Osteomyelitis caused by Salmonella does not have any specific clinical or radiological features, both in adult and pediatric age groups. A high index of suspicion, using appropriate testing methodologies and awareness about emerging drug resistance helps in accurate clinical management.
Keywords: Salmonella, pediatric, immunocompetant, osteomyelitis.
Salmonella in humans causes five distinct types of clinical infections. They can be categorized as enteric fever, septicemia without localization, focal disease, gastroenteritis, and the carrier state. Salmonella Typhi and Paratyphi are commonly associated with enteric fever and the carrier state. Non typhoidal Salmonella serovars are associated with gastroenteritis [1]. Osteomyelitis due to any of the any of these serovars is extremely rare, the incidence being around 0.8% of overall Salmonella infections. Seeding in the bones can occur during metastatic spread during septicemia or rarely, due to direct inoculation. As per literature, only 0.45% of all types of osteomyelitis are attributed to this organism [2]. Salmonella osteomyelitis usually affects immunocompromised hosts and those with thalassemia or sickle cell disease [3]. A few case reports of osteomyelitis in healthy adults are available, attributed to different serovars. The occurrence in a pediatric healthy patient is almost unheard of. We report a case of distal femur osteomyelitis due to Salmonella enterica serovar Kentucky in a healthy pediatric patient.
A male child, 8 years old, apparently normal previously, presented with complaints of pain in left knee from 4 weeks. This was insidious in onset, initially mild, and gradually progressed over time. He also complained of fever, swelling, and difficulty in movement. There was no history of any antecedent trauma. The parents recalled that he had mild diarrhea 4–5 weeks prior, which subsided with symptomatic medication. There was no history of cough, breathlessness, hemoptysis, weight loss, or night sweats. The child was treated locally with cefixime but it did not improve. The child was vaccinated appropriately as per age. On examination, there was tenderness and swelling of the left knee, with restriction of movement (Fig. 1). Systemic examination was unremarkable. There was no organomegaly. High resolution ultrasonography of left knee joint showed synovial thickening with soft-tissue edema in the left lower femoral epiphysis with minimal clear free fluid in the left prepatella bursa (Figs. 2 and 3). With a working diagnosis of the left distal femur osteomyelitis, the child was admitted for debridement. Basic laboratory workup was normal. Left knee debridement was done and serosanguinous fluid aspirated during the procedure was inoculated into a blood culture bottle and was sent to microbiology laboratory for culture. The bottle was loaded into BacT/Alert 3D (Biomeriux, France). The sample was also sent for cartridge based nucleic acid amplification test (CBNAAT) by for tuberculosis by Xpert/MTB Rif assay (Cephied, USA) and for Biofire filmarray test under blood culture identification panel (Biomeriux, France). CBNAAT was negative. Biofire filmarray test flagged positive for S. enterica and detected CTX-M. Culture performed by inoculation into blood culture bottle yielded gram negative bacilli. This was identified as Salmonella species, of the non-enteric variety (Fig. 4). Identification of the isolate was done by manual biochemical reactions as well as using VITEK 2 compact (Biomeriux, France). The isolate was also sent to ICMR-National Institute of Cholera and Enteric diseases, Kolkata, which is a WHO collaborating center for research and training on diarrheal diseases. The identification provided by them was S. enterica serovar Kentucky. (Ref number HK/01/2022/99/963). This isolate had a peculiar susceptibility pattern. It was susceptible to trimethoprim-sulfamethoxazole, but was resistant to all third generation cephalosporins and ciprofloxacin. It showed susceptibility to carbapenems. The child was treated with Inj. Meropenem, 380 mg (20 mg/kg/dose) intravenously, 3 times a day for 14 days along with analgesics as needed and other supportive measures. After 14 days, treatment was continued with oral trimethoprim-sulfamethoxazole at 10 mg/kg/day (for trimethoprim) for 4 weeks. The child recovered well.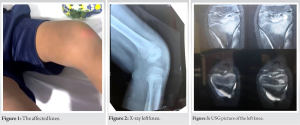
