
En bloc excision with a non-vascularised ulnar cortical graft provides effective oncological clearance with excellent functional reconstruction in metacarpal giant cell tumours.
Dr. Subashini Rajendiran, Department of Hand Surgery, Sri Ramachandra Institute of Higher Education and Research, Porur, Chennai - 600116, Tamil Nadu, India. E-mail: doctor.subashini@ymail.com
Abstract
Introduction: A giant cell tumour (GCT) of bone is a benign but locally aggressive neoplasm, most commonly affecting the epiphyseal region of long bones. Involvement of the hand bones is rare and is known to exhibit more aggressive behaviour with higher recurrence rates compared to conventional sites. Optimal reconstruction following tumour excision in the hand remains challenging, as, along with the reconstruction of the bone defect, the function of the hand should also be addressed.
Case Report: A 19-year-old right-hand-dominant female presented with a progressively enlarging, painful swelling over the dorsum of the right hand. Radiological evaluation revealed an expansile, lytic lesion involving the ring finger metacarpal with cortical breach. Magnetic resonance imaging showed an aggressive lesion with soft-tissue involvement. Histopathological examination confirmed the diagnosis of GCT of bone. The patient underwent wide excision of the tumour followed by reconstruction using a non-vascularised autologous cortical bone graft from the ulna.
Conclusion: GCT of the metacarpal is rare and requires aggressive surgical management due to its high recurrence potential. A non-vascularised ulnar bone graft provides a reliable, simple, and effective reconstructive option following tumour excision.
Keywords: Giant cell tumors, non-vascularized bone grafts, en bloc excision, multinucleate giant cells.
Giant cell tumours (GCTs) of bone account for approximately 5% of all primary bone tumours [1] and typically affect skeletally mature individuals in the third and fourth decades of life [1]. The most common locations include the distal femur, proximal tibia, and distal radius [1,2]. Involvement of the hand bones is rare [3], accounting for less than 2% of cases, but is associated with more aggressive biological behaviour and higher recurrence rates [4,5]. Due to the small size of hand bones and proximity to tendons, neurovascular structures, and joints, management of GCT in the hand poses unique surgical challenges. Various treatment modalities have been described, ranging from curettage to wide excision with reconstruction based on the size of the tumour. This case report highlights the successful management of metacarpal GCT using en bloc excision and reconstruction with a non-vascularised ulnar bone graft.
A 19-year-old female presented with a 6-month history of pain and gradually progressive swelling over the dorsum of the right hand. The pain was dull and aching in nature, aggravated by activity, and not relieved by rest. There was no history of trauma, fever, or constitutional symptoms.
Clinical examination:
Local examination revealed a firm, tender swelling over the fourth (ring finger) metacarpal region. The overlying skin was normal with no signs of inflammation. Finger movements were painful but preserved. The sensation of the hand was normal, and the fingers were viable.
Radiological findings:
Plain radiographs of the right hand showed an expansile, lytic lesion involving the fourth metacarpal with cortical thinning and breach. No matrix calcification was noted (Fig. 1).
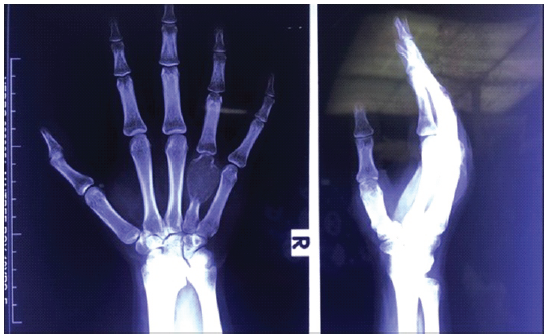
Figure 1: Anteroposterior and lateral radiograph of the right hand, an expansile lytic lesion involving the fourth metacarpal with cortical thinning and breach.
Magnetic resonance imaging revealed a well-defined expansile lesion with hypointense to isointense signal on T1-weighted images and hyperintense signal on T2-weighted images, with cortical destruction and soft tissue extension over the right fourth metacarpal. A core needle biopsy was performed at an outside hospital prior to definitive surgery, suggesting features consistent with a GCT of bone, guiding the decision for wide excision (Fig. 2).
