
Total shoulder arthroplasty combined with latissimus dorsi and teres major transfer may serve as a viable reconstructive option for patients with osteoarthritis and irreparable subscapularis tears.
Dr. Chang Hee Baek, Department of Orthopaedic Surgery, Yeosu Baek Hospital, Jeollanam-do, Republic of Korea/50, Yeoseo 1-ro, Yeosu-si, Jeollanam-do, Republic of Korea. Phone: +82-1877-5075; Fax: +82-61-653-3008. E-mail: yeosubaek@gmail.com
Abstract
Introduction: Anatomic total shoulder arthroplasty (TSA) is the standard treatment for glenohumeral osteoarthritis with an intact rotator cuff; however, irreparable subscapularis tears often contraindicate TSA due to compromised anterior stability. Reverse TSA (RTSA) is commonly performed in such cases but alters native biomechanics and may limit rotational strength.
Case Report: A 69-year-old female presented with chronic shoulder pain and functional limitation. Imaging revealed advanced glenohumeral osteoarthritis with a full-thickness irreparable subscapularis tear, while the posterosuperior rotator cuff remained intact. The patient underwent anatomic TSA combined with anterior latissimus dorsi and teres major (LDTM) tendon transfer and partial subscapularis repair. At the 4-year follow-up, significant improvements were observed in pain and function, with the Visual Analogue Scale improving from 5 to 1, the Constant score from 59 to 82, and the American Shoulder and Elbow Surgeons score from 56 to 81. Range of motion and strength improved across all planes. Radiographs demonstrated stable implant fixation without complications, and sonography confirmed an intact tendon transfer. The patient returned to daily activities without pain and reported high satisfaction.
Conclusion: Anatomic TSA combined with anterior LDTM tendon transfer may be a viable alternative to RTSA in selected patients with glenohumeral osteoarthritis and irreparable subscapularis tears.
Keywords: Total shoulder arthroplasty, subscapularis tear, latissimus dorsi and teres major tendon transfer, rotator cuff insufficiency, shoulder stability.
Anatomic total shoulder arthroplasty (TSA) is the preferred treatment for patients with glenohumeral osteoarthritis and an intact rotator cuff, aiming to restore native joint biomechanics and preserve shoulder strength and function [1]. However, in cases where the subscapularis tendon is irreparably torn or severely compromised, TSA is typically contraindicated due to the essential role of the subscapularis in anterior shoulder stability and joint function [2,3,4,5]. In such scenarios, reverse TSA (RTSA) is often considered a safer alternative, as it does not depend on rotator cuff integrity for function [6]. Nevertheless, RTSA alters the native biomechanics of the shoulder by shifting the centre of rotation medially and inferiorly, relying predominantly on the deltoid for function [7]. This can result in reduced rotational strength and functional limitations, especially in active patients. For selected patients with isolated subscapularis deficiency but preserved posterosuperior rotator cuff integrity, reconstructive tendon transfers may allow the use of TSA while maintaining anatomic alignment and restoring dynamic anterior stability. The latissimus dorsi and teres major (LDTM) tendon transfer, traditionally utilised for managing irreparable subscapularis tears in the native shoulder, can be adapted for anterior transfer to serve as a subscapularis substitute in the setting of TSA [8,9,10,11]. When combined with TSA, this approach may offer a viable alternative to RTSA in carefully selected cases, particularly in younger or more active patients seeking preservation of native biomechanics. This report presents a case of anatomic TSA in a 69-year-old female patient with primary glenohumeral osteoarthritis and a severe subscapularis tear, in which anterior LDTM tendon transfer combined with partial subscapularis repair was performed to restore anterior stability and facilitate anatomic reconstruction.
Case description:
A 69-year-old right-hand-dominant female presented with chronic left shoulder pain and progressive functional impairment. Her primary complaints included difficulty with forward elevation (FE) and internal rotation (IR) due to pain, especially during daily activities as a housewife, such as cleaning and washing dishes. She reported increasing pain and difficulty with food preparation, toileting, and personal hygiene, all of which significantly impacted her quality of life. Physical examination revealed FE of 150°, abduction (ABD) of 140°, external rotation (ER) of 50°, and IR to the back, reaching the L4 vertebral level. Strength measurements were as follows: FE 23.1 N, ABD 24.1 N, ER 21.6 N, and IR 14.6 N. Patient-reported outcome measures showed moderate functional limitations and pain, with a visual analogue scale (VAS) score of 5/10, a Constant score of 59/100, and an American Shoulder and Elbow Surgeons (ASES) score of 56/100. Plain radiographs demonstrated advanced glenohumeral osteoarthritis characterised by joint space narrowing, without superior humeral head migration or acromialisation (Fig. 1).
