
Recurrent foot swelling in a child that fails to behave as expected for an osteochondroma should prompt MRI-guided reassessment and consideration of macrodystrophia lipomatosa, as the two conditions share clinical, radiological, and histopathological features that can lead to misdiagnosis and avoidable surgical failure.
Dr. Siddhartha Sharma, Department of Orthopaedic Surgery, Postgraduate Institute of Medical Education and Research, Chandigarh, India. E-mail: sids82@gmail.com
Abstract
Introduction: Macrodystrophia lipomatosa (MDL) is a rare, non-hereditary congenital disorder of localised gigantism caused by disproportionate proliferation of fibroadipose tissue in all mesenchymal elements of the affected extremity. Its clinical, radiological, and histopathological features can closely mimic those of osteochondroma – the most common benign bone tumour – leading to misdiagnosis, inappropriate surgery, and rapid recurrence. We report a case in which a recurrent foot swelling in a child, twice confirmed as osteochondroma on histopathology, was revised to MDL and successfully managed with staged reconstruction.
Case Report: A 9-year-old male presented in 2024 with a progressively enlarging, recurrent swelling over the medial aspect of the right foot associated with overlying skin changes. The swelling had first been noted when the child began walking. Initial excision at an outside institution had yielded a histopathological diagnosis of osteochondroma arising from the head of the first metatarsal. Recurrence occurred within 2–3 months. Repeat biopsy in September 2020 again reported osteochondroma; a skeletal survey showed no additional lesions. By 2024, continued enlargement with soft-tissue involvement, friable overlying skin, and radiological features prompted a revised diagnosis of MDL. A two-stage surgical approach was undertaken. Stage one comprised wide local excision, polymethylmethacrylate (bone cement) spacer placement with K-wire stabilisation of the first metatarsal, and soft-tissue reconstruction using an anterolateral thigh free flap. Stage two involved removal of the cement, reconstruction of the first ray with a fibular strut graft fixed with a foot plate and intramedullary K-wire, and simultaneous flap debulking. The patient progressed from non-weight-bearing to full weight-bearing at 1 month postoperatively.
Results: At 20 months of follow-up, the child ambulates independently and performs all activities of daily living without restriction. There is no clinical or radiological evidence of recurrence. A mild limitation in running and toe movement persists.
Conclusion: MDL can reliably masquerade as osteochondroma on both biopsy and imaging, particularly in the foot. Rapid post-excision recurrence with progressive soft-tissue involvement should trigger magnetic resonance imaging reassessment and reconsideration of the diagnosis. A staged reconstructive approach – wide excision, free flap coverage, and biological bone reconstruction – achieves durable functional recovery in most cases.
Keywords: Macrodystrophia lipomatosa, osteochondroma, foot swelling, misdiagnosis, fibular strut graft, staged reconstruction, pediatric orthopedics.
Recurrent post-excision bony swellings in children are uncommon, and when they occur, the treating clinician faces a critical diagnostic choice: is this true osteochondroma recurrence, or does the clinical behavior demand a revised diagnosis? Osteochondroma accounts for 20–50% of all benign bone tumours [1], and local recurrence following complete excision is well established in <2% of cases [2]. However, when recurrence is rapid and associated with progressive soft-tissue involvement, the diagnosis must be revisited. Macrodystrophia lipomatosa (MDL) is a rare, non-hereditary congenital disorder with localised gigantism characterised by disproportionate proliferation of fibroadipose tissue in all mesenchymal layers – subcutaneous tissue, muscle, periosteum, nerve sheaths, and bone marrow [3,4]. In the lower extremity, it follows the plantar nerve distribution, most commonly affecting the second and third digits [5]. Crucially, the periosteal nodularity of MDL – composed of chondroblasts, osteoblasts, and osteoclasts [6] – can histologically resemble the cartilaginous cap of an osteochondroma, creating a genuine risk of misclassification on biopsy alone. We present a case in which a recurrent foot swelling in a 9-year-old boy, confirmed as osteochondroma on two separate biopsies, was ultimately diagnosed with MDL based on clinical progression and imaging reassessment and successfully managed with a staged reconstructive surgical approach.
