
Single-screw and two-screw fixation in the Latarjet procedure yield comparable functional outcomes; accurate coracoid graft positioning and meticulous surgical technique are more critical determinants of success than the number of fixation screws
Dr. Onkar B Dhage, Department of Orthopaedics, Government Medical College and Hospital, Chhatrapati Sambhajinagar, Maharashtra, India. E-mail: onkardhage007gmail.com
Abstract
Background: Recurrent anterior shoulder instability associated with glenoid bone loss frequently requires surgical stabilisation. The Latarjet procedure addresses both bony deficiency and dynamic instability through a triple stabilizing mechanism. Controversy persists regarding the optimal method of coracoid graft fixation – single-screw versus two-screw – with ongoing debate about their biomechanical stability, complication profiles, and functional outcomes.
Materials and Methods: Materials and Methods: A prospective comparative study was conducted at the Department of Orthopaedics, Government Medical College and Hospital, Chh. Sambhajinagar, Chh. Sambhajinagar. Patients with recurrent anterior shoulder instability undergoing the Latarjet procedure were allocated to single-screw fixation (Group A) or two-screw fixation (Group B). Functional outcomes were assessed using the Constant-Murley score and clinical range of motion at follow-up. Radiological evaluation assessed graft union and positioning. Minimum follow-up was 3 months.
Results: Both groups were comparable at baseline. At final follow-up, both groups demonstrated significant improvement in functional outcomes, with comparable Constant-Murley scores and range of motion recovery. Radiological evaluation showed high graft union rates in both groups. Recurrence rates were low and comparable. Hardware-related irritation was slightly higher in the two-screw group, while operative time was marginally shorter in the single-screw group. No significant difference was observed between groups in functional outcome, graft union, recurrence, or complication rates.
Conclusion: Both single-screw and two-screw fixation techniques in the Latarjet procedure provide comparable functional outcomes, graft union, and recurrence rates. Accurate graft positioning and meticulous surgical technique appear to be more critical determinants of success than the number of fixation screws.
Keywords: Latarjet procedure, shoulder instability, coracoid graft, single-screw fixation, two-screw fixation, graft positioning, glenoid bone loss.
Recurrent anterior shoulder instability is a common problem in young active individuals, frequently associated with glenoid bone loss. Soft tissue stabilisation procedures alone may fail in the presence of significant bony defects, necessitating bony augmentation. The Latarjet procedure, first described by Michel Latarjet in 1954, is a bone-block stabilisation technique that addresses both bony deficiency and dynamic instability [1]. The procedure achieves its effect through a well-recognised triple stabilising mechanism: (1) bony augmentation of the glenoid articular surface through the transferred coracoid graft; (2) a dynamic sling effect produced by the conjoint tendon, which stabilises the humeral head in the position of abduction and external rotation; and (3) capsular repair reinforcement [2]. Although the Latarjet procedure is widely accepted as a reliable treatment for recurrent anterior shoulder instability with significant bone loss, controversy remains regarding the optimal method of coracoid graft fixation. Both single-screw and two-screw fixation techniques are employed in clinical practice. Two-screw fixation is often considered the biomechanical gold standard due to superior rotational stability of the coracoid graft, while single-screw fixation offers technical simplicity, shorter operative time, and reduced risk of graft fracture during drilling [3,4]. Equally critical to the fixation method is the accuracy of graft positioning. The coracoid graft must be placed flush with the anterior glenoid rim in the axial plane and below the glenoid equator in the sagittal plane (infero-anterior quadrant, targeting 3–5 o’clock on the right shoulder). Malpositioned grafts – whether too medial, causing persistent instability, or too lateral, causing increased contact pressure – predispose to poor outcomes and early arthritis [5,6,7,8,9,10]. This study aims to compare the clinical and radiological outcomes of single-screw versus two-screw fixation in the Latarjet procedure, with a focus on functional outcome, graft union, recurrence, and complication rates.
