
Post-immunization quadriceps contracture should be a differential for quadriceps contracture in a child. Distal quadricepsplasty with alternate sliding hemisectioning of the vastus intermedius offers good functional outcomes with almost no complications.
Pritam Kumar Panda, Department of Orthopedics, VSSIMSAR, Burla, Sambalpur 768017, Odisha, India. E-mail: pritampanda57@gmail.com
Abstract
Introduction: Quadriceps contracture is a condition of shortening and fibrosis of the quadriceps muscle, resulting in restriction of various ranges of flexion of the knee. It commonly affects the children’s age group who are immunised through the intramuscular route. Intramuscular immunization remains a potential cause of the problem, among other causes. Sound evaluation and surgical release of contracture are warranted in cases where conservative management with physiotherapy has failed to provide pain-free and adequate knee movements for routine activities.
Materials and Methods: Subjects with post-immunisation contracture were treated by open quadriceps release with Z-plasty of the rectus femoris and fractional lengthening of the vastus intermedius with knee immobilisation 3 weeks post-surgery, followed by quadriceps physiotherapy for range of movement exercises as tolerated by the patient. Follow-up was done at 3, 6, 12, and 24 weeks. Pre- and post-knee ranges of motions were compared.
Results: Immediate post-release knee flexion range was significantly improved, attaining an acceptable range of flexion in nearly about 12 weeks for routine outdoor activities. No complication was reported apart from a few degrees of extensor lag.
Conclusion: Distal procedure with Z-plasty and fractional lengthening can be considered a fair technique of addressing quadriceps contracture with minimal complications and a good anticipated outcome.
Keywords: Quadriceps contracture, quadricepsplasty, intramuscular injection, Z-plasty.
Quadriceps contracture is a condition characterised by shortening and fibrosis of the quadriceps muscle due to multiple causes, such as congenital/idiopathic, trauma, infection, or muscular injections [1]. In the recent past, it was more common following intramuscular injections due to its application in the anterior aspect of the thigh to prevent sciatic nerve palsy in children with less developed gluteal muscles [2]. Children with this condition usually present with a fully extended, stiff knee, which leads to limping, awkward sitting, difficulty in squatting, and hampering of various activities. Severe cases may be associated with genu recurvatum, congenital knee dislocation, patella alta, and habitual patella dislocation [3].
In our case series, we have reported six children of different age groups who presented to our hospital at different times with complaints of inability to squat and fold their legs. There was difficulty in running, playing, walking, and all sorts of routine activities, as noticed by their parents. Initially, they were advised to attend physiotherapists; however, the results were insignificant and unsatisfactory. In all cases, deformities were painless and progressive. Although they had no history of trauma, infection, or any other congenital anomalies, all of them had received multiple intramuscular injections to the anterior thigh aspect as a routine procedure of immunisation during their infancy. In due course of time, a cord-like band was formed without any evidence of ulceration, which was responsible for the restriction of knee flexion (Fig. 1).

Figure 1: Restriction of left knee flexion.
In all cases, examination has revealed no genu recurvatum, genu valgum, subluxation of tibia, or habitual dislocation of patella. Wasting of the thigh was there. Ely’s test was negative in all of them, indicating pathology lies in combined quadriceps forms rather than rectus femoris alone, for which distal release was planned. Neurological examination was normal. The X-ray was normal and revealed no evidence of patellar hypoplasia, flattening of the femoral condyle, or any degenerative changes. Based on all these findings, a diagnosis of post-injection quadriceps contracture was made (Table 1).
