
In skeletally immature patients with chronic ankle instability, arthroscopic all-inside repair of lateral ankle ligament detachments can be safely performed when anchor length and insertion angle are carefully selected to respect the distal fibular physis and avoid peroneal tendon irritation.
Dr. Fernando Alfredo Fernández-Garza, Department of Traumatology and Orthopedics, Instituto de Seguridad Social de Trabajadores del Estado de Nuevo León, Monterrey, Nuevo León, México.
Abstract
Introduction: A lateral ankle sprain is among the most common orthopaedic injuries and may progress to chronic ankle instability (CAI), particularly in adolescents engaged in sports. Approximately 20–40% of patients with acute ankle sprains develop CAI, which is associated with recurrent instability, pain, and impaired athletic performance. Evidence regarding the surgical management of CAI in the paediatric population remains limited. This study aimed to evaluate the functional outcomes of arthroscopic all‑inside ligament repair in adolescents with CAI refractory to conservative treatment.
Materials and Methods: A retrospective observational case series was conducted between January 2024 and May 2025. Patients younger than 16 years with CAI unresponsive to at least 6 months of conservative management and with a minimum postoperative follow-up of 12 months were included. Demographic variables and time to return to sports were recorded. Functional outcomes were assessed using the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle–Hindfoot Score and the Karlsson–Peterson Ankle Score, measured preoperatively and at 3, 6, and 12 months postoperatively. Statistical analysis was performed using the Friedman test with Wilcoxon signed‑rank post hoc comparisons and Kendall’s W for effect size.
Results: Five patients (2 males, 3 females; mean age 14.4 ± 0.8 years) were included. All returned to sports at a mean of 2.8 months postoperatively. No complications were reported. The mean baseline AOFAS score was 71.0 ± 8.2, improving to 98.0 ± 4.4 at 3 months and reaching 100.0 at 6 and 12 months. The Karlsson–Peterson score increased from 61.2 ± 10.7 at baseline to 93.0 ± 5.7 at 3 months and 100.0 at subsequent follow‑ups. The Friedman test demonstrated significant differences across time points (AOFAS: χ2 = 13.62, P = 0.0035; Karlsson–Peterson: χ2 = 15.00, P = 0.0018), with Kendall’s W = 1.0 indicating a very large effect size.
Conclusion: Arthroscopic all‑inside ligament repair in adolescents with CAI refractory to conservative management yielded excellent functional outcomes, early return to sports, and no complications. Anchor size selection was critical to avoid physeal injury and peroneal tendon irritation. These findings support the feasibility and safety of minimally invasive ligament repair in skeletally immature patients, although larger studies with longer follow-up are warranted to confirm durability and generalisability.
Keywords: Chronic ankle instability, arthroscopic ligament repair, pediatric orthopedics, minimally invasive surgery.
A lateral ankle sprain is one of the most common orthopaedic injuries and may lead to long-term complications, including chronic ankle instability (CAI). It is estimated that approximately 20–40% of patients who sustain an acute ankle sprain subsequently develop CAI [1]. In a systematic review conducted by Fong et al., the ankle was identified as the most frequently injured anatomical region in 24 of the 70 sports analysed. Moreover, ankle sprain was the most common ankle injury in 33 of 43 sports, with a higher incidence observed in court-based and team sports [2]. CAI typically develops following a lateral ankle sprain and is characterised by recurrent episodes of instability, sensations of “giving way”, weakness during physical activity, and self-reported disability persisting for more than 6 months [3]. The literature addressing CAI in the paediatric population remains limited; however, previous reports suggest that up to 30% of paediatric patients who experience an ankle sprain may develop this condition [4]. Initial management consists primarily of functional rehabilitation [5,6]. Nevertheless, in patients who fail conservative treatment, surgical intervention may be indicated [1]. Despite the growing use of arthroscopic ligament repair techniques in adults, evidence regarding their safety and functional outcomes in skeletally immature patients remains scarce. Concerns regarding potential physeal injury continue to limit the widespread adoption of surgical treatment in paediatric patients with CAI. Furthermore, there is limited literature specifically evaluating all-inside arthroscopic repair techniques in adolescent populations. Therefore, additional clinical evidence is needed to better characterise postoperative outcomes and the feasibility of these minimally invasive procedures in this age group. The aim of the present study is to describe the functional outcomes of paediatric patients diagnosed with CAI who were refractory to conservative management and subsequently treated with surgical intervention.