Study design and setting:
The study protocol was approved by the Institutional Ethics Committee, and written informed consent was obtained from all patients before inclusion in the study. A prospective comparative study was conducted in the Department of Orthopaedics, Government Medical College and Hospital, Chh. Sambhajinagar, India.
Inclusion and exclusion criteria:
Inclusion criteria:
- Recurrent anterior shoulder instability with documented glenoid bone loss on pre-operative computed tomography (CT)/magnetic resonance imaging (MRI)
- Age 18–40 years
- Failed conservative management or Bankart repair
- Minimum 3-month follow-up.
Exclusion criteria:
- Posterior or multidirectional instability
- Active infection
- Significant rotator cuff tear
- Prior Latarjet procedure on the same shoulder
- Inability to follow-up.
Surgical technique:
All surgeries were performed under general anesthesia in the beach-chair position using a standard deltopectoral approach. The coracoid process was osteotomized, the undersurface prepared, and the graft transferred through a subscapularis split to the anteroinferior glenoid. Graft positioning was confirmed intraoperatively and on post-operative imaging, targeting flush placement with the anterior glenoid rim (axial) and below the glenoid equator (sagittal). In Group A (single-screw), fixation was achieved with one cortical screw through the center of the coracoid graft. In Group B (two-screw), fixation was achieved with two parallel cortical screws. Capsular repair was performed in all cases. Post-operative rehabilitation followed a standardized protocol.
Outcome measures:
Functional outcomes were assessed using the Constant-Murley Score and clinical range of motion (forward flexion, abduction, external rotation) at 3 and 6 post-operatively. Radiological evaluation included plain X-rays (immediate post-operative and at follow-up) and CT scans where available, assessing graft union and positioning. Recurrence of instability and hardware-related complications were also recorded.
Statistical analysis:
Data were analyzed using the Statistical Package for the Social Sciences version 26.0. Continuous variables were expressed as mean ± standard deviation. Comparison between groups was performed using Student’s t-test for continuous variables and Chi-square test for categorical variables. A P < 0.05 was considered statistically significant.
Cases:
- A 23-year-old male with presented with instability at right shoulder, having multiple episodes of dislocation of shoulder anteriorly in past, operated 8 months back. Patient managed with Latarjet procedure with Single-screw fixation
- A 25-year-old male with 4 episodes of anterior shoulder dislocation on right side, first episode was during overhead throwing of ball, got operated 7 months back Patient managed with Latarjet procedure with Two-screw fixation (Figs. 1, 2, 3, 4, 5, 6, 7, 8)
- A 28-year-old female with history of recurrent shoulder dislocation on Right side, known case of Epilepsy since 12 years
- A 22-year-old male athlete with left sided recurrent anterior shoulder dislocation, first episode was during playing cricket 3 years ago, got operated a year ago
- A 45-year-old male with blunt trauma to Right shoulder 1 year ago complaing of shoulder dislocation for more than 3 times
- A 25-year-old male with pain in Right shoulder, having multiple episodes of shoulder dislocation in past, operative history of 6 months
- A 28-year-old male gymnast with 4–5 times anterior shoulder dislocation on right side, first episode was 3 years ago, got operated 8 months ago
- A 30-year-old male individual with shoulder instability on left side, was operated 6 months back.