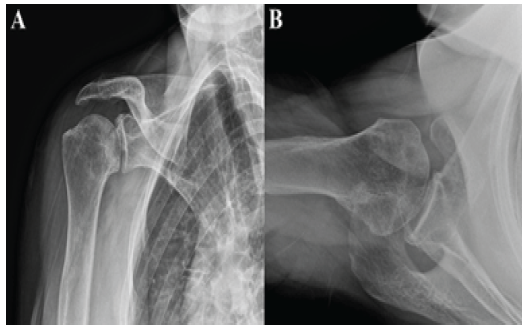
Figure 1: Pre-operative plain radiographs of the right shoulder. (a) Anteroposterior view. (b) Axillary view.
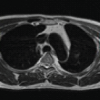
Magnetic resonance imaging revealed cartilage defects in the humeral head and glenoid wear, with a full-thickness tear of the subscapularis tendon showing medial retraction and Goutallier et al. [12] grade III fatty infiltration. The supraspinatus and infraspinatus tendons were intact, with preserved muscle quality and no retraction or atrophy (Fig. 2).
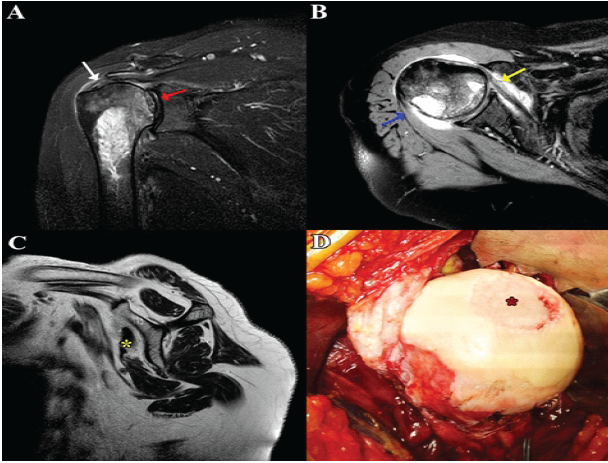
Figure 2: Pre-operative magnetic resonance imaging (MRI) of the right shoulder and intraoperative findings. (a) Coronal MRI showing an intact supraspinatus tendon (white arrow) and joint space narrowing with cartilage wear (red arrow). (b) Axial MRI demonstrating a subscapularis tear (yellow arrow) and intact infraspinatus tendon (blue arrow). (c) Sagittal MRI illustrating a severely degenerated subscapularis tear with muscle atrophy (yellow asterisk). (d) Intraoperative photograph showing the humeral head with a central cartilage defect (red asterisk).
Given the advanced osteoarthritis combined with an isolated subscapularis tear and preserved posterosuperior rotator cuff integrity, an anatomical TSA was planned. To restore anterior shoulder stability and function, an anterior LDTM tendon transfer was performed along with partial subscapularis repair.
Surgical procedure:
The patient was positioned in the beach-chair position under general anaesthesia. A standard deltopectoral approach was used, with inferior extension of the incision to the lower border of the pectoralis major (PM) to provide adequate exposure for the LDTM tendon transfer. The long head of the biceps tendon was tenotomised, and the remnant of the torn subscapularis was released and tagged with traction sutures for partial repair. Dissection was carried out along the superior and inferior borders of the PM, which was retracted using a Kolbel retractor to expose the humeral insertion of the LDTM unit. The LDTM tendon was harvested as a single unit, preserving the continuity between the latissimus dorsi and teres major tendons. The tendinous edge was whipstitched with No. 2 non-absorbable sutures in Krakow fashion. Medial release was performed using sterile gauze to free adhesions and improve tendon excursion while avoiding injury to the radial nerve. The harvested tendon was then passed beneath the PM and directed anteriorly toward the greater tuberosity, with care to avoid excessive medial traction that could endanger the radial nerve. Following tendon harvest, a standard anatomic TSA (The Comprehensive® Total Shoulder System; Warsaw, IN, USA) was performed. The humeral head was resected at the anatomic neck with an inclination angle of 132.5° and 20° of retroversion. The humeral canal was reamed to accommodate a press-fit stem. Glenoid preparation involved the removal of residual cartilage and the correction of minor version abnormalities. A standard polyethylene glenoid component was implanted in a neutral version with concentric reaming to optimise conformity and restore joint line anatomy (Fig. 3a). For tendon fixation, six suture tunnels were drilled into the lateral aspect of the greater tuberosity, posterior to the bicipital groove, to facilitate partial subscapularis repair. Two additional tunnels were created inferiorly to secure the transferred LDTM tendon (Fig. 3b). Loop sutures were passed through each tunnel, and the humeral stem was inserted through the preplaced loops. The sutures from the LDTM tendon were passed through the inferior two tunnels. After humeral stem impaction, the loops were pulled taut around the stem to achieve secure fixation (Fig. 3c). With the arm positioned in approximately 45° of abduction and full IR, the LDTM tendon was fixed to the greater tuberosity using the preplaced sutures. Adequate tensioning and fixation were confirmed by cycling the shoulder through internal and ER. Finally, a partial repair of the remnant subscapularis tendon was performed using the traction sutures to augment anterior stability and reinforce the tendon transfer construct (Fig. 3d).
