
• Traditional bone-setting practice may have devastating consequences to limb and endanger life • Supervised training of bone setters is the need of the hour • Raise awareness among healthcare providers, policymakers and the community about the risks associated with unscientific fracture management
Dr. Purushotham Lingaiah, Department of Orthopaedics, All India Institute of Medical Sciences, Mangalagiri, Andhra Pradesh, India. E-mail: puru@aiimsmangalagiri.edu.in
Abstract
Introduction: The traditional practice of bone setting is more prevalent in developing countries, including India. These traditional practices of fracture management lead to numerous limb-threatening complications like non-union, pressure necrosis, gas gangrene, nerve palsies, necrotising fasciitis, and most importantly, compartment syndrome. Approximately 75% of acute compartment syndrome (ACS) occurs due to an underlying long bone fracture, most commonly fractures of the tibia, followed by forearm fractures. We report a case of the rare occurrence of compartment syndrome of the arm, highlighting the challenges in its management, and also raise awareness about traditional bone setting and its complications.
Case Report: A 35-year-old male patient with a right distal one-third humerus shaft fracture and a non-displaced radial neck fracture, treated by a traditional bone setter, presented with complaints of swelling and pain in the arm 4 days after the injury. On clinical and radiological evaluation, the patient was diagnosed with compartment syndrome of the arm resulting in right radial nerve palsy and pressure necrosis of superficial muscles with skin blisters. Peripheral pulses were feeble. Debridement with external fixation and radial nerve exploration was performed. Split skin grafting was done for wound coverage. A Sarmiento functional cast was applied once the wounds healed. The patient had a satisfactory functional outcome at the 1-year follow-up.
Conclusion: This case highlights the potentially devastating consequences of traditional bone-setting practices, which remain prevalent in developing countries. The occurrence of ACS with subsequent radial nerve palsy following non-operative manipulation of a humerus fracture underscores the urgent need for early recognition, prompt referral, and appropriate orthopaedic intervention. Reporting this case is important as it not only contributes to the limited literature on upper limb compartment syndrome secondary to traditional fracture treatment but also serves to raise awareness among healthcare providers, policymakers, and the community about the risks associated with unscientific fracture management practices.
Keywords: Upper extremity fractures, traditional bone setting, compartment syndromes, pressure ulcer, ischemia, orthopedic procedures.
Traditional bone setting (TBS) is an ancient form of healthcare practised in many cultures around the world, especially in parts of Africa, Asia, and rural communities elsewhere. TBS is a non-formal method of managing fractures, dislocations, sprains, and joint injuries. It involves the manual manipulation, alignment, and splinting of bones and joints without formal orthopaedic training. Traditional bone setters are usually community healers who inherit knowledge from older generations or learn through apprenticeship [1]. The practice of TBS is highly unregulated and lacks fundamental scientific principles of fracture management, infection prevention, and control [2]. These lead to numerous complications like malunion, non-union, pressure necrosis, gas gangrene, nerve palsies, necrotising fasciitis, and most frequently, compartment syndrome due to tightly placed splints. These limb-threatening conditions pose a significant challenge to the orthopaedic surgeons practising in these regions [3]. Acute compartment syndrome (ACS) is a condition characterised by increased pressure within the closed osteofascial compartment, amounting to impaired local vascular perfusion. Approximately 75% of ACS is predisposed to an underlying long bone fracture, most commonly fractures of the tibia and forearm. It can occur with any underlying condition that restricts the intra-compartmental space or increases the fluid in the intra-compartmental space. Other causes of ACS include burns, vascular injuries, crush injuries, thrombosis, improperly placed casts or splints, tight circumferential bandages, and poor positioning during surgeries [4]. Although ACS is routinely documented, ACS involving the arm is not frequently encountered [5]. We present a rare case of ACS of the arm in a 35-year-old male with associated fractures of the right distal one-third humerus fracture, treated by a traditional bone setter using herbal paste and a compression bandage. This case highlights the potentially devastating consequence of traditional bone-setting practice, which remains prevalent in developing countries. Limb salvage was achieved by timely intervention.
