
In Sprengel deformity associated with thoracic deformity, particularly spondylocostal dysostosis, addressing severe downward scapular rotation with a modified Wilkinson procedure incorporating a Y-shaped osteotomy may be essential for achieving meaningful functional improvement.
Dr. Yuta Tsukagoshi, Department of Orthopaedic Surgery, Institute of Medicine, University of Tsukuba, Tsukuba - 305-8575, Japan. E-mail: most_valuable_swimmer@tsukuba-seikei.jp
Abstract
Introduction: Sprengel deformity is a rare congenital anomaly caused by failure of normal scapular descent during embryogenesis. Spondylocostal dysostosis (SCDO) is a genetically heterogeneous disorder characterized by vertebral segmentation defects and rib malformations. Reports describing the coexistence of these two conditions are scarce, and optimal surgical management remains unclear.
Case Report: A 6-year-old girl presented with limited elevation of the left shoulder and visible scapular asymmetry. Imaging demonstrated elevation, medial displacement, and severe downward rotation of the scapula, associated with rib malalignment and cervicothoracic segmentation anomalies consistent with SCDO. We performed a modified Wilkinson procedure incorporating a Y-shaped scapular osteotomy to achieve both caudal repositioning and rotational correction.
Conclusion: At 1 year postoperatively, shoulder elevation was nearly symmetric, and at 18 months, the patient had no functional limitations. In cases of Sprengel deformity associated with SCDO, severe downward rotation may necessitate a rotationally corrective osteotomy rather than descent alone.
Keywords: Sprengel deformity, spondylocostal dysostosis, modified Wilkinson procedure, and Y-shaped osteotomy.
Sprengel deformity is a rare congenital anomaly of the scapula and results from failed caudal migration during early foetal development. The deformity produces an elevated, hypoplastic, and malrotated scapula, frequently associated with functional limitation and cosmetic asymmetry [1,2]. Although it may occur as an isolated abnormality, Sprengel deformity often coexists with rib malformations, cervical fusion, or scoliosis [3]. Spondylocostal dysostosis (SCDO) is a congenital disorder characterised by vertebral segmentation defects and intrinsic rib malformations resulting from mutations affecting somitogenesis. Reports describing the coexistence of Sprengel deformity and SCDO are rare, although a case series identified Sprengel deformity in one of 13 SCDO patients, suggesting that this association may be underrecognised [4]. Additional studies have noted rib and vertebral anomalies among children with Sprengel deformity and spinal dysraphism, supporting the concept of shared developmental pathways [3]. Surgical correction of Sprengel deformity has historically focused on inferior scapular repositioning as described by Green and Woodward [1,5]. However, these approaches do not directly address rotational deformities. Wilkinson introduced scapular osteotomy to correct severe malrotation, offering advantages in selected patients [6]. Japanese clinical work has expanded on this, demonstrating that Y- and V-shaped scapular osteotomies can achieve improved rotational alignment and shoulder elevation when downward rotation is prominent [7,8]. Despite these developments, little has been published regarding surgical strategies for Sprengel deformity in the context of thoracic deformity as seen in SCDO. This report describes a child with Sprengel deformity associated with SCDO who underwent a modified Wilkinson procedure with favourable results.
A 6-year-old girl was referred for evaluation of persistent limitation of the left shoulder motion and progressive cosmetic deformity. The left shoulder movement had first been noted to be abnormal at approximately 1 year of age, and she was diagnosed with Sprengel deformity and cervical spine anomalies at 1 year and 10 months. Because she had no significant limitations in her activities of daily living or shoulder pain, she was managed conservatively until referral to our institution at age 5. Her prenatal and perinatal histories were unremarkable, and her growth and development were age-appropriate. No relevant family history was noted. Physical examination revealed elevation of the left scapula with obvious asymmetry. Left shoulder flexion was limited to 70° and abduction to 80°, whereas the right side demonstrated a full range of motion (Fig. 1).