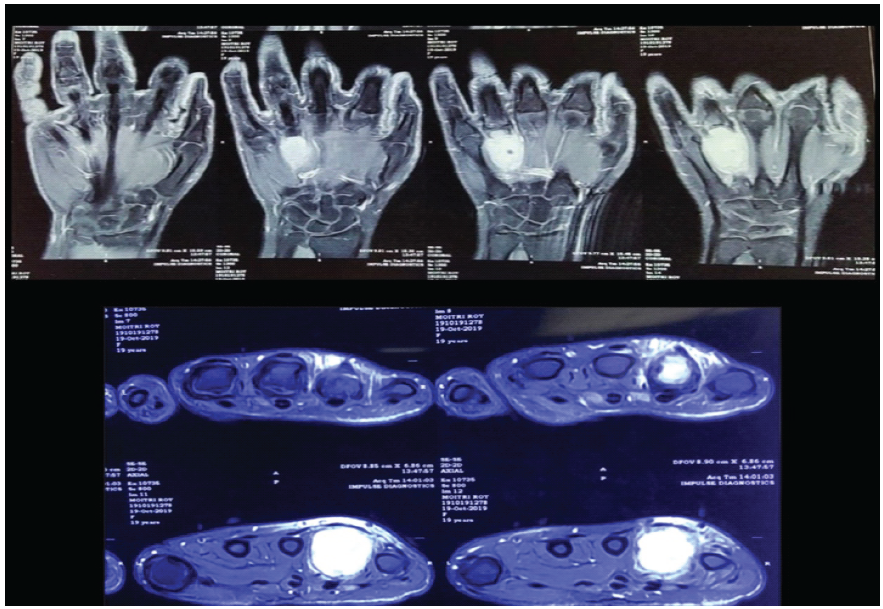
Figure 2: Magnetic resonance imaging of coronal and axial cuts of the right hand revealed a well-defined expansile lesion with hypointense to isointense signal on T1-weighted images and hyperintense signal on T2-weighted images, with cortical destruction and soft tissue extension over the right hand fourth metacarpal.
Surgical management:
The patient underwent right-hand ring-finger en bloc excision of the tumour through a dorsal approach. Following complete tumour removal, a bone defect of approximately 3 cm was present. Reconstruction was performed using a non-vascularised autologous cortical bone graft harvested from the ipsilateral ulna. A graft of size 4 cm × 1.5 cm was harvested along the subcutaneous border (posterior border) of the ulna about 4 cm proximal to the olecranon process. Part of the medial surface and part of the posterior surface, with the posterior border in the middle, was harvested. The graft was shaped appropriately and pegged inside the proximal part of the remnant 4th metacarpal and fixed by two K-wires. The wound was closed in layers. For the immediate post-operative period, a dorsal slab was applied with the wrist in neutral, the metacarpophalangeal joints in 70° flexion, and finger IP joints in extension (Figs. 3, 4, 5, 6, 7).

Figure 3: Intra-operative photographs demonstrating exposure and excision over the dorsal aspect of the hand. The lesion was excised meticulously. A defect of approximately 3 cm was noted after excision. The defect was filled using a graft from the posterior border of the ulna.
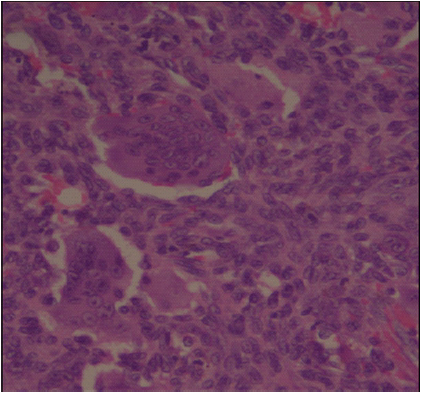
Figure 4: Histopathological slide showing numerous osteoclast-like multinucleated giant cells uniformly distributed among mononuclear stromal cells.

Figure 5: Two months post-operative follow-up anteroposterior and oblique radiograph of the right hand showing incorporating graft over the fourth metacarpal region.

Figure 6: Two-month post-operative follow up clinical image showing healed surgical scar site over the dorsum of the right hand, dorsum of elbow (donor site), flexion of finger at metacarpophalangeal joint, and making of fist demonstrating the functional outcome.
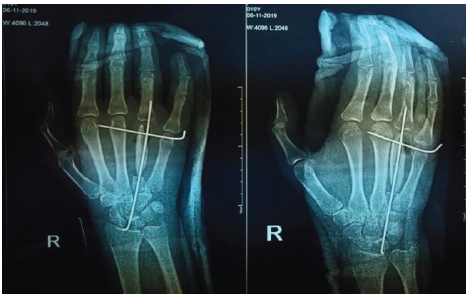
Figure 7: Immediate post-operative follow-up anteroposterior and oblique radiograph of the right hand showing incorporating graft over the fourth metacarpal region with K-wire pinning.