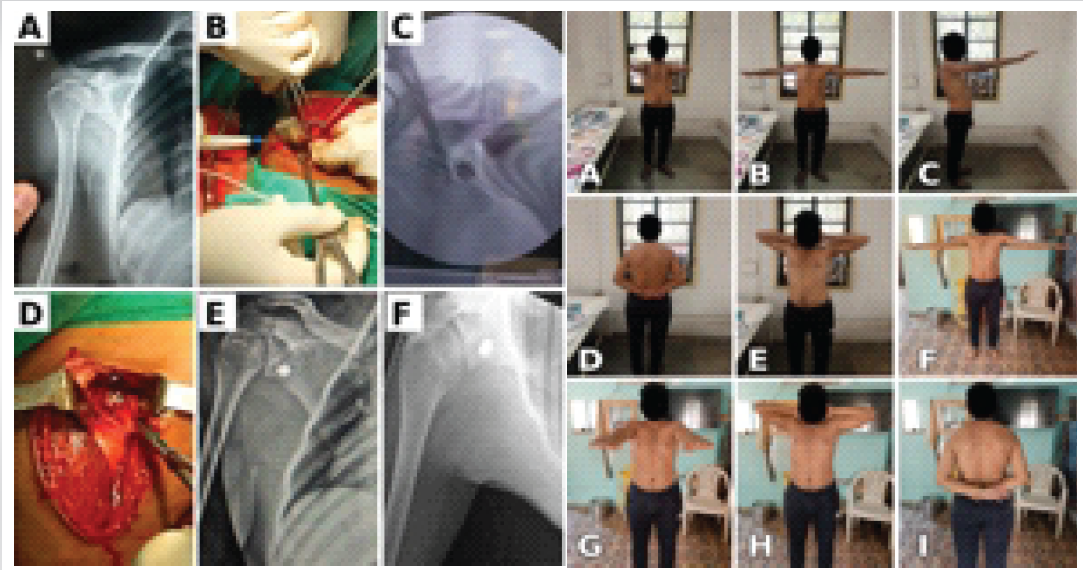
Figure 1: (a) Pre-operative X-ray (b, c, d) Intra-op images (e) Immediate post-operative X-ray (f) 3 month follow-up X-ray (a, b, c, d, e) follow-up range of motion at 3 months and (f, g, h, I) at 6 months
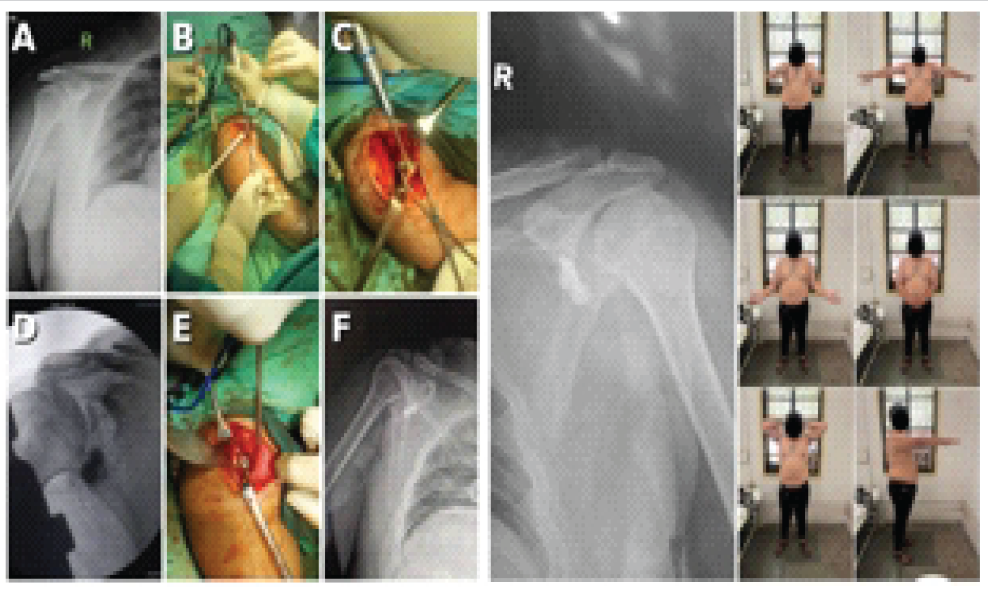
Figure 2: (a) Pre-operative X-ray (b, c, d, e) Intra-operative images (f) Post-operative X-ray
Follow-up X-ray and range of motion at 3 months.
