
The article highlights the importance of regular bone health monitoring and fracture healing assessment for individuals undergoing phenytoin therapy, emphasizing the need for clinicians to remain vigilant and consider metabolic adjustments and providing close patient follow-up in epilepsy cases, also highlighting phenytoin’s potential positive therapeutic role in fracture management and need for further studies.
Dr. Tanmay Avhad, Department of Orthopaedics, TNMC and BYL Nair Charitable Hospital, Mumbai, Maharashtra, India. E-mail: tanmayavhad@gmail.com
Abstract
Introduction: Prolonged phenytoin (PHD) therapy in epileptics predisposes patients to deleterious effects on bone health causing osteoporosis; however, despite its known effect on wound healing, collagen and fibroblast proliferation, and osteogenic differentiation, its impact on fracture healing remains poorly researched, we, report two cases of early exuberant callus formation in long bone fractures in patients undergoing long-term PHD therapy.
Case Report: Two female patients with known seizure disorder on long-term PHD therapy experienced proximal humerus fractures after trivial trauma. Metabolic work-up revealed low serum calcium and Vitamin D3 levels with elevated ALP, serum osteocalcin, and iPTH. Despite planned surgery, both patients showed early exuberant callus formation post-trauma, leading to conservative management with successful outcomes.
Conclusion: Regular bone health monitoring is crucial for patients on long-term antiepileptic therapy, especially PHD users, to enhance treatment outcomes and address potential complications. Although the influence of PHD on fracture healing is uncertain, the cases presented hint at a potential beneficial correlation, indicating a need for more research in this domain.
Keywords: Phenytoin, fracture, bone turnover, union, callous.
Epilepsy stands as a considerable public health issue, impacting nearly 50 million individuals globally [1]. The negative impacts of antiepileptic drugs (AEDs) on bone health were initially documented almost 40 years ago and since then, increasing evidence has connected a range of biochemical, metabolic, and radiologic irregularities in bones to the utilization of AEDs [2,3]. Historically, there has been limited focus on the metabolic alterations linked to prolonged use of AEDs. Among these changes are the impact on bone metabolism, resulting in decreased bone mineral density and a heightened susceptibility to fractures. This situation is especially concerning for individuals with epilepsy, who already face an elevated risk of fractures due to other medication side effects (such as ataxia) and concurrent neurological impairments [4]. Phenytoin (PHT) has been a cornerstone in epilepsy treatment for over eight decades. Clinical observations have indicated that patients undergoing prolonged low-dose PHD therapy are predisposed to gingival hyperplasia due to increased proliferation of gingival fibrocytes and collagen [5]. Moreover, there is a notable rise in jawbone thickness and density, leading to patients exhibiting facial features resembling those of acromegaly [6]. Conversely, individuals subjected to long-term high-dose PHD therapy often develop osteoporosis, a condition more prevalent among postmenopausal women [7]. Historical documentation indicates that the antiepileptic medication PHD has been associated with promoting the formation of granulation tissue and facilitating wound healing [8]. Given the shared processes between wound healing and fracture healing, such as angiogenesis, collagen synthesis, and the release of various chemical mediators, it seemed reasonable to speculate that the positive impact of PHD on wound healing might also apply to fracture healing. However, research exploring the effects of PHD on fracture healing remains scarce [9]. We present a report of unusual cases of two patients of long bone fracture on long-term PHD therapy where exuberant callous formation was observed in early stages of fracture union to highlight the relation between the metabolic effects of these drugs on fracture union.
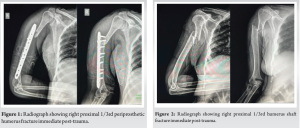
The first case, 45-year-old female, known case of epilepsy for two and half decades on PHD therapy had history of slip and fall at home leading to right midshaft humerus fracture for which the patient was managed surgically with plating. However, 1-month post-operative, the patient had a history of trivial trauma to the right arm. The clinical evaluation was consistent with the radiographic finding of the right periprosthetic proximal 1/3rd humerus shaft fracture without any distal neurovascular deficit (Fig. 1). In another case, a 56-year-old female, a known case of epilepsy for 28 years on PHD therapy, had a history of trivial trauma at home leading to right sided proximal 1/3rd humerus shaft fracture without distal neurovascular deficit as confirmed clinically and radiographically (Fig. 2).