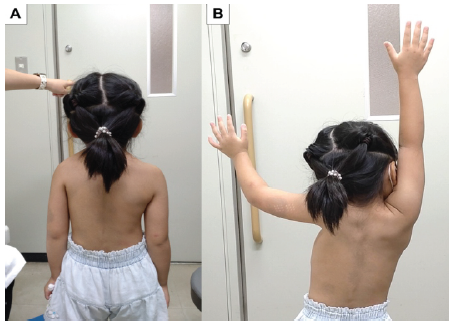
Figure 1: Clinical photographs of the back. Clinical photographs of the her back with the arms at rest (a) and during attempted elevation (b). Severe limitation of left shoulder flexion is evident.
Cervical rotation was mildly restricted. The left scapula was positioned in elevation and adduction and exhibited pronounced downward rotation with minimal upward rotation during attempted arm elevation. Radiographs demonstrated elevation of the scapula, medial displacement, and distinct downward rotation (Fig. 2).
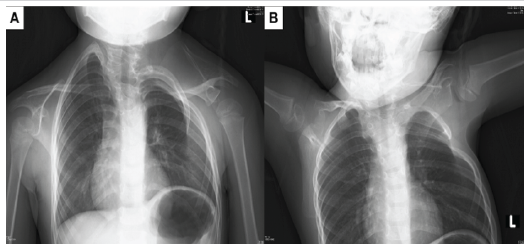
Figure 2: Plain radiographs of the shoulder girdle. Plain radiographs obtained in the resting position (a) and during arm elevation (b). Elevation of the left scapula is evident, accompanied by deformities of the spine and ribs.
The inferior angle of the scapula was positioned higher than that of the contralateral side, and rib alignment abnormalities and partial rib fusion were evident. Computed tomography showed segmentation anomalies from C4 to T2, deformity, and irregular alignment of the first to fourth ribs on the left side, and the presence of a hemivertebra (Fig. 3).
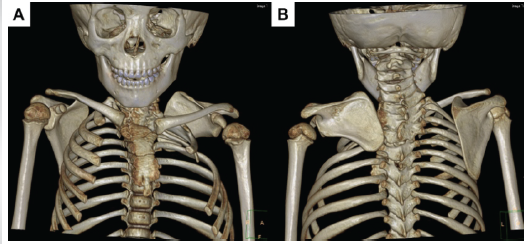
Figure 3: Three-dimensional computed tomography images. Three-dimensional computed tomography images of the chest showing anterior (a) and posterior (b) views. The left scapula demonstrates elevation, adduction, and pronounced downward rotation, together with fusion and deformities of the ribs and cervicothoracic vertebrae.
These findings were consistent with SCDO. An omovertebral bone was not identified on imaging. The Sprengel deformity was classified as Cavendish grade III [9]. Her left scapula was severely elevated and downward rotated, resting on deformed left ribs. Because severe downward rotation was considered a major contributor to the functional impairment and because simple caudal transposition was unlikely to provide adequate correction, we selected a modified Wilkinson procedure. A Y-shaped osteotomy was created at the medial scapular border to achieve both caudal repositioning and rotational realignment. The rhomboid muscles were preserved to maintain physiological scapular stability, and the scapula was placed beneath the latissimus dorsi to minimise postoperative winging according to Leibovic’s method [2,7] (Figs. 4 and 5).
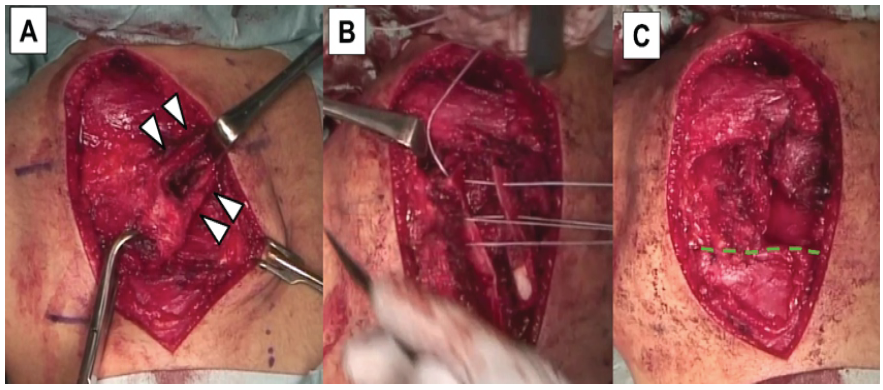
Figure 4: Intraoperative findings and surgical procedure. An omovertebral band (arrowheads) was identified within the rhomboid major muscle (a). A Y-shaped osteotomy was performed along the medial border of the scapula, followed by caudal translation and fixation of the medial and lateral fragments with fiber wires (b). The inferior angle of the scapula was positioned and secured within a latissimus dorsi muscle pocket (dashed line) (c).