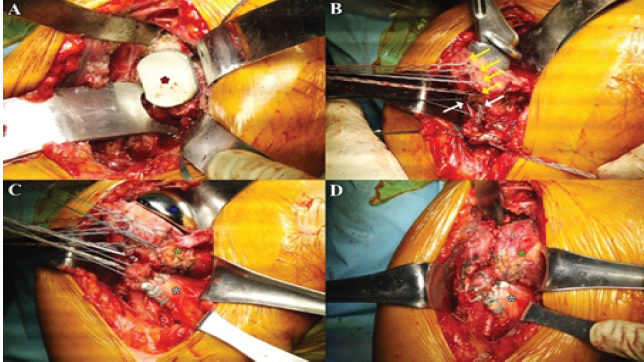
Figure 3: Surgical procedure. (a) Insertion of the glenoid component (red asterisk). (b) Sutures placed in tunnels for partial subscapularis repair (yellow arrow) and additional tunnels created for latissimus dorsi and teres major tendon transfer (white arrow). (c) After insertion of the humeral component (blue asterisk), the prepared latissimus dorsi and teres major tendon (white asterisk) and the subscapularis (yellow asterisk) are positioned for final fixation. (d) Final appearance after partial subscapularis repair (yellow asterisk) and latissimus dorsi and teres major transfer (white asterisk).
Post-operative outcome:
At 4 years post-operative follow-up, the patient showed marked improvement in pain, function, and strength, with high overall satisfaction. Patient-reported outcomes improved substantially: VAS decreased to 1/10, Constant score increased to 82/100, and ASES score improved to 81/100. Range of motion was preserved or improved, with FE of 160°, ABD of 160°, ER of 50°, and IR reaching the L1 vertebral level. Strength assessments increased in all planes: FE 26.2 N, ABD 27.1 N, ER 24.6 N, and IR 25.1 N. Radiographs confirmed stable fixation of humeral and glenoid components, without loosening, subsidence, or implant-related complications (Fig. 4). Sonography confirmed intact LDTM tendon transfer with no detachment. The partially repaired subscapularis remained well-positioned without retraction. Functionally, the patient resumed daily housework, including cooking and dishwashing, without pain, reporting consistent satisfaction with the surgical outcome.
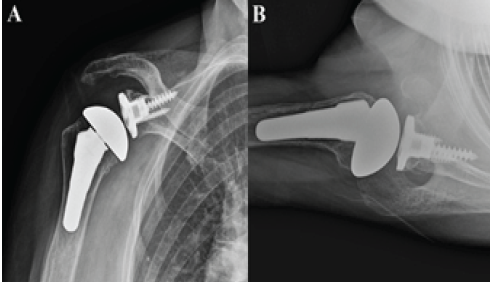
Figure 4: Post-operative plain radiographs of the right shoulder at 4 years. (a) Anteroposterior view. (b) Axillary view.