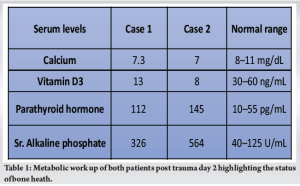
Considering the mode of injury both the patients were immobilized with chest arm strapping and planned for surgery along with a skeletal survey and metabolic workup to ascertain the case for pathological fractures in both patients. Workup suggested low levels of serum calcium, and Vitamin D3 with high levels of ALP, serum osteocalcin, and parathyroid hormone. (Table 1).
Therapeutic drug monitoring was performed for the AEDs and found to be higher than the recommended level due to non-compliance. Patients were worked up by the neurologist and anesthetist deeming the patient’s poor candidates for surgery due to their uncontrolled comorbidities. The repeat X-ray was taken 2-week post-trauma for both patients revealed exuberant callous at the fracture site which was unusual for the interval from trauma.
Radiological evidence of exuberant callous formation was noticed in both patients at the end of 10 days and 12-day post-trauma, respectively (Fig. 3 and 4). Clinical improvement in the form of decreased local tenderness and reduced mobility was noticed. Hence, patients were planned for a conservative line of management, Humerus Bracing with early mobilization was done along with metabolic corrections with Vitamin D3 and calcium supplements was planned along with regular follow-ups with serial radiographs. Both the patients showed an improvement in functional outcomes and good radiological union on serial follow-up and aggressive physical rehabilitation (Fig. 5).


The density of bones is governed by a delicate balance between bone formation and bone resorption. Initially, osteoblasts lay down an organic matrix, predominantly comprising Type I collagen (accounting for 90–95% of the matrix), alongside other proteins such as osteocalcin, osteonectin, osteopontin, and thrombospondin. Subsequently, mineralization occurs, during which the organic matrix is impregnated with hydroxyapatite, consisting of calcium and phosphorus. The concentration of these ions in the plasma and extracellular fluid dictates the rate at which hydroxyapatite forms and gets deposited. Maintaining adequate levels of calcium and phosphorus ions is crucial, as their deficiency can impede the mineralization process of the organic matrix [10]. Various biochemical markers can be assessed to gauge the overall rate of bone remodeling, which can be categorized into markers of bone formation originating from osteoblasts and markers of bone resorption representing breakdown products of osteoclastic activity [10]. Alkaline phosphatase serves as a marker for osteoblasts, with its cellular levels correlating with bone formation rates. In addition, circulating markers of bone formation include osteocalcin and Type I procollagen C-terminal peptide (PICP) [10]. During fracture healing, markers of bone formation indicate osteoblastic activity. Initially, Type-III collagen, a non-osteoblastic protein, is deposited, but it is later replaced by Type-I collagen as bone formation commences. Consequently, markers of bone healing include fragments of Type-I and Type-III procollagen released during the formation of Type-III collagen (such as Type-III collagen N-terminal propeptide, PIIINP), as well as those related to Type-I collagen (like Type-I collagen C-terminal propeptide, PICP, and Type-I collagen N-terminal propeptide, PINP). More specific indicators of osteoblastic activity encompass osteocalcin, the major non-collagenous protein of bone matrix, and the isoform bone-specific alkaline phosphatase, whose levels escalate during different phases of fracture healing [11]. The C-terminal extension peptide of Type I procollagen (PICP) is a putative serum marker of bone formation, and significant elevations have been seen in patients taking AEDs such as PHD) [12]. The effects of the above markers are not seen in osteoporosis