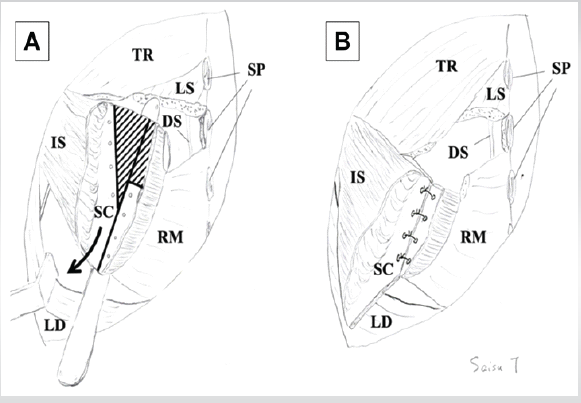
Figure 5: Surgical schematic of scapular Y-shaped osteotomy. Solid lines indicate the lines of osteotomies. Shaded lines indicate the areas to be resected. The black arrow indicates the direction of the pull-down of the scapula (a). After pulling down and suturing the lateral fragment of the scapula (b). DS: Dorsal scapular nerve, IS: Infraspinatus, LD: Latissimus dorsi, LS: Levator scapulae, RM: Rhomboid major, SC: Scapula, SP: Spinous process, TR: Trapezius. The original paper described by Okada [7] is published under the CC BY license. Therefore, no request for permission to reprint is required.
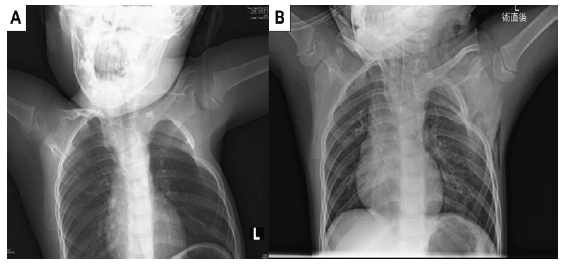
Figure 6: Pre-operative and immediate post-operative radiographs. Pre-operative (a) and immediate post-operative (b) radiographs obtained in the arm-elevated position. Upward rotation of the left scapula improved postoperatively, enabling elevation of the left upper limb.
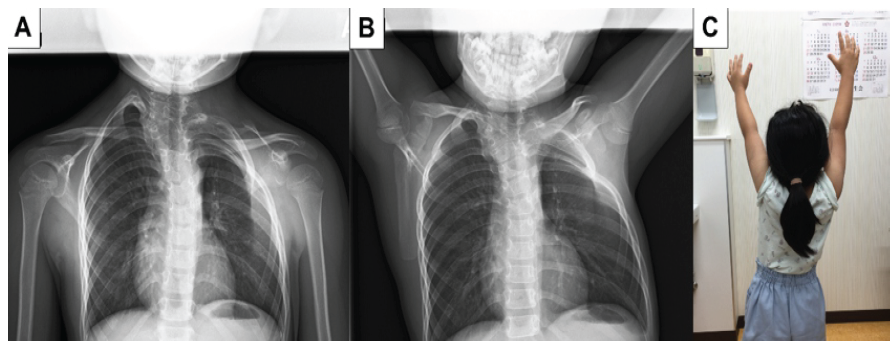
Figure 7: Radiographic and clinical outcomes at 1-year follow-up. Radiographs obtained in the resting position (a) and during elevation (b), and a clinical photograph of the back with the arms elevated (c) at 1-year follow-up. Shoulder abduction was possible without restriction of upward scapular rotation.
Post-operative recovery was uneventful. At 1-year follow-up, radiographs showed improved scapular position and rotation, and left shoulder flexion had improved to 150°, allowing the patient to swim freestyle (Fig. 7).