This case highlights the successful application of a primary LDTM tendon transfer performed concurrently with anatomic TSA in a patient presenting with severely compromised subscapularis tendons. The subscapularis plays a crucial role in anterior glenohumeral stability and IR strength, contributing significantly to the overall biomechanics of the shoulder [13]. Its insufficiency in the setting of TSA poses a formidable challenge, as failure to restore subscapularis function can lead to anterior instability, compromised implant longevity, and suboptimal clinical outcomes [7,14]. Traditionally, when subscapularis repair is not feasible, RTSA is considered; however, RTSA fundamentally alters native shoulder biomechanics by medialising and lowering the centre of rotation and shifting reliance predominantly to the deltoid muscle [7,15,16]. While effective for pain relief and stability, RTSA can result in reduced rotational strength and functional limitations, particularly in younger or more active patients who require greater functional demand [17,18,19,20]. The biomechanical rationale for incorporating LDTM tendon transfer lies in its ability to compensate for subscapularis deficiency by providing a dynamic muscular force that supports anterior stabilisation and IR [8,9,10,11,21]. Conventionally, PM transfer has been widely used, with numerous studies demonstrating its effectiveness in improving pain and function in patients with irreparable subscapularis tears in the native shoulder [22,23,24]. However, Elhassan et al. [8] noted that the PM muscle fibres run nearly perpendicular to the subscapularis, contradicting the principle that the transferred tendon should replicate the original muscle’s vector. Similarly, Elhassan et al. [25] reported that redirecting the PM tendon’s vector does not significantly alter its action, as the muscle belly remains anchored to the anterior chest wall. As an alternative, LD has been proposed as a more suitable donor due to its posterior origin and muscle fibre direction, which more closely approximates the subscapularis line of pull. Kontaxis et al.’s [26] biomechanical analysis demonstrated that LD transfer preserves an IR moment arm similar to the native subscapularis throughout the range of IR. While LD transfer alone may be insufficient to fully restore anterior stability, the combined transfer of LD and TM enhances the posterior line of pull and re-establishes more balanced glenohumeral force coupling [21]. In addition, Boileau et al. [20] reported that the LD tendon is often thin and prone to tearing and showed that incorporating the TM improves tendon bulk, stability, and handling, allowing for stronger fixation. In this context, LDTM transfer offers a compelling biological alternative to restore dynamic anterior stabilisation and IR without sacrificing anatomic joint mechanics, as is the case with RTSA [27,28,29]. RTSA, though reliable in the setting of rotator cuff deficiency, shifts the centre of rotation medially and inferiorly, which alters normal shoulder kinematics and diminishes rotational torque – potentially limiting functional outcomes, particularly in active individuals [7]. In contrast, TSA with LDTM transfer preserves native biomechanics and allows for more physiological shoulder motion, particularly in patients with intact posterosuperior rotator cuff components. While LDTM transfer has been widely applied in RTSA to address both internal and ER deficits, its use in conjunction with primary TSA remains relatively underexplored [19,20,27,28,29]. This case report contributes to a growing body of literature suggesting that, in select patients with primary osteoarthritis and irreparable subscapularis tears, LDTM transfer at the time of TSA may provide a more dynamic and potentially durable solution as an alternative treatment option for RTSA. Despite the promising theoretical benefits, several limitations and challenges remain associated with the current procedure. This may include restricted tendon excursion, suboptimal replication of the native subscapularis force vector, risk of muscle atrophy or lengthening over time, and the technical demands of the procedure. Appropriate patient selection is critical, particularly favouring younger, active individuals with an irreparable isolated subscapularis tear and preserved glenoid and humeral bone stock. To date, there are no published clinical outcomes evaluating the efficacy of primary TSA combined with LDTM transfer. Therefore, the integration of this technique in clinical practice should be approached with cautious optimism. Future investigations should aim to include larger, prospective cohorts, longer follow-up periods, and biomechanical validation to determine the durability and functional advantages of this combined approach.
This case demonstrates that primary LDTM tendon transfer combined with anatomic TSA can effectively improve function in patients with osteoarthritis with an isolated subscapularis tear. The combined procedure preserves native shoulder biomechanics and provides durable clinical and radiographic outcomes. Further studies are warranted to validate these findings and establish broader indications for this surgical approach.
This case demonstrates that primary LDTM tendon transfer combined with anatomic TSA can effectively improve function in patients with osteoarthritis with an isolated subscapularis tear. The combined procedure preserves native shoulder biomechanics and provides durable clinical and radiographic outcomes. Further studies are warranted to validate these findings and establish broader indications for this surgical approach.