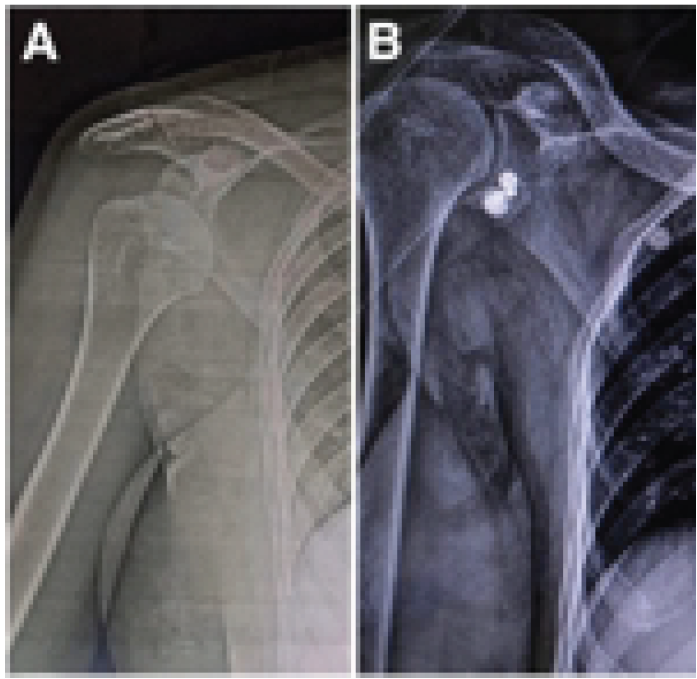
Figure 3[1.1]: (a) Pre-operative and (b) Post-operative X-rays of a 28-year-old female with recurrent right shoulder instability and epilepsy, showing the Latarjet procedure with two-screw fixation.
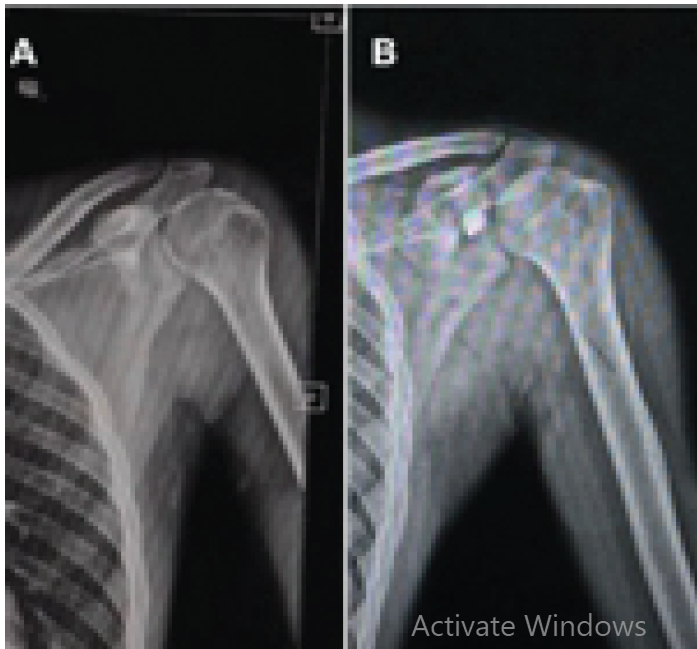
Figure 4[2.1]: (a) Pre-operative and (b) Post-operative X-rays of a 22-year-old male athlete with recurrent left anterior shoulder instability (cricket-related), showing the Latarjet procedure with single-screw fixation.
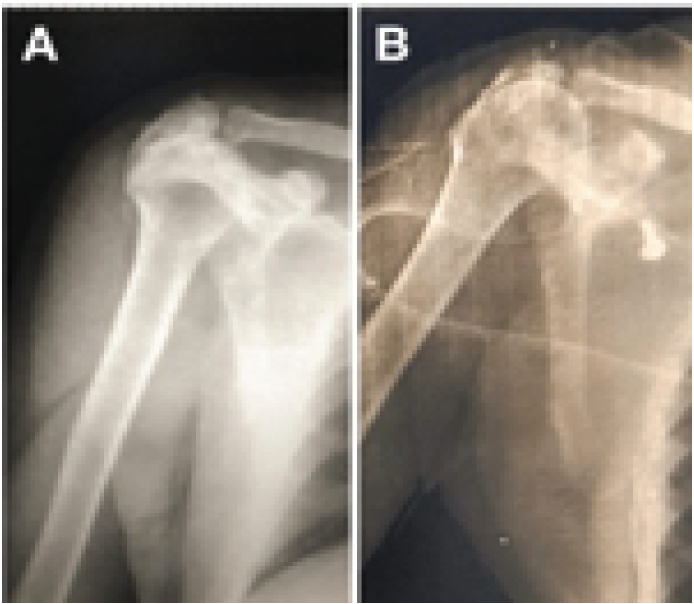
Figure 5: (a) Pre-operative and (b) Post-operative X-rays of a 45-year-old male with recurrent right shoulder instability following blunt trauma, showing the Latarjet procedure with single-screw fixation.