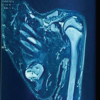
A retrospective, observational case series was conducted between January 2024 and May 2025. Patients younger than 16 years of age with a diagnosis of CAI who were refractory to conservative treatment for a minimum of 6 months, had a minimum postoperative follow-up of 12 months, and had confirmation of diagnosis through diagnostic imaging were included (Fig. 1).
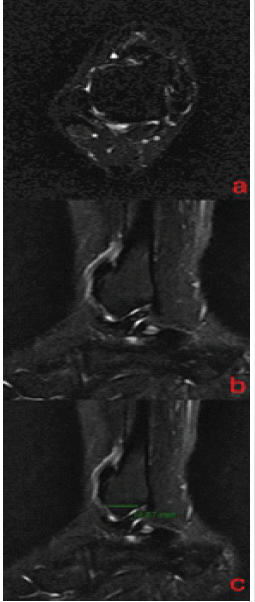
Figure 1: Distal fibular deinsertion from anterior talofibular ligament*.
Demographic variables were collected, including sex, age, affected side, and type of sport practised. Time to return to sports activity was also recorded. Ankle function was assessed using the American Orthopaedic Foot and Ankle Society (AOFAS) Ankle–Hindfoot Score [7] and the Karlsson–Peterson Ankle Score [8]. Evaluations were performed preoperatively and at 3, 6, and 12 months following surgical intervention. All patients underwent arthroscopic repair of the anterior talofibular ligament (ATFL) using the all-inside ankle technique [9,10] (Fig. 2).
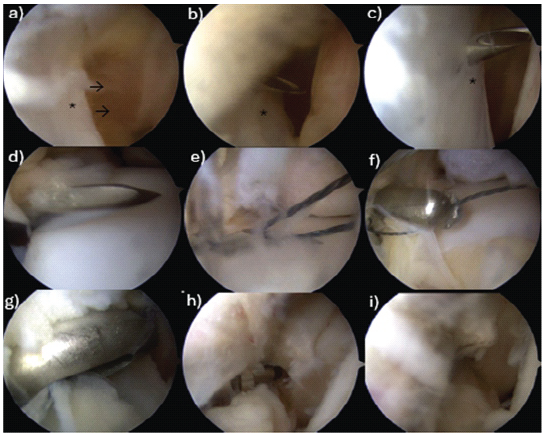
Figure 2: Arthroscopic repair and all-inside reinsertion with a needle and nitinol of the anterior talofibular ligament (a-c*) detached from the distal fibula→. This ligament was retrieved with a loop suture (c-f). A loop suture tape was used for retrieve (g) and subsequent reinsertion with a 2.9 mm. Pushlock anchor (Arthrex Naples Fl, US) (h). The repaired anterior talofibular ligament is identified (i).
Means and standard deviations were calculated for each time point. For inferential analysis, the Friedman test for related samples was applied, given the small sample size and non-normal distribution. Pairwise comparisons were performed using the Wilcoxon signed-rank test with Bonferroni correction. Effect size was reported using Kendall’s W. Statistical analyses were performed using IBM Statistical Package for the Social Sciences Statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA). A significance level of P < 0.05 was considered.
Five patients were included (2 males and 3 females), with a mean age of 14.4 ± 0.8 years. All patients returned to sports activity at an average of 3 months postoperatively. No recurrent instability, neurovascular injury, wound complications, or growth-related complications were observed. Individual demographic characteristics are presented in Table 1.