References
- 1. McDonald J, Lachance AD, MacDonald J, Sogard O, Mooney N, Choi JY. Five-year clinical outcomes of metal-backed, hybrid, and polyethylene glenoid components in total shoulder arthroplasty. Clin Shoulder Elb 2025;28:196-203. [Google Scholar] [PubMed]
- 2. Piper CC, Horneff JG 3rd. Management of subscapularis insufficiency after total shoulder arthroplasty. J Am Acad Orthop Surg 2022;30:933-40. [Google Scholar] [PubMed]
- 3. Shields E, Ho A, Wiater JM. Management of the subscapularis tendon during total shoulder arthroplasty. J Shoulder Elbow Surg 2017;26:723-31. [Google Scholar] [PubMed]
- 4. Ahmed AF, T Kreulen R, Mikula J, Nayar SK, Miller AS, McFarland EG, et al. Subscapularis management in anatomic total shoulder arthroplasty: A systematic review and network meta-analysis. Shoulder Elbow 2023;15:15-24. [Google Scholar] [PubMed]
- 5. Kim SC, Kim IS, Jang MC, Yoo JC. Complications of reverse shoulder arthroplasty: A concise review. Clin Shoulder Elb 2021;24:42-52. [Google Scholar] [PubMed]
- 6. Oh JH, Jeong HJ, Won YS. Implant selection for successful reverse total shoulder arthroplasty. Clin Shoulder Elb 2023;26:93-106. [Google Scholar] [PubMed]
- 7. Goetti P, Denard PJ, Collin P, Ibrahim M, Mazzolari A, Lädermann A. Biomechanics of anatomic and reverse shoulder arthroplasty. EFORT Open Rev 2021;6:918-31. [Google Scholar] [PubMed]
- 8. Elhassan BT, Wagner ER, Kany J. Latissimus dorsi transfer for irreparable subscapularis tear. J Shoulder Elbow Surg 2020;29:2128-34. [Google Scholar] [PubMed]
- 9. Mun SW, Kim JY, Yi SH, Baek CH. Latissimus dorsi transfer for irreparable subscapularis tendon tears. J Shoulder Elbow Surg 2018;27:1057-64. [Google Scholar] [PubMed]
- 10. Baek CH, Kim JG, Baek GR. Outcomes of combined anterior latissimus dorsi and teres major tendon transfer for irreparable anterosuperior rotator cuff tears. J Shoulder Elbow Surg 2022;31:2298-307. [Google Scholar] [PubMed]
- 11. Baek CH, Kim JG, Kim BT, Kim SJ. Isolated latissimus dorsi transfer versus combined latissimus dorsi and teres major tendon transfer for irreparable anterosuperior rotator cuff tears. Clin Orthop Surg 2024;16:761-73. [Google Scholar] [PubMed]
- 12. Goutallier D, Postel JM, Bernageau J, Lavau L, Voisin MC. Fatty muscle degeneration in cuff ruptures. Pre- and postoperative evaluation by CT scan. Clin Orthop Relat Res 1994;304:78-83. [Google Scholar] [PubMed]
- 13. Huegel J, Williams AA, Soslowsky LJ. Rotator cuff biology and biomechanics: A review of normal and pathological conditions. Curr Rheumatol Rep 2015;17:476. [Google Scholar] [PubMed]
- 14. Friedman RJ. Biomechanics of total shoulder arthroplasty: A preoperative and postoperative analysis. Semin Arthroplasty 1995;6:222-32. [Google Scholar] [PubMed]
- 15. Rugg CM, Coughlan MJ, Lansdown DA. Reverse total shoulder arthroplasty: Biomechanics and indications. Curr Rev Musculoskelet Med 2019;12:542-53. [Google Scholar] [PubMed]
- 16. Roche CP. Reverse shoulder arthroplasty biomechanics. J Funct Morphol Kinesiol 2022;7:13. [Google Scholar] [PubMed]
- 17. Kim SC, Lee JE, Lee SM, Yoo JC. Factors affecting internal rotation after reverse shoulder arthroplasty. J Orthop Sci 2022;27:131-8. [Google Scholar] [PubMed]
- 18. Luster TG, Dean RS, Trasolini NA, Eichinger JK, Parada SA, Ralston RK, et al. Predictive factors influencing internal rotation following reverse total shoulder arthroplasty. J Shoulder Elbow Surg 2024;33:1200-8. [Google Scholar] [PubMed]
- 19. Boileau P, Chuinard C, Roussanne Y, Bicknell RT, Rochet N, Trojani C. Reverse shoulder arthroplasty combined with a modified latissimus dorsi and teres major tendon transfer for shoulder pseudoparalysis associated with dropping arm. Clin Orthop Relat Res 2008;466:584-93. [Google Scholar] [PubMed]