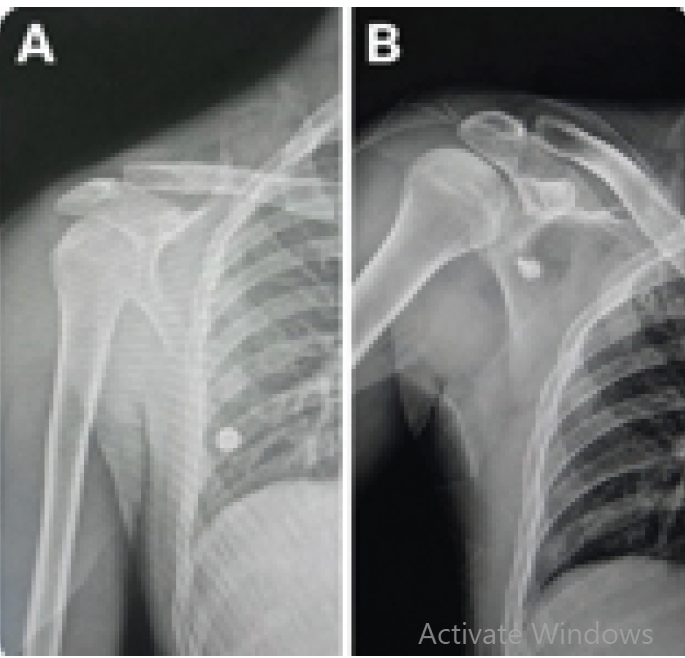
Figure 6: (a) Pre-operative and (b) Post-operative X-rays of a 25-year-old male with multiple episodes of right shoulder instability, showing the Latarjet procedure with single-screw fixation.

Figure 7: (a) Pre-operative and (b) Post-operative X-rays of a 28-year-old male gymnast with recurrent right anterior shoulder instability, showing the Latarjet procedure with two-screw fixation.
Figure 8: (a) Pre-operative and (b) Post-operative X-rays of a 30-year-old male with left shoulder instability, showing the Latarjet procedure with two-screw fixation.
Patient demographics:
The study included patients with recurrent anterior shoulder instability who underwent the Latarjet procedure and were allocated to Group A (single-screw fixation) or Group B (two-screw fixation). Both groups were comparable at baseline with no significant difference in age, sex distribution, duration of symptoms, or number of preoperative dislocations (Table 1).
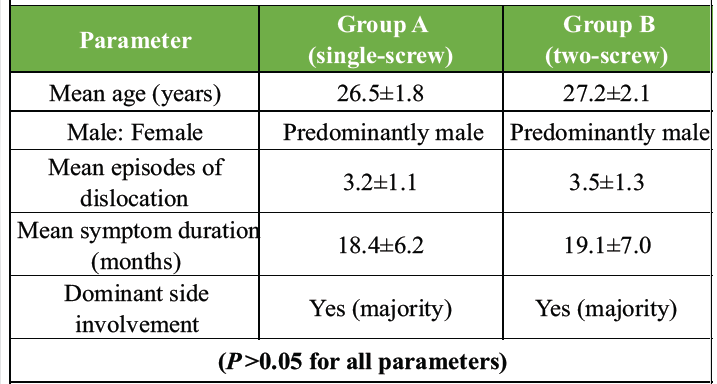
Table 1: Baseline demographic comparison between groups
Patient ages ranged from 25 to 30 years. The cohort was predominantly male. Presented cases included athletes (gymnastics, overhead throwing sports), patients with epilepsy-related instability, and those with recreational dislocation. All cases demonstrated Bankart lesions and Hill-Sachs defects on pre-operative MRI, with glenoid bone loss confirmed on CT.