A 35-year-old male suffered a closed injury to the right elbow with associated pain, swelling, and inability to move the elbow, following a road traffic accident. The patient visited a traditional bone setter (Quack), where initial treatment was given. The treatment included twice-daily application of a herbal paste (composition details not available) followed by a compressive bandage. On the 4th day of the treatment, the patient developed severe pain in the distal arm, blisters on the volar aspect of the arm and elbow, and an inability to move the wrist. The patient presented to our emergency department with the above complaints. On examination, there was a diffuse swelling over the entire right upper limb with multiple blisters on the ulnar and volar aspect of the distal arm and elbow. Skin over this region was necrosed with no sensations (Fig. 1).

Figure 1: Clinical presentation showing skin necrosis and blisters on the distal arm.
The arm compartment was tense. There was wrist drop and sensory loss in the dorsal radial digits, suggesting radial nerve palsy. The pulse was low volume in comparison to the contralateral side. There were contusions over the elbow region with bony crepitus suggestive of an underlying fracture. He was haemodynamically stable and afebrile. Investigations – A radiograph of the elbow revealed a fracture of the distal shaft of the humerus with a non-displaced fracture of the radial head (Fig. 2).
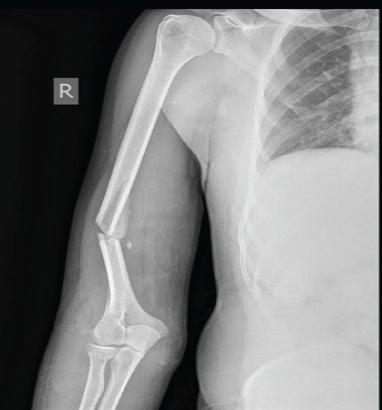
Figure 2: Plain radiograph showing fracture of the distal shaft humerus and radial neck.
In view of feeble peripheral pulsations, right upper limb arterial and venous Doppler was performed, which revealed normal colour uptake with maintained velocities over the distal right radial and ulnar arteries (Fig. 3).
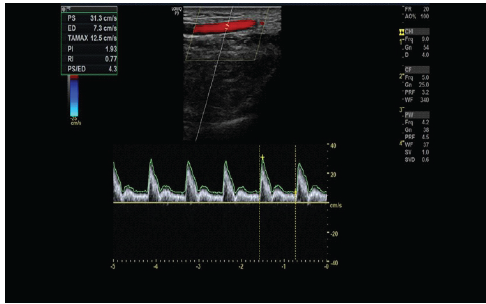
Figure 3: Color Doppler showing normal waveform and flow velocities in the radial artery.
Based on the clinical and radiological findings, a diagnosis of ACS of the arm with radial nerve palsy resulting from faulty fracture treatment was made. Management – Fasciotomy of the arm, debridement of the wound, radial nerve exploration and stabilisation with external fixation were performed (Fig. 4).

Figure 4: External fixation of the arm.
The radial nerve was contused with no discontinuity. Post-operative regular dressings resulted in healthy granulation tissue. Skin grafting was done after 2 weeks. Follow-up at 2 months showed healed skin lesions and a well-formed callus at the fracture site, and the wrist extension recovered. External fixation was removed, and a Sarmiento functional cast till fracture healing was applied (Fig. 5). Outcome – At 1 year follow-up, the fracture was consolidated (Fig. 6). The patient regained a full range of movement at the shoulder and elbow. The radial nerve had completely recovered.

Figure 5: Well-healed wound.

Figure 6: Radiologically healed fracture with no signs of infection at 1 year follow-up.