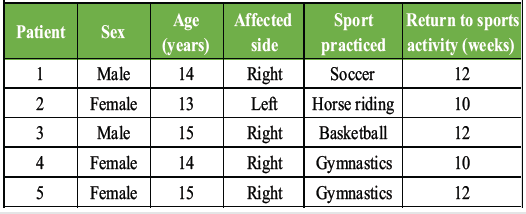
Table 1: Individual demographic data
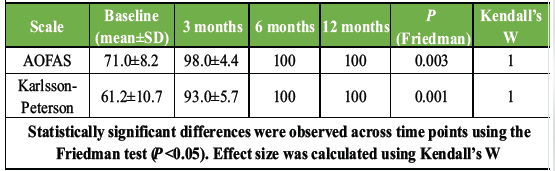
Table 2: Functional outcomes after arthroscopic ligament repair
Functional outcomes are summarised in Table 2. The mean baseline AOFAS Ankle–Hindfoot Score was 71.0 ± 8.2 points, increasing to 98.0 ± 4.4 at 3 months and reaching 100.0 at both 6 and 12 months. The Karlsson–Peterson Ankle Score showed baseline values of 61.2 ± 10.7, rising to 93.0 ± 5.7 at 3 months and 100.0 at subsequent follow-ups. The Friedman test demonstrated statistically significant differences across time points for both scales (AOFAS: χ2 = 13.62, P = 0.0035, Kendall’s W = 1.0; Karlsson–Peterson: χ2 = 15.00, P = 0.0018, Kendall’s W = 1.0). Post hoc Wilcoxon signed-rank comparisons between baseline and each follow-up showed a consistent trend toward improvement, although P-values did not reach statistical significance (P = 0.06), likely attributable to the small sample size. Clinically, all patients achieved maximum scores in both scales by 6 months, which remained stable through the 12-month follow-up.
With the progressive increase in sports participation, training intensity, and competitive level among adolescents, a parallel rise in sports-related musculoskeletal injuries is expected, including lateral ankle sprains [4,11,12]. Although initial conservative management remains the first-line treatment for lateral ankle ligament injuries in this population according to current clinical practice guidelines [6], a subset of patients fails non-operative treatment and progresses to CAI or microinstability, a condition whose diagnosis and optimal surgical management remain controversial according to biomechanical evidence [13]. This clinical scenario is associated with recurrent sprains, persistent pain, and a subjective sensation of instability, ultimately impairing sports participation and quality of life [11,14]. In this context, the availability of effective and safe surgical alternatives becomes essential. The available evidence on all-inside arthroscopic treatment in the paediatric population with CAI remains limited. However, the results observed in this case series demonstrate significant clinical and functional improvement as early as 3 months after surgical intervention, with peak scores reached at 6 months and maintained through 12-month follow-up. An important aspect is the time to return to sports activity, which in our cohort averaged 2.8 months. This finding suggests an accelerated recovery, possibly attributable to the minimally invasive approach. Although there is no specific literature directly comparing arthroscopic versus open techniques in paediatric patients, our findings are consistent with the return-to-sport times reported by Xiong et al. [12]. The findings of Xiong et al. [15] suggest that structural imaging parameters do not necessarily influence functional outcomes following surgical stabilisation in adolescents with CAI. This is consistent with our results, which demonstrate significant improvements in patient-reported ankle function regardless of magnetic resonance imaging signal characteristics. These observations reinforce the importance of comprehensive clinical and functional assessment in surgical decision-making [6] for paediatric patients and support the individualisation of surgical technique based on surgeon experience and patient-specific anatomical characteristics. Although both anatomic and non-anatomic open techniques for lateral ligament repair have been described, they are associated with inherent drawbacks, including lateral soft-tissue fibrosis, wound-healing complications [14,16,17], and limited ability to assess and address concomitant intra-articular pathology. In contrast, arthroscopic approaches allow for direct visualisation and simultaneous management of associated intra-articular lesions, representing a potential advantage over open procedures. In the adult population, all-inside arthroscopic ligament repair has been shown to be a safe and cost-effective alternative for the treatment of ATFL injuries [14,16,17,18], supporting the cautious extension of this technique to younger patients. Surgical intervention in skeletally immature patients remains a topic of debate, primarily due to concerns regarding potential physeal injury. However, emerging evidence suggests that ligament repair techniques can be safely performed without compromising physeal integrity. Takao et al. [19] reported that arthroscopic repair in skeletally immature patients resulted in satisfactory clinical outcomes without growth-related complications, supporting the safety of surgical management in this population. Similarly, Guelfi et al. [20] demonstrated excellent functional outcomes without physeal violation following arthroscopic all-inside ligament repair for ankle instability in skeletally immature patients, further supporting the safety and efficacy of physeal-sparing techniques. Huang et al. [18] evaluated an all-arthroscopic approach for chronic lateral ankle instability in adolescents and observed favourable clinical outcomes and significant functional improvements in the majority of cases. These findings align with our results, which demonstrate comparable post-operative functional scores and return-to-sport timelines. Moreover, these studies emphasise the feasibility of minimally invasive surgical techniques in adolescents, with important implications for surgical planning based on patient age and skeletal maturity. In this setting, adolescent-specific anatomical considerations, including the orientation of the distal fibular physis and the morphology of the distal fibular epiphysis [11], are critical when selecting the appropriate surgical technique. Anchor size represents a key technical factor to avoid breaching the posterior fibular cortex and to minimise the risk of peroneal tendon irritation. In the present case series, favourable outcomes were achieved using 2.9 × 12.5 mm impact anchors while avoiding anchors longer than 19 mm. Our findings further demonstrate that the all-inside technique for ATFL avulsion from the fibular insertion in an adolescent population allows for safe ligament reinsertion into the distal fibular epiphysis, effectively sparing the physis and reducing the risk of peroneal tendon irritation.