Functional outcomes:
At final follow-up, both groups demonstrated significant improvement in functional outcomes compared to pre-operative status. The mean Constant-Murley score improved substantially in both groups, with no statistically significant difference between single-screw and two-screw fixation (Table 2). Range of motion also improved comparably in both groups, with patients achieving near-full forward flexion and abduction by 6–9 months.
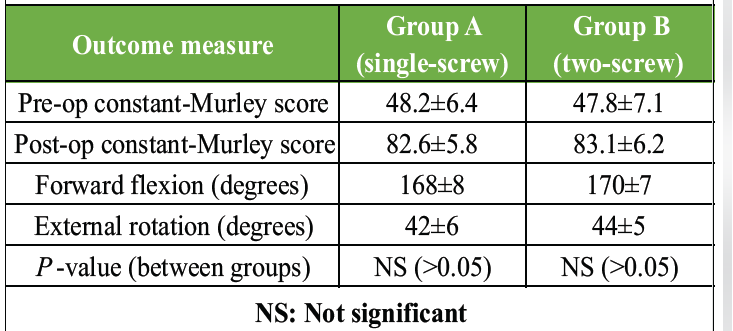
Table 2: Functional outcome comparison at final follow-up
Radiological outcomes:
Radiological evaluation at 3 months demonstrated high graft union rates in both groups. Graft positioning was assessed on post-operative X-rays and CT, confirming flush placement with the anterior glenoid rim and infero-anterior positioning below the glenoid equator in successfully stabilised cases. No cases of significant graft malposition were noted in the final cohort. Recurrence rates were low and comparable between groups.
Complications:
Overall complication rates were similar between groups. Hardware-related irritation was slightly more frequent in the two-screw group, while operative time was marginally shorter in the single-screw group. No cases of neurovascular injury, deep infection, or graft fracture were recorded. One case of early screw loosening was managed conservatively. No re-dislocation requiring revision surgery was recorded during the follow-up period (Table 3).
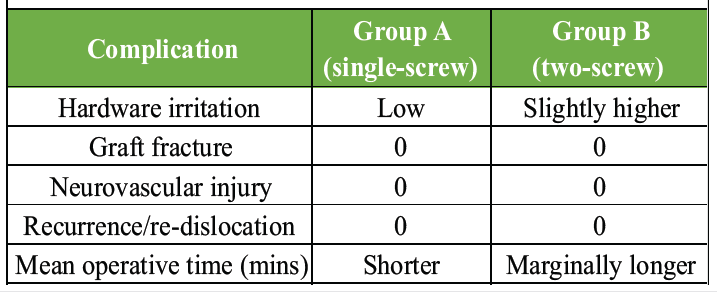
Table 3: Complication profile comparison between groups
The Latarjet procedure remains a gold standard for managing recurrent anterior shoulder instability with significant glenoid bone loss. Our comparative clinical study found no significant difference between single-screw and two-screw coracoid fixation in terms of functional outcome, graft union, recurrence, or complication rates, consistent with emerging evidence in the literature [6,7,11,12]. While biomechanical studies have traditionally supported two-screw fixation as providing superior rotational stability of the coracoid graft and better resistance to shear forces, these advantages do not appear to translate into measurable clinical superiority [4,8,13]. This discrepancy likely reflects the fact that early biological graft incorporation and accurate graft positioning — rather than immediate construct rigidity — are the primary determinants of clinical success. A key observation from our study was the overriding importance of accurate graft positioning. Placement of the coracoid graft flush with the anterior glenoid rim and below the glenoid equator (targeting the infero-anterior quadrant, 3–5 o’clock on the right shoulder) appeared to influence shoulder stability and functional recovery more significantly than the number of fixation screws. This is consistent with the computational biomechanical analysis by Martins et al. [5] and the finite element study by Ernstbrunner et al. [10], which demonstrated that malpositioned grafts — whether too medial or too lateral — adversely alter glenohumeral contact mechanics and predispose to early arthritic change. Single-screw fixation offers several practical advantages: Shorter operative time, reduced risk of graft fracture during drilling, lower implant cost, and technically simpler revision if required. These benefits may be particularly relevant in resource-limited settings and for smaller coracoid grafts where double drilling risks structural compromise [9]. Our findings support the 2023 