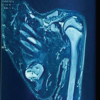
A 9-year-old male child presented to our centre in 2024 with a recurrence of swelling over the medial aspect of the right foot, which had progressively increased in size and was associated with changes in the overlying skin. In the detailed history, the swelling was first noticed shortly after the child began walking. It was insidious in onset and gradually progressive. Initial evaluation with radiographs and magnetic resonance imaging (MRI) revealed a lesion arising from the head of the first metatarsal. The patient underwent surgical excision at an outside institution, and histopathological examination confirmed the diagnosis of osteochondroma. Within 2–3 months following the initial surgery, the parents observed recurrence of the swelling at the same site, with a gradual increase in size. The lesion was initially managed with observation. A repeat biopsy performed in September 2020 reconfirmed the diagnosis of osteochondroma. A skeletal survey at that time did not reveal any additional lesions. The child remained under follow-up until presenting to our institution in 2024 with a progressively enlarging lesion, now associated with friable overlying skin (Fig. 1a and b). Plain radiographs were taken, which showed bony outgrowth from the distal part of the 1st metatarsal without any periosteal reaction (Fig. 1c). The diagnosis of MDL was made after getting an MRI, which revealed extensive soft-tissue hypertrophy and unencapsulated adipose tissue proliferation (Fig. 1d).
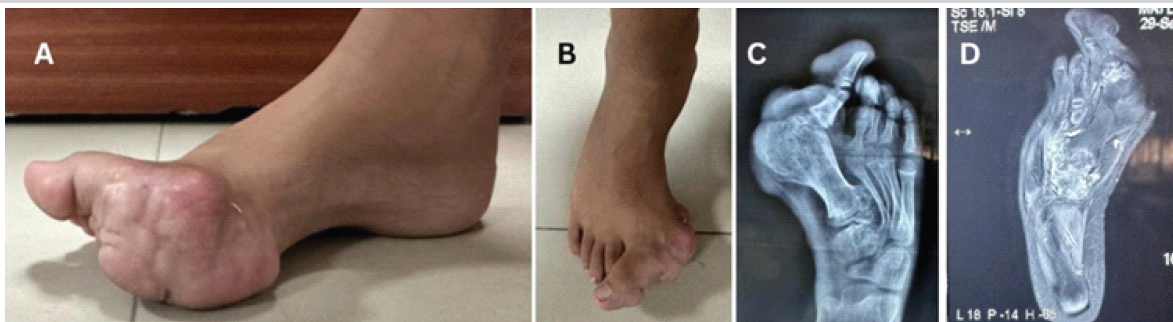
Figure 1: Status at presentation to our institute, (a and b) A large, ill-defined lobulated growth at the distal aspect of the first toe leading to hallux valgus deformity. (c) Plain radiograph showing bony outgrowth from the distal part of the 1st metatarsal, splaying of the distal metatarsal, degenerative changes in the joint surface, and marked localized soft-tissue hypertrophy. There is no periosteal reaction. (d) Magnetic resonance imaging showing bulky soft-tissue hypertrophy due to unencapsulated adipose tissue proliferation, a feature suggestive of macrodystrophia lipomatosa.
In view of the recurrent nature of the lesion and associated soft-tissue involvement, a staged surgical approach was planned. In the first stage, the patient underwent wide local excision of the tumour, reconstruction using polymethylmethacrylate (bone cement) with K-wire stabilisation of the first metatarsal (Fig. 2a and b), and soft-tissue coverage using an anterolateral thigh (ALT) free flap (Fig. 2c and d).