In an era of advanced orthopaedic care, TBS is still commonly followed in many communities worldwide, especially in developing countries in Asia, South America, and Africa. In India, with abundant medical institutions and the best advanced medical care, about 60% of the traumas are treated by TBS [6]. This practice involves using wooden straps and casts to immobilise and stretch the injured limb, often resulting in complications such as non-union, mal-union, infections, and, most importantly, compartment syndromes. It often involves realigning bones by hand, followed by immobilisation using herbal medicated splints/sticks [7]. Despite limitations in traditional practices, various social and peer factors contribute to the support of traditional medicine.
- Cost is usually much lower than modern orthopaedic care.
- Accessibility in rural areas where hospitals are far.
- Cultural trust and family traditions.
ACS is a frequent complication seen after unscientific means of fracture management. It is an acute limb-threatening condition and, if untreated, can be life-threatening by causing tissue necrosis, permanent functional impairment, possible renal failure, and death due to acute rhabdomyolysis. They are predominantly seen in the lower limb; while most literature focuses on lower-extremity compartment syndrome, involvement of the upper extremity – particularly the arm and forearm – represents a significant clinical challenge due to its relative rarity and potential for delayed diagnosis [8]. Compartment syndrome of the arm requires prompt recognition and intervention to prevent permanent functional impairment. There are classically five P’s associated with compartment syndrome: pain, paraesthesia, pallor, paralysis, and pulselessness [9]. Due to a low index of suspicion and non-classical presentation, ACS of the arm is likely to be missed. Our case did not show all the classical symptoms. However, he had exponential pain over the site of fracture, pressure necrosis of skin, and radial nerve palsy. ACS of the arm is extremely rare and has not been frequently reported. The probable reason could be the pliability of compartments of the arm [10]. Hence, the presence of an additional factor, such as external compression, vascular injury, and crush injury, could be found in these cases. Our case had a road traffic accident, sustaining injuries to his right upper limb. The compressive bandage treatment by a traditional bone setter, along with wooden straps to stabilise and immobilise the injured limb, led to ACS. Clinically and radiologically, the case was diagnosed as multiple upper limb fractures (right distal one-third humerus shaft fracture and a non-displaced radial neck fracture) with radial nerve palsy, pressure necrosis, and ACS. This underscores the need for early evaluation and management of the fractures under a proper orthopaedic setting rather than TBS, since bone healing and the subsequent events are dependent on the duration of presentation and the targeted management. There are multiple causes of compartment syndrome, but this case report describes a unique scenario where an external TBS caused compartment syndrome. Untreated or delayed compartment syndrome can result in severe complications, including muscle necrosis, nerve injury, infection, and Volkmann’s ischaemic contracture. Systemic complications such as rhabdomyolysis and renal failure have also been reported in severe cases. Timely fasciotomy and decompression can prevent these complications of ACS [11]. Our patient underwent fasciotomy, debridement, bony stabilisation with external fixation, and radial nerve exploration. Postoperatively, the patient improved symptomatically and was discharged in a haemodynamically stable condition. This case illuminates the extremes of outcomes an ill-managed fracture can present with and the indispensable need to create awareness among the patients and the orthopaedic surgeons for effective handling of the patient and improved patient care. Wound management following fasciotomy often requires delayed closure or skin grafting. Prognosis depends largely on the timing of diagnosis and intervention. Patients treated early typically recover good limb function, whereas delays beyond several hours significantly increase the risk of long-term impairment.
Traditional bone-setting practices can have potentially devastating consequences, as seen in this case of humeral shaft fracture complicated by ACS, radial nerve palsy, and pressure necrosis. Swift surgical intervention ensured limb salvage, but the case serves as a stark reminder that unscientific fracture management endangers lives and demands urgent awareness, early referral, and decisive orthopaedic care. Reporting this case is important as it not only contributes to the limited literature on upper limb compartment syndrome secondary to traditional fracture treatment but also serves to raise awareness among healthcare providers, policymakers, and the community about the risks associated with unscientific fracture management practices.