ISAKOS Congress report (Catteeuw et al.) which demonstrated that open Latarjet with single-screw fixation achieves a high rate of graft fusion and represents a safe alternative to double-screw fixation. Two-screw fixation retains its theoretical advantages in specific scenarios – notably large graft constructs, osteoporotic bone, or situations where rotational control is judged critical intraoperatively. The 2024 biomechanical evaluation by Chang et al. in the journal of shoulder and elbow surgery confirmed that two-screw constructs provide reliable resistance to displacement under load, provided proper compression is achieved across the graft [4,13]. Hardware-related irritation and screw prominence secondary to coracoid graft osteolysis represent recognized complications, more frequent in the two-screw configuration; Ting et al. demonstrated that while osteolysis is radiologically common, it does not compromise clinical outcomes in the majority of patients [14]. The clinical cases presented in this series illustrate the diversity of patients undergoing the Latarjet procedure in a tertiary care government hospital in India – young athletes, patients with epilepsy, and manual workers – with uniformly good outcomes and no recurrences at minimum 3-month follow-up. These real-world outcomes further support the effectiveness of both fixation techniques when surgical technique is meticulous [15,16].
Both single-screw and two-screw fixation techniques in the Latarjet procedure provide comparable functional outcomes, graft union rates, and recurrence rates at early follow-up. The number of fixation screws does not significantly influence clinical outcome. Accurate coracoid graft positioning — flush with the anterior glenoid rim and below the glenoid equator — and meticulous surgical technique are more critical determinants of success than fixation configuration. Single-screw fixation represents a viable, technically simpler, and cost-effective alternative, particularly in cases with smaller coracoid grafts or in resource-limited settings.
In the Latarjet procedure, single-screw fixation is a safe and cost-effective alternative to two-screw fixation with comparable outcomes; accurate graft positioning remains the primary determinant of success regardless of fixation configuration.
References
- 1. Latarjet M. Treatment of recurrent dislocation of the shoulder. Lyon Chir 1954;49:994-7. [Google Scholar] [PubMed]
- 2. Walch G, Boileau P. Latarjet-Bristow procedure for recurrent anterior instability. Tech Shoulder Elbow Surg 2000;1:256-61. [Google Scholar] [PubMed]
- 3. Shinde GR, Patil SA, Naik N, Jagdale A. Outcome of Latarjet technique with low profile single 4.0 MM titanium screw and washer for recurrent dislocation of shoulder: A prospective study. J Med Sci Clin Res 2018;6:132-40. [Google Scholar] [PubMed]
- 4. Chang K, Covarrubias O, Scott D, Paller D, Green A. Latarjet procedure: Biomechanical evaluation of 2-screw coracoid fixation. J Shoulder Elbow Surg 2024;33:2236-42. [Google Scholar] [PubMed]
- 5. Martins R, Quental C, Folgado J, Angelo AC, Azevedo CD. Influence of graft positioning during the Latarjet procedure on shoulder stability and articular contact pressure: Computational analysis of the bone block effect. Biology (Basel) 2022;11:1783. [Google Scholar] [PubMed]
- 6. Omae H. CT image evaluation of one-screw fixation in the Latarjet procedure. Trauma Case Rep 2020;30:100372. [Google Scholar] [PubMed]