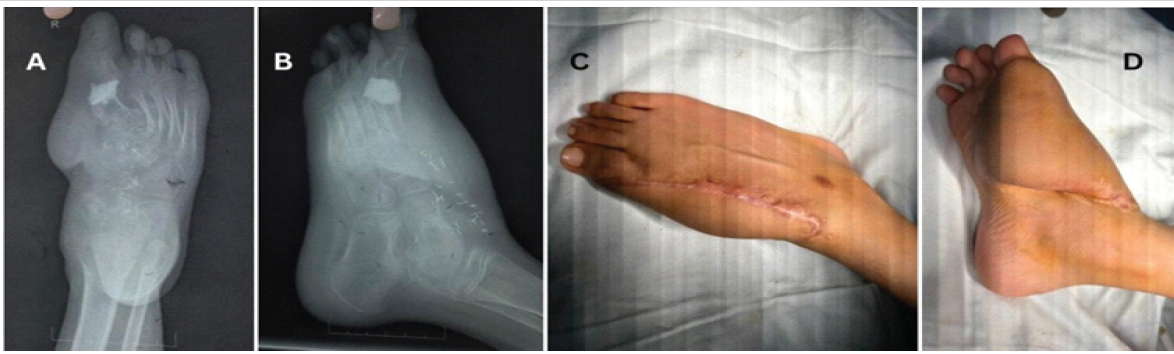
Figure 2: First stage, (a and b) post-operative radiograph after excision of the tumor and cement spacer placement. (c and d) Clinical picture showing good uptake of the anterolateral thigh free flap.
Postoperatively, the limb was immobilised, and the patient was maintained as non-weight-bearing. In the second stage, removal of the bone cement was performed, followed by reconstruction of the first ray using a fibular strut graft. Fixation was achieved using a footplate along with an intramedullary K-wire (Figs. 3 and 4).
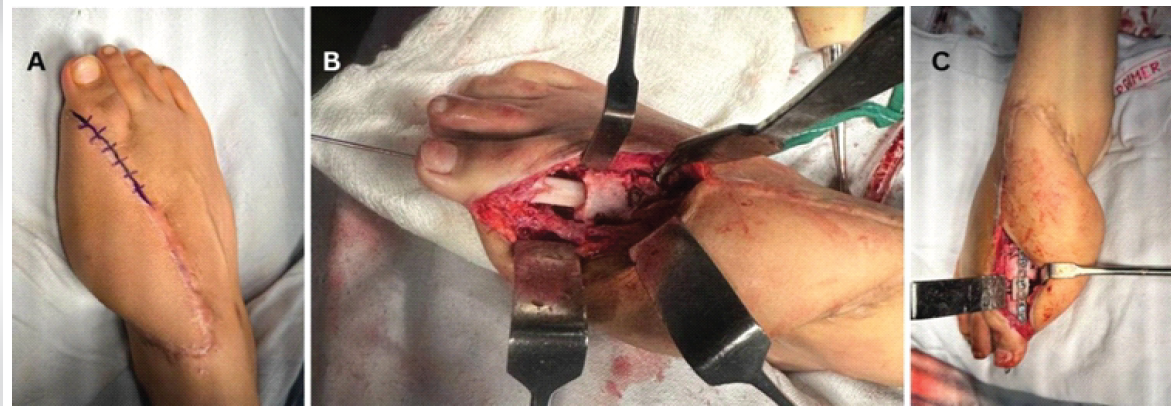
Figure 3: Intraoperative pictures of the second stage, (a) skin marking showing the planned skin incision. (b) Placement of fibula strut and stabilization with a K-wire. (c) Additional stabilization with the foot plate.

Figure 4: Radiographs immediately after the second-stage procedure.
Simultaneously, debulking of the flap was carried out. Postoperatively, gradual mobilisation was initiated, with partial weight-bearing at 1 month, progressing to full weight-bearing thereafter. At 20 months of follow-up, the child is able to perform activities of daily living independently, with no clinical or radiological evidence of recurrence (Figs. 5 and 6). He has no limitation in walking, although a mild limitation in running persists, which is mostly due to a new swelling that has arisen from the ipsilateral talus.

Figure 5: Clinical picture at 20 months follow-up.