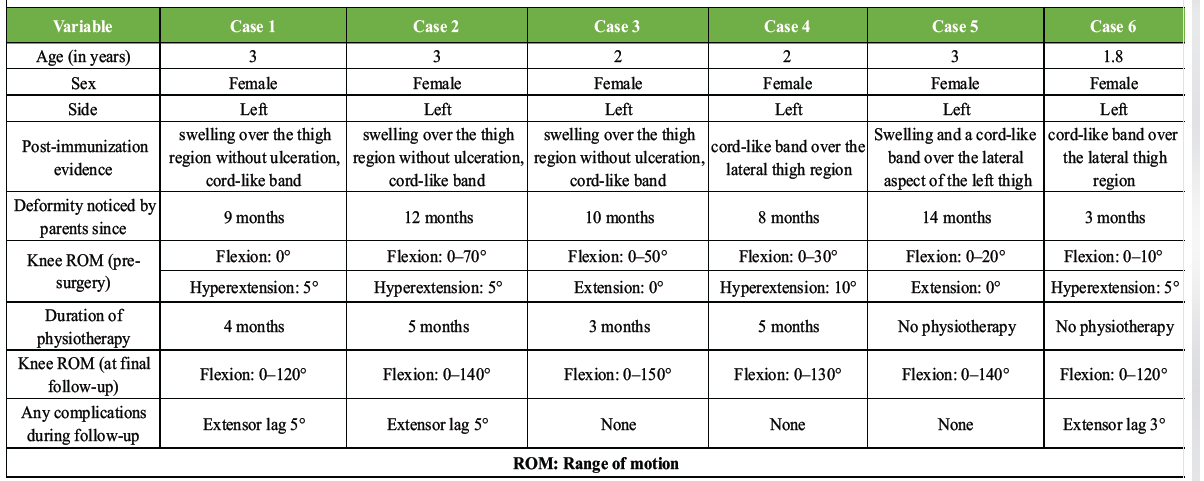
Table 1: Table briefly summarizing case demographics, cause, duration, pre and postoperative range of movements and complications
All children were operated on in the supine position under general anaesthesia supplemented with a caudal block. A longitudinal 8 cm anterolateral incision was given over the distal aspect of the thigh, falling just short of the patella. The quadriceps tendon was identified as a whitish, glistening, tight structure following skin, subcutaneous, and fascial dissection (Fig. 2).

Figure 2: Tendon of the rectus femoris.
It was traced from the upper pole of the patella till proximally, where the rectus femoris blends with it, and the rectus was isolated. Subsequently, the vastus lateralis was isolated from the lateral edge of the rectus by blunt dissection from the distal to proximal direction. However, the vastus medialis was isolated only proximally to avoid injury to the medial superior genicular vessels. The adhesion between the rectus and vastus intermedius was separated bluntly. Lengthening of the rectus was achieved by sliding Z-plasty or Z-tenotomy with the distal horizontal limb exiting laterally and the proximal horizontal limb exiting medially. Knee flexion was roughly 140° till this stage. Further to increase the knee flexion, Intermedius was given a fractional lengthening through alternate sliding hemisectioning release (Fig. 3), which achieved the knee flexion up to roughly 160° (Fig. 4).
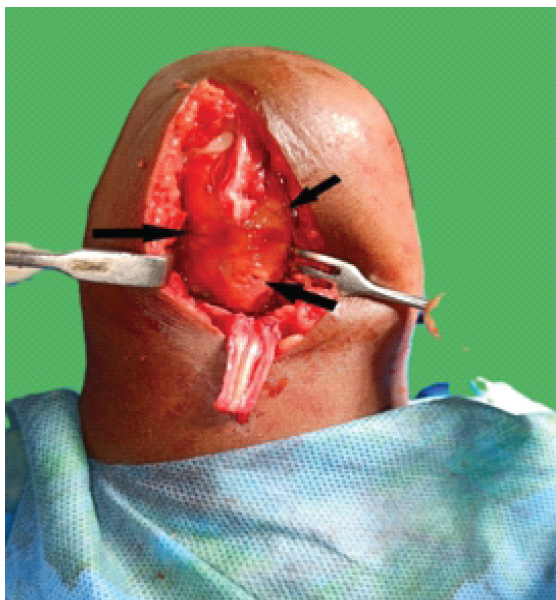
Figure 3: Showing Z tenotomy of rectus with alternate sliding hemisectioning release of vastus intermidius (black arrows).

Figure 4: Range of intraoperative flexion achieved.
Cut ends of the rectus were repaired with 3.0 prolene in maximal flexion, to which both medial and lateral vastii were approximated to aid healing of the distal tendinous structure (schematic diagram of procedure Fig. 5).