as it is a state in which bone resorption exceeds formation. However, in fractured state, body promotes fracture healing by increasing osteoblastic activities and bone formation. In Patients receiving AEDs, high levels of bone formation markers indicating increased osteoblastic activity can affect fracture healing both patients sustained fractures following trivial trauma indicating severe osteoporosis due to long-term anti-epileptic treatment. Therapeutic drug monitoring revealed excessive plasma levels of antiepileptics; hence, body’s response for fracture union along with preexisting increased osteoblastic activity in response to long-term excess dose of antiepileptics seem to have acted synergistically in causing accelerated callous formation promoting union in both patients. According to research conducted by Frymoyer [13], fibula fractures in animals treated with DPH exhibited a statistically significant increase in the rate of union. A comparison of fracture healing trends between experimental and control animals indicated a consistent improvement in fracture healing among the experimental group throughout the entire observation period. In a study conducted by Donnell et al., utilizing a rat femur fracture model with PHD injection at fracture sites and tendon injuries, the subsequent evaluation revealed a higher count of inflammatory cells (P < 0.05) and blood vessels (P < 0.05) in the tendons treated with PHD compared to controls. However, there was no statistical difference observed in the stiffness or strength of the fractures treated with PHD compared to controls [14]. Mathew et al., in his study to evaluate the effect of local administration of PHD on fracture healing, showed a positive impact on fracture healing throughout the periosteal callus, particularly in hypervascular areas like the subperiosteal region. However, the influence of PHD on fracture healing is small and requires further research [15]. In a study by Yang et al., locally administered PHD was evaluated. Researchers assessed fracture healing using measures such as callus weighing, radiology, and histology. The findings revealed that both local and systemic use of PHD promoted fracture healing [16]. Tang et al. also showcased the beneficial impact of oral PHD in 40 cases involving closed fractures of the tibia and fibula. Their study revealed improved healing in the experimental group compared to controls by the conclusion of 3 months [17]. Nevertheless, this unique phenomenon of tissue and bone healing has been linked to the osteogenic differentiation of human bone marrow stem cells through the PI3K/Akt pathway [18]. This discovery holds significant potential for enhancing our comprehension of PHD’s impact on treatment strategies for fracture patients, potentially leading to the replacement of other antiepileptic medications known to adversely affect bone health.
Regular monitoring of bone health and fracture healing is crucial for individuals on long-term antiepileptic therapy, especially those receiving PHD, to mitigate potential effects on fracture healing and optimize treatment outcomes. Clinicians should consider metabolic corrections and close follow-up in patients with epilepsy to ensure timely intervention and promote better bone health. While the precise effect of PHD on fracture healing is not fully understood, the cases presented highlight a potential positive relationship, underscoring the need for further research in this area.
Regular monitoring of bone health is essential for patients on long-term antiepileptic therapy, particularly those taking PHD, to optimize treatment outcomes and mitigate potential complications. While the exact impact of PHD on fracture healing remains unclear, the presented cases suggest a possible positive relationship, emphasizing the need for further investigation in this area.