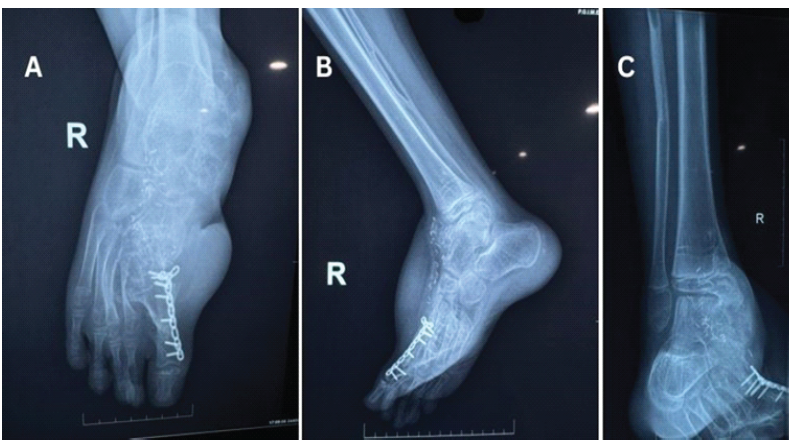
Figure 6: Plain radiograph at 20 months follow-up, (a and b) Excellent incorporation of fibula strut graft, and there is no recurrence of the tumor. (c) Complete regeneration of the fibula at the donor site; a new swelling that is arising from the talus is also evident, which requires further investigation.
This case illustrates a clinically important diagnostic pitfall: MDL mimicking osteochondroma, confirmed on repeat histopathology, with the correct diagnosis reached only after the lesion’s clinical behavior demanded a reassessment of the diagnosis. Osteochondroma is the most common benign bone tumour [1], and the lesion arose at the head of the first metatarsal, a site documented in the foot osteochondroma literature [7]. However, two features should have triggered earlier diagnostic scepticism: First, recurrence within 2–3 months is far outside the expected behavior of an incompletely excised osteochondroma; second, the rapid progressive soft-tissue involvement and overlying skin changes are inconsistent with a pure bony exostosis. The histopathological overlap is real and underappreciated. MDL’s periosteum is studded with nodules of chondroblasts, osteoblasts, and osteoclasts that enlarge distally [6], and these can be misread as the cartilaginous cap of an osteochondroma, particularly on small biopsy specimens. Day et al. specifically cautioned that a diagnosis of osteochondroma cannot stand without radiological proof of cortical-medullary continuity between the lesion and the parent bone [7]. The absence of this continuity – demonstrable on computed tomography or MRI – should exclude osteochondroma and widen the differential. MRI is the definitive discriminator. In osteochondroma, MRI confirms marrow continuity with the parent bone and allows measurement of the cartilaginous cap [1,8]. In MDL, MRI demonstrates abundant unencapsulated fibrofatty tissue with signal characteristics identical to normal subcutaneous fat on all sequences, linear hypointense fibrous bands, and the absence of cortical-medullary continuity [9,10]. Plain radiography in MDL shows soft-tissue lucency from adipose proliferation and characteristic distal widening of the phalanges – the “mushroom-like” appearance – described by Goldman and Kaye [6]. Regarding surgical management, there is no effective medical therapy for MDL [3]. Surgical indications include cosmetic disfigurement, functional impairment, and neurovascular compromise [3,5]. Simple debulking – the approach used at the outside institution and reported by Sudesh et al. [3] – carries a recurrence rate of 33–60% and a nerve injury rate of 30–50% [5,10]. For severe or aggressive cases, particularly the progressive subtype which predominates in foot involvement [11], a staged reconstructive approach is appropriate. Watt and Chung described a three-stage reconstruction for a severe pedal MDL case, achieving symmetrical shoe wear and normal gait by age 3 [11]. Their principle of allowing 6-month intervals for vascular recovery between stages informed our surgical planning. In our patient, the extent of the osseous defect and the compromised soft-tissue envelope necessitated the use of a cement spacer as a skeletal scaffold – maintaining alignment and length of the first ray while the ALT free flap established a durable soft-tissue cover. This two-stage strategy of biological reconstruction after soft-tissue maturation is well established in limb-salvage surgery. The fibular strut graft provided cortical support and biological incorporation. At 20 months, independent ambulation without recurrence is a satisfactory outcome for a case of this complexity.