S. enterica is comprises of typhoidal strains (Serovar Typhi and Paratyphoid) and nontyphoidal strains. Bacteremia, which commonly occurs in enteric fever, can also happen in nontyphoidal gastroenteritis and that can lead to osteomyelitis. It is known to typically affect the diaphysis of long bones, most common being the femur and humerus. Other bones which can be involved are the lumbar vertebrae, tibia, radius, and ulna. The four most common causes of osteomyelitis among Salmonella species in adults are Salmonella Typhimurium, Salmonella Enteritidis, S. enterica sub spp. Arizonae and Salmonella Typhi [4,5,6]. Analysis of Salmonella Osteomyelitis by Stephanie and Schmalzle revealed that most of the osteomyelitis patients have an underlying predisposing condition such as sickle cell trait, thalassemia trait, and other hemoglobinopathes [7]. Most of these cases of osteomyelitis are reported in adult patients. A Nigerian study by Adeyokunnu and Hendrickse, analyzed 63 children with Salmonella osteomyelitis. They reported that in 61 children, this occurred in association with HbS either in the homozygous state or in heterozygous combination with other haemoglobins. Osteomyelitis was most prevalent during the first 2 years of life, and boys were more often affected than girls, as per this study [8]. In contrast, we report an absolutely healthy child, 8 years of age, with no history of any hemoglobinopathy. There was a history of diarrheal illness, which probably caused the hematogenous seeding of the organism in the bacteremic phase.A study by Vasileios et al. analyzed the incidence of osteomyelitis in previously healthy children. As per their literature search, there were 13 cases of S. Osteomyelitis in this population. Twelve of them were caused by non-typhoidal strains, with S. Enteritidis being the most common etiological agent. This study also emphasized that direct inoculation of surgical aspirates into blood culture bottles helped to grow the organism better as compared to direct inoculation onto agar media [9]. Another noteworthy feature in this case report is the susceptibility pattern. This isolate showed resistance to the third-generation cephalosporins, akin to ESBL production among Enterobacterales. This was also supported by the Biofire filmarray panel which detected CTX-M gene in this isolate. A study by Fu et al. analyzed the incidence of antimicrobial resistance in S. enterica serotype Enteritidis isolates in China from 2005 to 2014. As per this study, the number of cefepime resistant Enteritidis isolates is on the rise, and there is a strong possibility of dissemination of blaCTX–M–55-harboring plasmids among different species [10]. Another study by Zhang et al. looked at CTX-M-producing Salmonella isolates from raw meat and food animals. As per this study, 17.76% Salmonella isolates were ESBL-positive and CTX-M was the most prevalent type. They also proved the co-existence of PMQR genes which are responsible for fluoroquinolone resistance, along with blaCTX-M-55 in Salmonella isolates. As per the authors, coselection and genetic dissemination of resistance to fluoroquinolones and cephalosporins in Salmonella is was a possibility. As per their study, Salmonella Indiana, Salmonella Typhimurium, Salmonella Chester, and the few non-typeable isolates were the resistant strains [11]. We observed the same pattern in our patient as well. Multiple drug resistance in Salmonella can pose significant therapeutic challenges. As per literature, the most effective clinical management of confirmed Salmonella osteomyelitis is a employing a combined approach. It is recommended to undertake radical operative intervention like debridement, followed by targeted intravenous antibiotics based on susceptibility testing [12]. As per the European society of pediatric infectious diseases guidelines, treatment with antimicrobials needs to be continued for at least 3–4 weeks in a case of pediatric osteomyelitis. Longer course of therapy may be required for disease involving the pelvis or spinal column, infections caused by such unusual organisms, complicated infections, or those with slow response to treatment [13].
Salmonella osteomyelitis is to be considered as an important differential diagnosis, especially if the patient gives a prior history fever or diarrhea. Failure of empiric antibiotic therapy also provides a clue regarding this uncommon etiology. As the treatment duration in osteomyelitis is long, targeted therapy is crucial.
Awareness of uncommon causes of osteomyelitis is helpful. Practice of inoculating the surgical aspirate into blood culture bottles directly after aspiration certainly has better culture outcome. Culture will help in throwing light on the possible drug resistance in Salmonella which has crucial therapeutic implications. Awareness regarding the rare phenomenon of plasmid mediated cephalosporin resistance in different serovars also helps in planning appropriate treatment.