Sprengel deformity demonstrates wide variability in severity depending on the degree of elevation, dysplasia, and scapular rotation. Foundational techniques by Green and Woodward emphasised releasing abnormal soft-tissue attachments and achieving inferior scapular transposition [1,5]. Subsequently, the Wilkinson procedure was developed to achieve more reliable scapular descent while preserving the rhomboid muscles by performing a longitudinal osteotomy of the scapula and inferiorly translating the lateral fragment [6]. However, because Saisu observed persistent post-operative downward scapular rotation following the Wilkinson procedure, they refined the technique and devised a modified Wilkinson procedure incorporating a Y-shaped scapular osteotomy (Y-osteotomy) [7,8]. Recent biomechanical and clinical studies have highlighted the significance of downward scapular rotation as a major impediment to post-operative improvement in shoulder elevation. Investigations by Saisu demonstrated that persistent downward rotation can limit shoulder motion even when adequate scapular descent has been achieved [8]. These findings support surgical strategies that incorporate rotational correction, particularly in patients with severe deformity. Rib fusion and asymmetric thoracic growth in SCDO functionally block upward scapular rotation, thereby making descent-only procedures biomechanically insufficient. This explains why Wilkinson’s osteotomy, which directly resolves rotational malalignment, becomes essential in this subset rather than simply preferable. Consequently, rotational correction should not be considered an adjunct manoeuvre but rather the primary target when thoracic constraint prevents physiologic scapular motion. The presence of SCDO complicates the condition further. Thoracic malformation in SCDO does not simply coexist with Sprengel deformity but structurally augments downward scapular rotation by blocking upward rotational excursion against rigid rib fusion. Therefore, corrective descent alone becomes mechanically insufficient, justifying osteotomy-based rotational reconstruction as the primary surgical aim. This biomechanical constraint has been documented in SCDO case series and reports describing coexisting Sprengel deformity [4,10,11,12,13,14]. In such cases, descent-only procedures based on Green or Woodward techniques may be insufficient to restore shoulder biomechanics. In addition, rotational deformity that is inadequately corrected during the initial surgery may necessitate revision. Carson et al. and Leibovic et al. also highlighted the importance of addressing both elevation and rotation when assessing congenital scapular anomalies [2,13]. Thus, osteotomy-based procedures have an increasing role in complex cases. In the present case, the modified Wilkinson procedure enabled both controlled scapular descent and rotational realignment through a Y-osteotomy. This dual correction strategy is consistent with the recommendations of prior anatomical and clinical studies emphasising the importance of addressing scapular rotation [5,9]. Preservation of the rhomboids and placement beneath the latissimus dorsi likely contributed to dynamic stability and minimised postoperative winging. Particular attention was given to the risk of C5 traction neuropraxia and atlantoaxial rotatory subluxation, major complications described in systematic reviews [14]. Neither occurred in our case. This technique preserves the rhomboid major muscle, thereby allowing scapular abduction; as a result, dorsal traction on the clavicle is avoided, and compression of the brachial plexus is prevented, making it an effective surgical approach for reducing the risk of brachial plexus palsy without clavicular osteotomy. Although Sprengel deformity associated with SCDO remains rare, this case adds meaningful data to the limited literature on operative management. Continued accumulation of similar cases will be necessary to refine indications and determine long-term outcomes.
A modified Wilkinson procedure with a Y-osteotomy achieved substantial improvement in function and appearance in a child with Sprengel deformity associated with SCDO. In cases with severe downward rotation exacerbated by thoracic deformity, this approach may offer a rational and effective alternative to descent-only techniques. Our observations support the emerging concept that, in thoracic-restrictive variants of Sprengel deformity, rotational dominance rather than elevation alone defines surgical success.
In Sprengel deformity associated with thoracic deformities such as SCDO, severe downward scapular rotation may limit functional improvement with descent-only procedures. A modified Wilkinson procedure incorporating a scapular Y-shaped osteotomy may provide effective correction and improve shoulder function in patients with pronounced downward rotation.