- 7. Landreau P, Catteeuw A, Cochard B, Cau J, Verborgt O. No Significant Difference in Radiological Outcomes at 3 Months Between Single-Screw and Two-Screw Fixation in Latarjet Surgery. Munich: ISAKOS Congress; 2025. [Google Scholar] [PubMed]
- 8. Catteeuw A, Landreau P. Open Latarjet Using One-Screw Fixation Achieves a High Rate of Graft Fusion. Boston: ISAKOS Biennial Congress; 2023. [Google Scholar] [PubMed]
- 9. Ghodadra N, Gupta A, Romeo AA, Bach BR Jr., Verma N, Shewman E, et al. Normalization of glenohumeral articular contact pressures after Latarjet or iliac crest bone-grafting. J Bone Joint Surg Am 2010;92:1478-89. [Google Scholar] [PubMed]
- 10. Ernstbrunner L, Robinson DL, Huang Y, Wieser K, Hoy G, Eugene EK[TPS3.1], et al. The influence of glenoid bone loss and graft positioning on graft and cartilage contact pressures after the Latarjet procedure. Am J Sports Med 2023;51:2454-64. [Google Scholar] [PubMed]
- 11. Maguire JA, Dhillon J, Sarna N, Keeter C, Scillia AJ, McCulloch PC, et al. Screw fixation for the Latarjet procedure may reduce risk of recurrent instability but increases reoperation rate compared to suture-button fixation: A systematic review. Arthroscopy 2024;40:1882-93.e1. [Google Scholar] [PubMed]
- 12. Thamrongskulsiri N, Limskul D, Tanpowpong T, Kuptniratsaikul S, Itthipanichpong T. Clinical outcomes, union rates, and complications of screw versus button fixation in the Bristow-Latarjet procedure for anterior shoulder instability: A systematic review and meta-analysis. Clin Orthop Surg 2023;15:1000-12. [Google Scholar] [PubMed]
- 13. Reeves JM, Athwal GS, Johnson JA. Double-screw and quadruple-button fixation for the glenoid: Latarjet versus bone block applications. JSES Int 2020;4:780-5. [Google Scholar] [PubMed]
- 14. Ting RS, Jang B, Murray N, Williams TG, Kang IL, Su Y, et al. An assessment of the clinical relevance of coracoid graft osteolysis following the Latarjet procedure: A clinical and radiological review. JSES Int 2024;8:719-23. [Google Scholar] [PubMed]
- 15. Ernstbrunner L, Pastor T, Waltenspul M, Gerber C, Wieser K. Salvage iliac crest bone grafting for a failed Latarjet procedure: Analysis of failed and successful procedures. Am J Sports Med 2021;49:3620-7. [Google Scholar] [PubMed]
- 16. Zeng Z, Liu C, Liu Y, Huang Y. Early outcomes of the arthroscopic Latarjet procedure in a series of 37 patients with shoulder instability. BMC Musculoskelet Disord 2021;22:845. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2026 Eden-Hybinette Procedure as Salvage Treatment for Failed Latarjet Surgery: A Case Report
April 1, 2026 Eden-Hybinette Procedure as Salvage Treatment for Failed Latarjet Surgery: A Case Report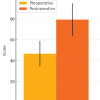 December 1, 2025 Mid-term Functional Outcomes of Open Congruent Arc Latarjet for Recurrent Anterior Shoulder Instability: A Retrospective Cohort Study
December 1, 2025 Mid-term Functional Outcomes of Open Congruent Arc Latarjet for Recurrent Anterior Shoulder Instability: A Retrospective Cohort Study July 1, 2026 Humeral Avulsion of Glenohumeral Ligament Lesion – A Case Report and Surgical Considerations
July 1, 2026 Humeral Avulsion of Glenohumeral Ligament Lesion – A Case Report and Surgical Considerations July 1, 2025 Late Presentation of Acromioclavicular Joint Dislocation with Double Fracture of Coracoid Process Managed by Arthroscopic Stabilization Technique: A Case Report
July 1, 2025 Late Presentation of Acromioclavicular Joint Dislocation with Double Fracture of Coracoid Process Managed by Arthroscopic Stabilization Technique: A Case Report