References
- 1.McAnearney S, McCall D. Salmonella osteomyelitis. Ulster Med J 2015;84:171-2. [Google Scholar | PubMed]
- 2.Sanchez AA, Mazurek MT, Clapper MF. Salmonella osteomyelitis presenting as fibrous dysplasia. A case report. Clin Orthop 1996;330:185-9. [Google Scholar | PubMed]
- 3.Miller SI, Da P. Salmonella species. In: Mandell GL, Douglas RG, Bennett JE, editors. Principles and Practice of Infectious Diseases. Pennsylvania: Churchill Livingstone; 2000. p. 2344-60. [Google Scholar | PubMed]
- 4.Arora A, Singh S, Aggarwal A, Aggarwal PK. Salmonella osteomyelitis in an otherwise healthy adult male: Successful management with conservative treatment: A case report. J Orthop Surg 2003;11:217-20. [Google Scholar | PubMed]
- 5.Declercq J, Verhaegan J, Verbist L, Lammens J, Stuyck J, Fabry G. Salmonella typhii osteomyelitis. Arch Orthop Trauma Surg 1994;113:232-4. [Google Scholar | PubMed]
- 6.Ispahani P, Slack RC. Enteric fever and other extraintestinal salmonellosis in University Hospital, Nottingham, UK, between 1980 and 1997. Eur J Clin Microbiol Infect Dis 2000;19:679-87. [Google Scholar | PubMed]
- 7.Stephanie S, Schmalzle SA. Salmonella enterica serovar Typhi osteomyelitis in a young adult with sickle cell and thalassemia traits: A possible association. IDCases 2018;15:e00478. [Google Scholar | PubMed]
- 8.Adeyokunnu A, Hendrickse RG. Salmonella osteomyelitis in childhood. A report of 63 cases seen in Nigerian children of whom 57 had sickle cell anaemia. Arch Dis Childhood 1980;55:175-84. [Google Scholar | PubMed]
- 9.Vasileios T, Christianna V, Ioannis M, Garyfallia S, Dimitrios P, Evangelia L, et al. Salmonella osteomyelitis in previously healthy children: Report of 4 cases and review of the literature. Pediatr Infect Dis J 2016;35:116-7. [Google Scholar | PubMed]
- 10.Fu Y, Xu X, Zhang L, Xiong Z, Ma Y, Wei Y, et al. Fourth generation cephalosporin resistance among Salmonella enterica Serovar Enteritidis isolates in Shanghai, China conferred by blaCTX-M-55 harboring plasmids. Front Microbiol 2020;11:910. [Google Scholar | PubMed]
- 11.Zhang CZ, Ding XM, Lin XL, Sun RY, Lu YW, Cai RM, et al. The emergence of chromosomally located blaCTX-M-55 in Salmonella from foodborne animals in China. Front Microbiol 2019;10:1268. [Google Scholar | PubMed]
- 12.Rayan F, Mukundan C, Shukla DD. A case of relapsing Salmonella osteomyelitis in a thalassaemia trait patient. J Orthop Traumatol 2009;10:31-3. [Google Scholar | PubMed]
- 13.Saavedra-Lozano J, Falup-Pecurariu O, Faust SN, Girschick H, Hartwig N, Kaplan S, et al. Bone and joint infections. Pediatr Infect Dis J 2017;36:788-99. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Bisphosphonate-Related Pathological Femoral Fracture in a Child with ACTG2-Related Intestinal Failure and Metabolic Bone Disease: A Case Report
August 1, 2026 Bisphosphonate-Related Pathological Femoral Fracture in a Child with ACTG2-Related Intestinal Failure and Metabolic Bone Disease: A Case Report August 1, 2026 Spiked Washer–Augmented Screw Fixation for Bilateral Tibial Tuberosity Avulsion Fractures in an Adolescent: A Case Report
August 1, 2026 Spiked Washer–Augmented Screw Fixation for Bilateral Tibial Tuberosity Avulsion Fractures in an Adolescent: A Case Report July 1, 2026 Concurrent Occurrence of Dysplasia Epiphysealis Hemimelica involving Lateral Malleolus and Sinus Tarsi: Rare Case with Review of Literature
July 1, 2026 Concurrent Occurrence of Dysplasia Epiphysealis Hemimelica involving Lateral Malleolus and Sinus Tarsi: Rare Case with Review of Literature July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor
July 1, 2026 Posterior Scapular Osteochondroma in a Pediatric Patient: An Uncommon Presentation of a Common Benign Tumor