References
- 1. Green WT. Surgical correction of congenital elevation of the scapula. J Bone Joint Surg Am 1972;39A:1439-48. [Google Scholar] [PubMed]
- 2. Leibovic SJ, Ehrlich MG, Zaleske DJ. Sprengel deformity. J Bone Joint Surg Am 1990;72:192-7. [Google Scholar] [PubMed]
- 3. Van Aalst J, Vles JS, Cuppen I, Sival DA, Niks EH, Van Rhijn LW, et al. Sprengel’s deformity and spinal dysraphism: Connecting the shoulder and the spine. Childs Nerv Syst 2013;29:1051-8. [Google Scholar] [PubMed]
- 4. Teli M, Hosalkar H, Gill I, Noordeen H. Spondylocostal dysostosis: Clinical review of thirteen cases including one associated with Sprengel deformity. Spine 2004;29:191-7. [Google Scholar] [PubMed]
- 5. Woodward JW. Congenital elevation of the scapula. J Bone Joint Surg Am 1961;43:219-28. [Google Scholar] [PubMed]
- 6. Wilkinson JA, Campbell D, Parsons SW. Scapular osteotomy for Sprengel’s shoulder. J Bone Joint Surg Br 1984;66:486-90. [Google Scholar] [PubMed]
- 7. Okada M, Tanaka N, Suzuka T, Kadoya Y, Saisu T, Kawaguchi M. Anesthetic management of scapular Y-osteotomy using suprascapular nerve block and erector spinae plane block for Sprengel deformity associated with Klippel-Feil syndrome: A case report. JA Clin Rep 2023;9:55. [Google Scholar] [PubMed]
- 8. Saisu T. Disorders of the shoulder in children – congenital elevation of the scapula (Sprengel deformity). Orthopedics 2019;42:599-604. [Google Scholar] [PubMed]
- 9. Cavendish ME. Congenital elevation of the scapula. J Bone Joint Surg Br 1972;54:395-408. [Google Scholar] [PubMed]
- 10. Balaji S. Spondylocostal dysostosis with Sprengel deformity: A rare association. Int J Res Orthop 2017;3:1123-6. [Google Scholar] [PubMed]
- 11. Anuradha DS, Reddy KJ, Reddy KR. Spondylocostal dysostosis with Sprengel deformity: A case report. Int J Contemp Pediatr 2018;5:1675-8. [Google Scholar] [PubMed]
- 12. Bindu CM, Krishnappa J, Hegde P, Bharath M. Jarcho-Levin syndrome (spondylocostal dysostosis) associated with sprengel deformity. J Clin Sci Res 2017;6:46-9. [Google Scholar] [PubMed]
- 13. Carson WG, Lovell WW, Whitesides TE. Congenital elevation of the scapula. J Bone Joint Surg Am 1972;63:1199-207. [Google Scholar] [PubMed]
- 14. Zarantonello P, Di Gennaro GL, Todisco M, Cataldi P, Stallone S, Evangelista A, et al. Surgical treatment of sprengel’s deformity: A systematic review and meta-analysis. Children (Basel) 2021;8:489. [Google Scholar] [PubMed]




Related Articles in Journal of Orthopaedic Case Reports
 March 10, 2024 Bilateral Sprengel Deformities, Mirror Movements Synkinesis, and Arthrogryposis Multiplex Congenita: A Novel Combination
March 10, 2024 Bilateral Sprengel Deformities, Mirror Movements Synkinesis, and Arthrogryposis Multiplex Congenita: A Novel Combination January 10, 2016 Young Adult Hip: Reactivation of dormant, previously undiagnosed Mycobacterium Tuberculosis infection following intra-articular steroid injection
January 10, 2016 Young Adult Hip: Reactivation of dormant, previously undiagnosed Mycobacterium Tuberculosis infection following intra-articular steroid injection February 10, 2021 Limb Salvage Surgery in Fungating Giant Cell Tumors: A Report of Three Cases
February 10, 2021 Limb Salvage Surgery in Fungating Giant Cell Tumors: A Report of Three Cases February 1, 2026 Surgical Management of Volar Lip Fractures of the Middle Phalanx: A Case Series on Diverse Techniques and Outcomes, Do Acute and Chronic Presentations Differ in Outcome?
February 1, 2026 Surgical Management of Volar Lip Fractures of the Middle Phalanx: A Case Series on Diverse Techniques and Outcomes, Do Acute and Chronic Presentations Differ in Outcome?