MDL can closely mimic osteochondroma clinically and histologically. When a presumed osteochondroma recurs rapidly, demonstrates progressive soft-tissue involvement, or lies within the plantar nerve territory, the diagnosis must be reconsidered. Correlation of histopathology with MRI – specifically looking for fibrofatty tissue without cortical-medullary continuity – is essential for the correct diagnosis. A staged reconstructive approach, incorporating wide excision, free flap soft-tissue coverage, and fibular strut reconstruction, achieves durable functional recovery in severe recurrent paediatric cases.
- Histopathological confirmation of osteochondroma must always be correlated with imaging demonstrating cortical and medullary continuity between the lesion and the parent bone; without this, macrodystrophia lipomatosa cannot be excluded on biopsy alone
- Rapid post-excision recurrence, progressive soft-tissue involvement, or a lesion in the plantar nerve territory of the foot are red-flag features that should prompt magnetic resonance imaging reassessment and reconsideration of the primary diagnosis
- Staged reconstruction – wide local excision, free flap soft-tissue coverage, and biological bone grafting – is a viable and effective strategy for severe, recurrent macrodystrophia lipomatosa of the foot in children, achieving independent ambulation with no recurrence at 20 months.
References
- 1. Tepelenis K, Papathanakos G, Kitsouli A, Troupis T, Barbouti A, Vlachos K, et al. Osteochondromas: An updated review of epidemiology, pathogenesis, clinical presentation, radiological features and treatment options. In Vivo 2021;35:681-91. [Google Scholar] [PubMed]
- 2. Florez B, Mönckeberg J, Castillo G, Beguiristain J. Solitary osteochondroma long-term follow-up. J Pediatr Orthop B 2008;17:91-4. [Google Scholar] [PubMed]
- 3. Sudesh P, Raj N, Kumar R, Prakash S. Macrodystrophia lipomatosa. Foot (Edinb) 2012;22:172-4. [Google Scholar] [PubMed]
- 4. Çelebi F, Karagulle K, Oner AY. Macrodystrophia lipomatosa of the foot: A case report. Oncol Lett 2015;10:951-3. [Google Scholar] [PubMed]
- 5. Prasetyono TO, Hanafi E, Astriana W. A review of macrodystrophia lipomatosa: Revisitation. Arch Plast Surg 2015;42:391-406. [Google Scholar] [PubMed]
- 6. Goldman AB, Kaye JJ. Macrodystrophia lipomatosa: Radiographic diagnosis. Am J Roentgenol 1977;128:101-5. [Google Scholar] [PubMed]
- 7. Day FN, Ruggieri C, Britton C. Recurrent osteochondroma. J Foot Ankle Surg 1998;37:162-4; discussion 173. [Google Scholar] [PubMed]
- 8. Bovée JV. Multiple osteochondromas. Orphanet J Rare Dis 2008;3:3. [Google Scholar] [PubMed]
- 9. Blacksin M, Barnes FJ, Lyons MM. MR diagnosis of macrodystrophia lipomatosa. AJR. Am J Roentgenol 1992;158:1295-7. [Google Scholar] [PubMed]
- 10. Khan RA, Wahab S, Ahmad I, Chana RS. Macrodystrophia lipomatosa: Four case reports. Ital J Pediatr 2010;36:69. [Google Scholar] [PubMed]
- 11. Watt AJ, Chung KC. Macrodystrophia lipomatosa: A reconstructive approach to gigantism of the foot. J Foot Ankle Surg 2004;43:51-5. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report
August 1, 2026 Surgical Excision of a Rare Ventral Scapular Osteochondroma using the Prone “Chicken-Wing” Position: A Case Report February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report
February 1, 2026 Symptomatic Ventromedial Scapular Osteochondroma Presenting with Restriction of Shoulder Movements: A Case Report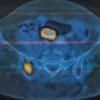 August 1, 2026 Understanding Diagnostic Challenges in Ewing Sarcoma – A Report of Two Cases
August 1, 2026 Understanding Diagnostic Challenges in Ewing Sarcoma – A Report of Two Cases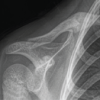 August 1, 2026 Serendipitous Healing of a Congenital Pseudoarthrosis of the Clavicle Following Acute Injury: A Case Report
August 1, 2026 Serendipitous Healing of a Congenital Pseudoarthrosis of the Clavicle Following Acute Injury: A Case Report