Histopathology:
Histopathological examination showed numerous osteoclast-like multinucleated giant cells uniformly distributed among mononuclear stromal cells, consistent with GCT of bone. The resected margins were free of tumour (negative margins), confirming adequate oncological clearance (Fig. 4).
Post-operative outcome:
The post-operative period was uneventful. The patient was started on early mobilisation within a splint from the 3rd postoperative day. Radiographs at follow-up demonstrated satisfactory graft incorporation and alignment. She was followed up for a period of 5 years, and the patient had good functional recovery of the hand with no evidence of local recurrence. The patient was able to write with this hand (Figs. 5 and 6).
GCT of bone affecting the metacarpals is uncommon and is recognised for its relatively aggressive clinical behaviour compared to lesions in long bones [4,5]. The small size of the hand bones, thin cortices, and limited soft-tissue envelope contribute to early cortical breach [4] and extraosseous extension, often resulting in more advanced disease at presentation [5]. These anatomical characteristics also explain the higher recurrence rates [6] reported when intralesional curettage is used as the primary treatment for hand GCTs. The principal goal of management in such cases is to achieve adequate oncologic clearance while preserving as much hand function as possible. Although curettage remains acceptable in conventional GCT, its use in hand lesions has historically been associated with frequent recurrence. Consequently, wide or marginal excision followed by structural reconstruction is favoured in most reported series [7,8], as it offers better local control. Reconstruction of post-excisional defects in the metacarpal poses a unique challenge [9] because the reconstructed segment must restore bone continuity, maintain length, and allow tendon gliding and joint motion. Several methods have been described, including non-vascularised autografts, vascularised bone transfers, arthrodesis, and prosthetic reconstruction. The choice of technique is influenced by patient age, tumour extent, bone stock, surgeon expertise, and functional expectations. In the present case, a non-vascularised cortical bone graft from the ulna was used. This option offers a biologically compatible, mechanically stable graft with minimal donor-site morbidity and does not require microsurgical reconstruction. When performed in a well-vascularised bed, non-vascularised grafts have shown predictable incorporation, especially in young patients [10]. Vascularised bone grafts may be beneficial in situations involving large defects, compromised soft tissues, or previously operated beds [11]. However, they are technically demanding, prolonging operative time [12,13], and may not confer additional benefit in routine metacarpal reconstruction. In our patient, graft integration and satisfactory hand function were achieved without recurrence at follow-up. Adjunctive options such as chemical cauterisation, cryotherapy, cement augmentation, or systemic agents have been explored in conventional GCT [4], but their applicability in the hand remains limited due to concerns [6] regarding soft-tissue injury, thermal necrosis, or delayed graft healing in small bones. For this reason, surgical excision with biological reconstruction continues to be regarded as the most reliable treatment strategy in this anatomical region [5]. Metacarpal bone defects are most commonly reconstructed [14,15] with the distal radius and iliac crest being the preferred donor sites due to their ease of harvest, adequate graft volume, and predictable incorporation. Olecranon [16] and non-vascularised fibular strut grafts have also been described for moderate to segmental defects requiring additional structural support. Use of the ulna as a donor site is rarely reported in the literature and is largely limited to isolated case reports [15]. Nevertheless, in a well-vascularised bed, a non-vascularised ulnar cortical graft can provide adequate mechanical stability with minimal donor-site morbidity, making it a viable alternative in selected patients. Overall, the present case reinforces the view that en bloc excision followed by biological reconstruction is a rational and effective treatment approach for metacarpal GCTs. Reconstruction using a non-vascularised ulnar bone graft provides a simple, reproducible, and functionally satisfactory solution, particularly in young patients where preservation of hand function is paramount. Continued reporting of similar clinical experiences will help refine treatment algorithms for this rare entity.
GCT of the metacarpal is a rare entity requiring aggressive surgical management. En bloc excision followed by reconstruction using a non-vascularised ulnar bone graft for smaller defects is a safe, effective, and reproducible technique with satisfactory functional outcomes.
Metacarpal giant cell tumours are rare and aggressive, with high recurrence after intralesional treatment. En bloc excision with non-vascularised ulnar graft reconstruction provides a reliable and function-preserving solution.