References
- 1.Scott RA, Lhatoo SD, Sander JW. The treatment of epilepsy in developing countries: Where do we go from here? Bull World Health Organ 2001;79:344-51. [Google Scholar | PubMed]
- 2.Kruse R. Osteopathies in antiepileptic long-term therapy (preliminary report). Monatsschr Kinderheilkd (1902) 1968;116:378-81. [Google Scholar | PubMed]
- 3.Sheth RD. Metabolic concerns associated with antiepileptic medications. Neurology 2004;63:S24-9. [Google Scholar | PubMed]
- 4.Petty SJ, O’Brien TJ, Wark JD. Anti-epileptic medication and bone health. Osteoporos Int 2007;18:129-42. [Google Scholar | PubMed]
- 5.Chacko LN, Abraham S. Phenytoin-induced gingival enlargement. BMJ Case Rep 2014;2014:bcr2014204670. [Google Scholar | PubMed]
- 6.Johnson JP. Acquired craniofacial features associated with chronic phenytoin therapy. Clin Pediatr (Phila) 1984;23:671-4. [Google Scholar | PubMed]
- 7.Ensrud KE, Walczak TS, Blackwell T, Ensrud ER, Bowman PJ, Stone KL. Antiepileptic drug use increases rates of bone loss in older women: A prospective study. Neurology 2004;62:2051-7. [Google Scholar | PubMed]
- 8.Talas G, Brown RA, McGrouther DA. Role of phenytoin in wound healing-A wound pharmacology perspective. Biochem Pharmacol 1999;57:1085-94. [Google Scholar | PubMed]
- 9.Mascres C, Marchand JF. The influence of sodium diphenylhydantionate on bone healing in the rat. J Biol Buccale 1983;11:137-52. [Google Scholar | PubMed]
- 10.Holick MF, Krane SM. Introduction to bone and mineral metabolism. In: Eugene B, Fauci A, Kasper D, Hauser S, Longo D, Jameson JL, editors. Harrison’s Principles of Internal Medicine. 15th ed. New York: McGraw-Hill; 2001. p. 2192-4. [Google Scholar | PubMed]
- 11.Cox G, Einhorn TA, Tzioupis C, Giannoudis PV. Bone-turnover markers in fracture healing. J Bone Joint Surg Br 2010;92:329-34. [Google Scholar | PubMed]
- 12.Dent CE, Richens A, Rowe DF, Stamp TC. Osteomalacia with long-term anticonvulsant therapy in epilepsy. Br Med J 1970;4:69-72. [Google Scholar | PubMed]
- 13.Frymoyer JW. Fracture healing in rats treated with diphenylhydantoin (Dilantin). J Trauma 1976;16:368-70. [Google Scholar | PubMed]
- 14.Donnell M, Nelligan M, Condron C, Murray P, Bouchier-Hayes D. The role of local phenytoin treatment in tendon and fracture healing. Orthop Procs 2006;88-B(Supp 2):283. [Google Scholar | PubMed]
- 15.Mathew M, Dhillon MS, Nagi ON, Sen RK, Nada R. The effect of local administration of phenytoin on fracture healing: An experimental study. Acta Orthop Belg 2006;72:467-73. [Google Scholar | PubMed]
- 16.Yang T, Meng Z, Yang Z. The effect of phenytoin in healing of fracture of rabbits. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 1997;11:149-52. [Chinese] [Google Scholar | PubMed]
- 17.Tang LL, Shen B, Yin Y. Clinical observation of phenytoin in promoting fracture healing. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 1999;13:343-5. [Chinese] [Google Scholar | PubMed]
- 18.Zhang Z, Shang W, Zhao X, Lin L. Phenytoin regulates osteogenic differentiation of human bone marrow stem cells by PI3K/Akt pathway. Regen Ther 2023;24:201-10. [Google Scholar | PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Plastic Bowing of the Pediatric Tibia is Extraordinarily Rare and Not Represented in the Literature, the Unicorn of Pediatric Fractures: A Case Report
August 1, 2026 Plastic Bowing of the Pediatric Tibia is Extraordinarily Rare and Not Represented in the Literature, the Unicorn of Pediatric Fractures: A Case Report August 1, 2026 Open Reduction and Internal Fixation of Gartland Type III Supracondylar Humerus Fractures Using the Posterior Paratricipital Approach: A Case Series
August 1, 2026 Open Reduction and Internal Fixation of Gartland Type III Supracondylar Humerus Fractures Using the Posterior Paratricipital Approach: A Case Series April 1, 2026 Novel Technique for Fracture Non-Union in Children – A Case Report
April 1, 2026 Novel Technique for Fracture Non-Union in Children – A Case Report April 1, 2026 Comparing Locking Compression Plate and Retrograde Nail in the management of distal femur fracture: A Comprehensive Analysis
April 1, 2026 Comparing Locking Compression Plate and Retrograde Nail in the management of distal femur fracture: A Comprehensive Analysis