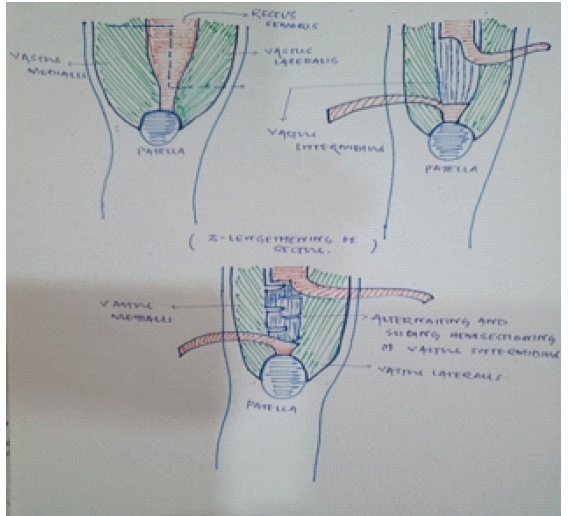
Figure 5: Schematic diagram of intraoperative release (Z tenotomy of rectus with alternating and sliding hemisectioning of the vastus intermedius).
Haemostasis was achieved, and the wound was closed in layers. The knee was immobilised in 100° of flexion using a plaster cast application. Post-surgery, all were kept non-weight-bearing for a period of 3 weeks. Following suture removal, static quadriceps exercise and both active and passive knee range of motion were encouraged under the supervision of a physiotherapist. Protected weight-bearing was allowed during this time with the use of braces. There was improvement in knee flexion with subsequent visits. On each visit, patients were encouraged to walk with full extension and to increase the knee flexion range with physiotherapist guidance and to practise the same at their home.
The quadriceps femoris is the primary extensor of the knee joint, and contracture leads to extension contracture of various grades, leading to loss of flexion of the knee joint. It limits day-to-day activities, such as running, jumping, climbing stairs, squatting, and cross-legged ground sitting, which is a common scenario for the Indian population, and thus decreases the playtime in the children’s age group, the disability affecting their lives significantly. Most often, the components of the quadriceps to undergo this change are the rectus femoris and vastus intermedius [4]. Various causes of this condition have been described in literature; prominent ones among them are trauma and immobilisation, congenital/idiopathic, infective, post-surgical, ischaemic myositis, post-traumatic myositis, and injection myositis [5]. Quadriceps contracture may be associated with habitual dislocation of the patella, genu recurvatum, anterior tibial subluxation, or patella alta [3]. Common to any age group, children under 5 years of age usually develop contracture following intramuscular injection [6]. The preferred route of vaccination in infants is intramuscular into the anterolateral aspect of the thigh in the quadriceps muscle due to ill-developed gluteal muscles and high chances of post-injection sciatic nerve palsy [3]. Quadriceps muscle contracture can be the rectus type, the vastus type, or the mixed type, and clinically it is important to differentiate the types depending on which the management is decided. Ely’s test is used to differentiate the rectus type from that of the vastus type. Mild grades of the deformity are managed with physiotherapy, but most cases demand surgical release of the contracture and adhesion, called ‘quadricepsplasty’ or ‘quadriceps release’. Various types of quadricepsplasty have been described by authors, such as Bennett’s V-Y plasty, Thompson’s quadricepsplasty, modified Thompson’s quadricepsplasty for distal release and Judet proximal release, Sengupta’s proximal release, Lenart and Kullmann’s proximal release of isolated rectus femoris contracture, etc. [7]. Early disease is usually dealt with proximal release, and late presenters are managed with distal release [8]. For a fully contracted quadriceps, distal release is indicated, while proximal release yields a better outcome in isolated rectus femoris contracture [9]. At present, there is no strict consensus as to what type of quadricepsplasty to perform, and this decision differs in each case; therefore, to get maximal effectiveness and outcome of the procedure, each case should be individually assessed and treated [8,9]. In our case series, we carried out distal quadricepsplasty with sliding Z-plasty/Z-tenotomy for rectus femoris lengthening with alternate sliding hemisectioning of vastus intermedius to aid in further flexion [10]. Results of the procedure were satisfactory, as the intraoperative knee flexion achieved was roughly 160°. From the pathogenesis point of view, research indicates the vastus intermedius is the most injured muscle, followed by the vastus lateralis and the rectus femoris, due to enclosure in a single osteo-fascial compartment with relatively poor blood supply. During intramuscular injection, when a large volume of fluid is confined to a closed space, it causes ischaemia, necrosis, and finally fibrosis [11,12], as evidenced by high sections of intermedius, as in the case of Judet’s procedure. All our patients had undergone alternate sliding hemisectioning of the vastus intermedius, which provides not only the integrity of the quadriceps required for full extension post-operatively but also lengthening to overcome the extension deformity as well. The age group affected in our series was under 5 years with a female predominance, whereas it was 3–7 years in a study carried out by Soumah et al. [13] and 6–10 years by Gbenou et al. [14]. Although knee flexion observed intraoperatively immediately after release was around 160° approximately, when these children were followed for a period of 6 months, the mean range of flexion was 133.33° (Fig. 6a and b).