References
- 1. Sobti A, Agrawal P, Agarwala S, Agarwal M. Giant cell tumor of bone – an overview. Arch Bone Jt Surg 2016;4:2-9. [Google Scholar] [PubMed]
- 2. Karpik M, Mazurkiewicz T, Wysocki M, Kwiatkowski K, Biały R, Koczy B, et al. Giant cell tumor of bone: population-based clinical series. Ortopedia Traumatologia Rehabilitacja. 2010;12(3):207–215. [Google Scholar] [PubMed]
- 3. James SL, Davies AM, Grimer RJ, Mangham DC, Rackham S, de Silva MVC, et al. Giant-cell tumours of bone of the hand and wrist. J Hand Surg Br. 2005;30(5):492–498. [Google Scholar] [PubMed]
- 4. Biscaglia R, Bacchini P, Bertoni F. Giant cell tumor of the bones of the hand and foot. Cancer 2000;88:2022-32. [Google Scholar] [PubMed]
- 5. Athanasian EA. Giant cell tumor of bone of the hand. J Hand Surg Am 2004;29:658-64. [Google Scholar] [PubMed]
- 6. O’Donnell RJ, Springfield DS, Motwani HK, Ready JE, Gebhardt MC, Mankin HJ. Recurrence of giant-cell tumors of the long bones after curettage and packing with cement. J Bone Joint Surg Am 1994;76:1827-33. [Google Scholar] [PubMed]
- 7. Campanacci M, Baldini N, Boriani S, Sudanese A. Giant-cell tumor of bone. J Bone Joint Surg Am 1987;69:106-14. [Google Scholar] [PubMed]
- 8. Raskin KA, Schwab JH, Mankin HJ, Springfield DS, Hornicek FJ. Giant cell tumor of bone. Cancer Treat Res 2015;162:291-303. [Google Scholar] [PubMed]
- 9. Dubois J, Touam C, Kakar S, Wolfe SW, Athanasian EA, Della Valle AG, et al. Reconstruction after resection of tumors of the hand. Hand Clinics. 2004;20(3):243–256. [Google Scholar] [PubMed]
- 10. Enneking WF, Mindell ER. Observations on massive retrieved human allografts. J Bone Joint Surg Am 1991;73:1123-42. [Google Scholar] [PubMed]
- 11. Urbaniak JR, Harvey EJ. Reconstruction with vascularized bone grafts. J Bone Joint Surg Am 1998;80:1080-96. [Google Scholar] [PubMed]
- 12. Weiland AJ, Moore JR, Daniel RK. Vascularized bone autografts. J Bone Joint Surg Am 1983;65:199-207. [Google Scholar] [PubMed]
- 13. Aponte-Tinao LA. Reconstruction after resection of bone tumors of the hand. Clin Orthop Relat Res 2012;470:757-64. [Google Scholar] [PubMed]
- 14. Sood A, Therattil PJ, Lee ES, Granick MS, Cho MJ, Moran SL, et al. Reconstruction of a complex metacarpal shaft fracture with autologous bone graft: Indications and graft options. J Hand Surg Am. 2015;40:1004–1008.. [Google Scholar] [PubMed]
- 15. Walker LG, Greene TL, Lunseth PA, White WL, Hanel DP, Hastings H, et al. Proximal ulna cortical bone graft for reconstruction of a metacarpal defect: Early recommendation. J Hand Surg Am. 1990;15:489–492. [Google Scholar] [PubMed]
- 16. Babushkina A, Edwards S. Corticocancellous olecranon autograft for metacarpal defect reconstruction: A case report. Hand (N Y) 2012;7:457-60. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 February 1, 2026 Isolated Osteochondromas of the Inner and Outer Tables of the Ilium: A Report of two Rare Cases
February 1, 2026 Isolated Osteochondromas of the Inner and Outer Tables of the Ilium: A Report of two Rare Cases November 1, 2025 Cavernous Hemangioma of Hoffa’s Fat Pad: A Rare Case Presentation
November 1, 2025 Cavernous Hemangioma of Hoffa’s Fat Pad: A Rare Case Presentation May 1, 2025 The Giant Cell Tumor of 1st Metatarsal in a Young Adult: A Rare Versatile Management with Fibula Cortical Graft
May 1, 2025 The Giant Cell Tumor of 1st Metatarsal in a Young Adult: A Rare Versatile Management with Fibula Cortical Graft November 1, 2024 Aggressive Giant Cell Tumor of Proximal Tibia Treated with Resection and Arthrodesis using Limb Reconstruction System – A Case Report
November 1, 2024 Aggressive Giant Cell Tumor of Proximal Tibia Treated with Resection and Arthrodesis using Limb Reconstruction System – A Case Report