Limitations:
The small sample size and case-series design limit the generalisability of the findings and preclude direct comparison with alternative surgical techniques. The absence of a control group and the single-centre nature of the study may introduce selection and performance bias, particularly given that all procedures were performed by experienced surgeons. Surgical treatment was limited to patients who failed at least 6 months of conservative management, potentially selecting a highly compliant and motivated cohort, which may have influenced the observed early return to sport. Finally, the 12-month follow-up may be insufficient to fully assess long-term outcomes, including recurrent instability or durability of the repair.
Arthroscopic all-inside repair of the ATFL in adolescents with CAI refractory to conservative treatment demonstrated excellent short-term functional outcomes, early return to sports, and no procedure-related complications in this case series. Careful surgical planning, particularly regarding anchor size selection and attention to physeal anatomy, is essential to minimise the risk of physeal injury and peroneal tendon irritation in skeletally immature patients. Larger prospective studies with longer follow-up are required to confirm the durability of these results.
Arthroscopic all-inside ligament repair represents a feasible and safe surgical option for adolescents with chronic ankle instability who fail conservative treatment. When performed with careful attention to paediatric-specific anatomy – particularly the distal fibular physis and appropriate anchor size selection – this minimally invasive technique can provide rapid functional recovery and facilitate early return to sports while minimising the risk of physeal injury and peroneal tendon irritation. This case series highlights the importance of meticulous surgical technique and individualised planning when extending advanced arthroscopic procedures to skeletally immature patients.
References
- 1. Al-Mohrej OA, Al-Kenani NS. Chronic ankle instability: Current perspectives. Avicenna J Med 2016;6:103-8. [Google Scholar] [PubMed]
- 2. Fong DT, Hong Y, Chan LK, Yung PS, Chan KM. A systematic review on ankle injury and ankle sprain in sports. Sport Med 2007;37:73-94. [Google Scholar] [PubMed]
- 3. Delahunt E, Coughlan GF, Caulfield B, Nightingale EJ, Lin CW, Hiller CE. Inclusion criteria when investigating insufficiencies in chronic ankle instability. Med Sci Sports Exerc 2010;42:2106-21. [Google Scholar] [PubMed]
- 4. Mandarakas M, Pourkazemi F, Sman A, Burns J, Hiller CE. Systematic review of chronic ankle instability in children. J Foot Ankle Res 2014;7:1-10. [Google Scholar] [PubMed]
- 5. Tedeschi R, Ricci V, Tarantino D, Tarallo L, Catani F, Donati D. Rebuilding stability: Exploring the best rehabilitation methods for chronic ankle instability. Sports 2024;12:282. [Google Scholar] [PubMed]
- 6. Vilchez-Cavazos F, Quiroga-Garza A, Acosta-Olivo CA, Rodríguez-Corpus LA, Espinosa-Uribe AG, Peña-Martínez VM, et al. Functional treatment versus immobilization for the management of acute ankle sprains: A systematic review and meta-analysis. J Bodyw Mov Ther 2025;44:48-55. [Google Scholar] [PubMed]
- 7. Kitaoka H, Alexander I, Adelaar R, Nunley J, Myerson M, Sanders M. Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes. Foot Ankle Int 1994;15:349-53. [Google Scholar] [PubMed]
- 8. Karlsson J, Peterson L. Evaluation of ankle joint function: the use of a scoring scale. Foot 1991;1:15-9. [Google Scholar] [PubMed]
- 9. Ueda N, Murahashi Y, Takahashi K, Mori Y, Watanabe K, Emori M, et al. All-inside arthroscopic anatomic anterior talofibular ligament repair for chronic lateral ankle instability and injury at the talar attachment: Surgical technique. Arthrosc Tech 2024;13:103098. [Google Scholar] [PubMed]