Figure 6: (a and b) Flexion of the knee at 12 weeks follow-up.
At this point in time, the range of motion, both active and passive, observed was good, allowing all sorts of activities, and parents were fully satisfied with the result. The range of motion achieved in our series is greater as compared to flexion achieved by Burnei et al. using Judet and Payr-Thompson techniques [15]. A similar good outcome was also seen in thirty cases, as evidenced by the Mukherjee and Das study, where fifty cases of quadriceps contracture in thirty-seven children were treated by quadriceps elongation [16]. Extensor lag, which is a common complication in 70% of distal procedures as described by Jackson and Hutton, who studied 32 contractures of the quadriceps in 17 children comparing conservative versus distal quadriceps plasty, is also encountered in the present case series [11]. The average extensor lag was 3.33° at the end of the 3-month follow-up (Fig. 7).

Figure 7: Extension of knee at 12 weeks follow-up.
However, we have noticed the extensor lag is gradually improving on subsequent follow-ups as the children are fully weight-bearing in extension of the knee and continue range of motion under physiotherapist guidance. Delayed wound healing was observed in one of our cases, likely because of a lack of maintenance of hygiene on the part of the parents due to low socioeconomic status, which, in due course of time, healed at subsequent follow-ups. The rate of skin complications, such as necrosis, wound dehiscence, and haematoma, in our series is almost nil as compared to other studies [15,16].
Although this disease has become rare nowadays due to the use of intravenous routes for injectable drugs still its presentation in a child needs proper evaluation, correct release of tendons, and extended supervised physiotherapy post-surgery to achieve a successful clinical outcome. Irrespective of all, as recurrence is not uncommon, a close periodic follow-up is mandatory in all cases. Distal procedure with Z-plasty and fractional lengthening can be a fair technique to address quadriceps contracture with minimal complications and a good anticipated outcome.
Across the Case Series the authors would like to impress upon the readers that (a) Post-immunization quadriceps contracture is a disabling condition for the child during the playful age, and if not addressed properly, may lead to some form of permanent deformity when the child grows. (b) This condition poorly responds to conservative management. (c) The distal quadriceps procedure yields a good result with respect to the functional demands of the child, allowing for almost the full range of knee movements with no complications in absence of isolated rectus femoris contracture.