The treatment by quacks can be detrimental to the limb and life of a patient. Early referral, prompt recognition, and treatment of compartment syndrome with a guarded prognosis may serve as an optimal approach in such cases.
References
- 1. Hamad H, Omer D, Abdelnabi R, Abdelgaleel A. Motives and consequences of musculoskeletal injuries management at traditional bone setting centers rather than hospital orthopedic departments in Khartoum, Sudan 2020. Afr Health Sci 2024;24:384-94. [Google Scholar] [PubMed]
- 2. Nandeesh S, Sharma A, Madhuchandra P, Koushik, Raju KP, Kumar AV, et al. A study on complications seen in musculoskeletal injuries treated by traditional bone setters. J Popul Ther Clin Pharmacol 2025;32:e10250. [Google Scholar] [PubMed]
- 3. Touré L, Bah A, Djiré I, Sidiki SA, Sékou S, Diarra Y, et al. Is traditional bone setting a risk factor for postoperative complications in limb fractures? A prospective case-control study from Mali. Int J Orthop Sci 2025;11:184-6. [Google Scholar] [PubMed]
- 4. Machaku D, Lodhia J, Nangole A, Chilonga K, Massawe H. Loss of a limb: A consequence of traditional bone setting. Int J Surg Case Rep 2025;130:111237. [Google Scholar] [PubMed]
- 5. Via AG, Oliva F, Spoliti M, Maffulli N. Acute compartment syndrome. Br Med Bull 2015;115:25-36. [Google Scholar] [PubMed]
- 6. Girish P, Varman JM, Gopinath G, Khader FA. Mismanagement by native bone setters and its complications – An observational and retrospective study. Indian J Orthp Surg 2020;6:316-21. [Google Scholar] [PubMed]
- 7. Palo N, Chandel S, Malik C, Shukla A, Choudhary GN, Govind N, et al. Traditional bonesetters clinics: Prospective trends and work assessment on 915 bonesetters operating in parts of Uttar Pradesh and Haryana, India. J Orthop Dis Traumatol 2023;6:194-19. [Google Scholar] [PubMed]
- 8. Maeckelbergh L, Colen S, Anné L. Upper arm compartment syndrome: A case report and review of the literature. Orthop Surg 2013;5:229-32. [Google Scholar] [PubMed]
- 9. Hanandeh A, Mani VR, Bauer P, Ramcharan A, Donaldson B. Identification and surgical management of upper arm and forearm compartment syndrome. Cureus 2019;11:e5862. [Google Scholar] [PubMed]
- 10. Balogun MJ, Morhason-Bello JO, Olusola IK. Peadiatric amputation from traditional bone setters’ gangrene in Ibadan: A malady. Int J Res Orthop 2024;10:1137-41. [Google Scholar] [PubMed]
- 11. Venkatesh Kumar N, Aravind Kumar SM, Ganapathi V, Sairamakrishnan S. Issues in management of fractures complicated by compartment syndrome. Int J Orthop Sci 2017;3:326-9. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Generalized Tetanus Following Traditional Manipulation of an Open Supracondylar Humerus Fracture in a Child: A Rare Case Report
August 1, 2026 Generalized Tetanus Following Traditional Manipulation of an Open Supracondylar Humerus Fracture in a Child: A Rare Case Report August 1, 2025 Vulvar Pressure Ulcer – An Inadvertent Complication of Thomas Splint: Case Report
August 1, 2025 Vulvar Pressure Ulcer – An Inadvertent Complication of Thomas Splint: Case Report April 1, 2025 Reconstructive Surgical Management of Vasopressor-Ischemia Related Distal Extremity Loss
April 1, 2025 Reconstructive Surgical Management of Vasopressor-Ischemia Related Distal Extremity Loss November 10, 2023 Acute digit ischemia due to a ruptured digital collateral artery aneurysm in a patient of hemophilia: A case report
November 10, 2023 Acute digit ischemia due to a ruptured digital collateral artery aneurysm in a patient of hemophilia: A case report