- 10. Nunes GA, Ferreira GF, Caetano RM, Mann TS, Guelfi M. All-inside arthroscopic repair of the anterior talofibular ligament: A case series. Int Orthop 2022;46:273-9. [Google Scholar] [PubMed]
- 11. Gruskay JA, Brusalis CM, Heath MR, Fabricant PD. Pediatric and adolescent ankle instability: Diagnosis and treatment options. Curr Opin Pediatr 2019;31:69-78. [Google Scholar] [PubMed]
- 12. Xiong S, Pan J, Xu X, Pi Y, Chen L, Jiang D, et al. Clinical Outcomes and Sports Participation After the Modified Broström Procedure in Children and Adolescents With Chronic Lateral Ankle Instability: A 5- to 10-Year Follow-up of 111 Cases. Am J Sports Med. 2025;53(10):2454–61. doi:10.1177/03635465251354961. [Google Scholar] [PubMed] [CrossRef]
- 13. Chang SH, Morris BL, Saengsin J, Tourné Y, Guillo S, Guss D, et al. Diagnosis and treatment of chronic lateral ankle instability: review of our biomechanical evidence. J Am Acad Orthop Surg 2021;29:3-16. [Google Scholar] [PubMed]
- 14. Vega J, Malagelada F, Manzanares Céspedes MC, Dalmau-Pastor M. The lateral fibulotalocalcaneal ligament complex: An ankle stabilizing isometric structure. Knee Surg Sports Traumatol Arthrosc 2020;28:8-17. [Google Scholar] [PubMed]
- 15. Xiong S, Zhong R, Pi Y, Zhao F, Chen L, Jiang D, et al. Preoperative MRI signal intensity of the anterior talofibular ligament is not associated with mid- to long-term outcomes after modified broström procedure in adolescents with chronic lateral ankle instability: A propensity-matched cohort analysis. Foot Ankle Int 2026;47:347-58. [Google Scholar] [PubMed]
- 16. Guelfi M, Vega J, Malagelada F, Dalmau-Pastor M. The arthroscopic all-inside ankle lateral collateral ligament repair is a safe and reproducible technique. Knee Surg Sport Traumatol Arthrosc 2020;28:63-9. [Google Scholar] [PubMed]
- 17. Vega J, Montesinos E, Malagelada F, Baduell A, Guelfi M, Dalmau-Pastor M. Arthroscopic all-inside anterior talo-fibular ligament repair with suture augmentation gives excellent results in case of poor ligament tissue remnant quality. Knee Surg Sports Traumatol Arthrosc 2020;28:100-7. [Google Scholar] [PubMed]
- 18. Huang X, Ye S, Li C, Luo Y, Li J, Zou M, et al. Simplified all-arthroscopic Broström technique in treatment of chronic lateral ankle instability in adolescents. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2025;39:457-61. [Google Scholar] [PubMed]
- 19. Takao M, Jujo Y, Iwashita K, Inagawa M, Chua EN, Lee KJ, et al. Arthroscopic modified lasso-loop stitch technique for chronic lateral ankle instability in skeletally immature vs mature patients. Foot Ankle Int 2024;45:373-82. [Google Scholar] [PubMed]
- 20. Guelfi M, Knörr J, Ruscigno G, Malagelada F, Pantalone A, Vega J. Excellent functional outcomes without physeal violation after arthroscopic all-inside ligament repair for ankle instability in skeletally immature patients. J Exp Orthop 2026;13:e70683. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report
August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report August 1, 2026 Serendipitous Healing of a Congenital Pseudoarthrosis of the Clavicle Following Acute Injury: A Case Report
August 1, 2026 Serendipitous Healing of a Congenital Pseudoarthrosis of the Clavicle Following Acute Injury: A Case Report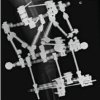 July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases
July 1, 2026 Step-cut and Butterfly Femoral Osteotomies Following Intraoperative Fracture Propagation during Distraction Osteogenesis: Report of Two Cases July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis
July 1, 2026 Beyond the Biopsy: Macrodystrophia Lipomatosa Unmasked After False Osteochondroma Diagnosis