References
- 1. Gunn DR. Contracture of the quadriceps muscle. A discussion on the etiology and relationship to recurrent dislocation of the patella. J Bone Joint Surg Br 1964;46:492-7. [Google Scholar] [PubMed]
- 2. Mayer M, Romain O. Sciatic paralysis after a buttock intramuscular injection in children: An ongoing risk factor. Arch Pediatr 2001;8:321-3. [Google Scholar] [PubMed]
- 3. Williams PF. Quadriceps contracture. J Bone Joint Surg 1968;15-B:278-84. [Google Scholar] [PubMed]
- 4. Bose K, Chong KC. The clinical manifestations and pathomechanics of contracture of the extensor mechanism of the knee. J Bone Joint Surg Br 1976;58-B:478-84. [Google Scholar] [PubMed]
- 5. Biswas M, Sahoo SS. Post-injection quadriceps contracture treated with horizontal distal Z quadricepsplasty: A case report. J Orthop Case Rep 2024;14:173-7. [Google Scholar] [PubMed]
- 6. Hagen R. Contracture of the quadriceps muscle in children: A report of 12 cases. Acta Orthop 1968;39:565-78. [Google Scholar] [PubMed]
- 7. Shivaprasad MS, Kumar YC, Ravikumar TV, Koirala S. Surgical management of quadriceps contracture. Int J Sci Res 2015;4:1919-22. [Google Scholar] [PubMed]
- 8. Milcan A, Eskandari MM, Oztuna V, Colak M, Kuyurtar F. Injection-induced contracture of the quadriceps femoris muscle in children. Orthopedics 2004;27:65-6. [Google Scholar] [PubMed]
- 9. Diri D, Alasaad H, Mhana SA, Mackieh R. Proximal release for injections induced hip flexion contracture in a child: A case report. Int J Surg Case Rep 2023;102:107865. [Google Scholar] [PubMed]
- 10. Fitoussi F, Bachy M. Tendon lengthening and transfer. Orthop Traumatol Surg Res 2015;101 Suppl 1:S149-57. [Google Scholar] [PubMed]
- 11. Jackson AM, Hutton PA. Injection-induced contractures of the quadriceps in childhood. A comparison of proximal release and distal quadricepsplasty. J Bone Joint Surg Br 1985;67:97-102. [Google Scholar] [PubMed]
- 12. Boon RL, Baildam E. Progressive fibrosis of the quadriceps muscle. Arch Dis Child 2004;89:44. [Google Scholar] [PubMed]
- 13. Soumah MT, Sylla AI, Toure MR, Camara T, Kama ML, Diallo MB, et al. Quadriceps fibrosis following intramuscular injections into the thigh: Apropos of 92 cases at the Ignace Deen Central University hospital in Conakry. Med Trop (Mars) 2003;63:49-52. [Google Scholar] [PubMed]
- 14. Gbenou AS, Kpadonou GT, Fiogbe AM, Zoumenou E, Alao MJ. Iatrogenic retractile quadriceps fibrosis within children in Benin: Epidemiological, clinical, therapeutical aspects. Afr J Paediatr Surg 2013;10:211-6. [Google Scholar] [PubMed]
- 15. Burnei G, Neagoe P, Margineanu BA, Dan DD, Bucur PO. Treatment of severe iatrogenic quadriceps retraction in children. J Pediatr Orthop B 2004;13:254-8. [Google Scholar] [PubMed]
- 16. Mukherjee PK, Das AK. Injection fibrosis in the quadriceps femoris muscle in children. J Bone Joint Surg Am 1980;62:453-6. [Google Scholar] [PubMed]


Related Articles in Journal of Orthopaedic Case Reports
 February 10, 2024 Post-injection quadriceps contracture treated with horizontal distal Z quadricepsplasty: A Case Report
February 10, 2024 Post-injection quadriceps contracture treated with horizontal distal Z quadricepsplasty: A Case Report March 1, 2026 When the Hip Won’t Stay Quiet – Treating Snapping Hip Syndrome with Open Z-Plasty and Gluteus Maximus Release: A Case-Based Technical Insight
March 1, 2026 When the Hip Won’t Stay Quiet – Treating Snapping Hip Syndrome with Open Z-Plasty and Gluteus Maximus Release: A Case-Based Technical Insight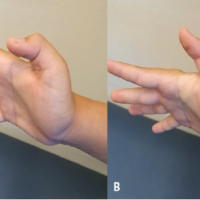 March 1, 2025 Single-stage reconstruction without grafting for neglected flexor pollicis longus tendon laceration in a child – A case report
March 1, 2025 Single-stage reconstruction without grafting for neglected flexor pollicis longus tendon laceration in a child – A case report January 6, 2014 Open Fracture of the Forearm Bones due to Horse Bite
January 6, 2014 Open Fracture of the Forearm Bones due to Horse Bite