- 20. Boileau P, Chuinard C, Roussanne Y, Neyton L, Trojani C. Modified latissimus dorsi and teres major transfer through a single delto-pectoral approach for external rotation deficit of the shoulder: As an isolated procedure or with a reverse arthroplasty. J Shoulder Elbow Surg 2007;16:671-82. [Google Scholar] [PubMed]
- 21. Baek GR, Kim JG, Nakla AP, Kwak D, Chung MS, McGarry MH, et al. Latissimus dorsi and teres major tendon transfer for irreparable anterosuperior rotator cuff tear improves kinematics and internal rotation compared to latissimus dorsi tendon transfer. Arch Orthop Trauma Surg 2023;143:4731-9. [Google Scholar] [PubMed]
- 22. Sánchez Carbonel JF, Hinz M, Lozano C, Kleim BD, Imhoff AB, Siebenlist S. Pectoralis major and pectoralis minor transfer for irreparable subscapularis tendon tears. Oper Orthop Traumatol 2022;34:45-54. [Google Scholar] [PubMed]
- 23. Nelson GN, Namdari S, Galatz L, Keener JD. Pectoralis major tendon transfer for irreparable subscapularis tears. J Shoulder Elbow Surg 2014;23:909-18. [Google Scholar] [PubMed]
- 24. Burnier M, Lafosse T. Pectoralis major and anterior latissimus dorsi transfer for subscapularis tears. Curr Rev Musculoskelet Med 2020;13:725-33. [Google Scholar] [PubMed]
- 25. Elhassan B, Christensen TJ, Wagner ER. Feasibility of latissimus and teres major transfer to reconstruct irreparable subscapularis tendon tear: An anatomic study. J Shoulder Elbow Surg 2014;23:492-9. [Google Scholar] [PubMed]
- 26. Kontaxis A, Lawton CD, Sinatro A, Bachner E, Lamplot JD, Dines DM, et al. Biomechanical analysis of latissimus dorsi, pectoralis major, and pectoralis minor transfers in subscapularis-deficient shoulders. J Shoulder Elbow Surg 2022;31:420-7. [Google Scholar] [PubMed]
- 27. Baek CH, Kim JG, Baek GR. Restoration of active internal rotation following reverse shoulder arthroplasty: Anterior latissimus dorsi and teres major combined transfer. J Shoulder Elbow Surg 2022;31:1154-65. [Google Scholar] [PubMed]
- 28. Baek CH, Kim JG, Baek GR, Baek G, Chung MS, McGarry MH, et al. Biomechanical comparison of internal rotational effectiveness following medialized glenoid and lateralized humerus reverse shoulder arthroplasty with tendon transfers: Isolated latissimus dorsi, combined latissimus dorsi/teres major, and pectoralis major tendon transfers. J Shoulder Elbow Surg 2025;34:1773-82. [Google Scholar] [PubMed]
- 29. Baek GR, Kim JG, Baek CH, Baek G, Chung MS, Kao O, et al. Latissimus dorsi and teres major tendon transfer increases internal rotation torque following lateralized reverse shoulder arthroplasty with subscapularis insufficiency. Arch Orthop Trauma Surg 2023;143:5759-66. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Delayed Spontaneous Pectoralis Major Tendon Rupture Following Anterior Latissimus Dorsi Transfer for Irreparable Subscapularis Tear: A Case Report
June 1, 2026 Delayed Spontaneous Pectoralis Major Tendon Rupture Following Anterior Latissimus Dorsi Transfer for Irreparable Subscapularis Tear: A Case Report July 10, 2022 Shoulder Injury Following Overzealous Manipulation in Adhesive Capsulitis by Untrained Professional Managed with Shoulder Arthroscopy
July 10, 2022 Shoulder Injury Following Overzealous Manipulation in Adhesive Capsulitis by Untrained Professional Managed with Shoulder Arthroscopy March 1, 2026 Clinical outcome of Intramedullary Screw Fixation in Metacarpal and Phalangeal Fractures
March 1, 2026 Clinical outcome of Intramedullary Screw Fixation in Metacarpal and Phalangeal Fractures November 1, 2025 Use of Credit Cards by Orthopedic Surgeons: Evaluating the Pros and Cons
November 1, 2025 Use of Credit Cards by Orthopedic Surgeons: Evaluating the Pros and Cons