
A novel probe test efficiently selects the optimal diameter of biodegradable interference screws for ACL reconstruction, significantly reducing screw-related complications and the need for additional cortical fixation.
Dr. Naveen Jeyaraman, Department of Orthopaedics, ACS Medical College and Hospital, Dr MGR Educational and Research Institute, Chennai, Tamil Nadu, India. E-mail: naveenjeyaraman@yahoo.com
Abstract
Introduction: Anterior cruciate ligament (ACL) reconstruction is a common orthopedic procedure, employing various grafts such as the hamstring tendon, bone-patellar bone, and quadriceps tendon. Fixation methods include suspensory loop with button, interferential screw, and cortical fixation. The optimal screw diameter for tibial tunnel fixation remains undefined, with choices ranging from 1mm smaller to 1–2 mm larger than the tunnel diameter. Screw-related complications such as breakage and thread flattening are concerns. This study was to determine the ideal screw diameter for secure graft fixation in the tibial tunnel during ACL reconstruction.
Materials and Methods: A novel arthroscopic probe technique was utilized to assess tibial tunnel bone integrity. Bone quality was categorized into weak, strong, and very strong. Screw size selection, either equal to or 1–2 mm larger than the tunnel diameter, was based on bone quality. Screw lengths varied from 25 mm to 35 mm.
Results: The novel technique significantly reduced screw-related complications, from 9.6% (24 out of 248 patients) to 0.5% (1 out of 187 patients). The need for additional cortical stabilization decreased from 14.5% (36 out of 248 patients) to 1.6% (3 out of 187 patients).
Conclusion: The low-cost, efficient 2-min probe test is a secure and effective method for selecting interferential screws in ACL reconstruction, minimizing complications, and additional stabilization needs.
Keywords: Anterior cruciate ligament, biodegradable screw, tibial tunnel, graft fixation.
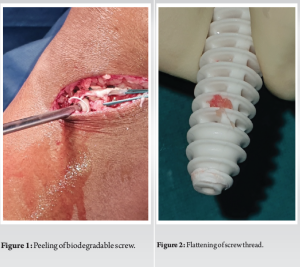
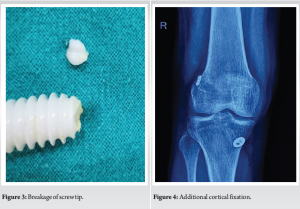
Anterior cruciate ligament (ACL) reconstruction, a surgical procedure performed worldwide, is considered a standard practice in arthroscopy. The technique involves affixing a graft to the femur and tibia to replace the original, injured ACL. Various methods are employed to secure the graft to these bones, including suspensory fixation, aperture fixation, cortical fixation, and additional fixation. The most commonly used method for femoral fixation is the implementation of a suspensory device, while an interferential screw is typically utilized for tibial fixation [1]. On the tibial side interference screw fixation is one of the stronger modes of ligament fixation [2-5]. Both metallic and biodegradable screws are in use for decades. Bio-screw has claimed many advantages over the metallic screw in terms of less graft laceration, low-stress shielding, no second surgery for screw removal, low distortion during magnetic resonance imaging, and well bone stock for revision surgery. Still, it is not free from disadvantages, most commonly accounting for its higher cost, lower mechanical strength, tunnel widening, and abnormal biological response [6,7]. The determination of the bio-screw’s dimensions for securing the graft within the tibial tunnel is primarily influenced by the size of the graft, the length of the tunnel, and its diameter [8,9]. The diameter of the screw may be diminished by 1 mm in relation to the diameter of the tunnel, equal to the diameter of the tunnel, or increased by 1–2 mm as compared to the tunnel diameter. On occasion, the tendon is harmed and even torn during the insertion of the screw into the tibial tunnel [10,11]. The graft injury is less with smaller-sized screws but there is a higher possibility of loosening of graft leading to post-operative laxity. In turn, when a larger diameter screw is used, it leads to graft damage and laceration during screwing [11,12]. The tendon undergoes compression and occasional incision when an unsuitable screw is inserted, resulting in a decline in the pullout strength [11]. The estimation of the strength of interference screw fixation in ACL reconstruction should not be based on the utilization of insertion torque [13,14]. Many studies showed that during ACL reconstruction, the tibial bio-screw is 1 mm more than the tunnel diameter [9,15]. Campbell’s 12th edition: Use a 1 mm smaller screw with the use of cortical post for graft fixation into the tibial tunnel. We performed 248 (male: 209 and female: 39) ACL reconstructions from 2009 to 2015. In all cases, we used a cortical suspensory button for femoral fixation and an interferential bio-screw for tibial fixation. The usual screw was of length 25 mm to 35 mm and diameter 1 mm more than the tunnel diameter based on the literature. We used semitendinosus and gracilis autograft. For us, hearing the torque sound while screwing justifies the appropriate fixation of the graft. In 38 cases (15%), we were not able to hear the torque sound while screwing the screw and presumed an inferior fixation as the feeling of fixation of the graft was not well appreciated. Because of the cost factor screw was changed to a 1 mm higher diameter only in 2 cases but additional cortical fixation such as a suture wheel, bone stapler, or suture post was used in the rest 36 more economical cases. In contrast, there were 24 cases (all male) where we could not screw the interferential screw in one attempt. Of these 24 cases, screw tip was broken in 4 cases, excoriated in 6 cases, and flattening of screw threads in 14 cases (Fig. 1, 2, 3). We presume that the screw size diameter of 1 mm more than the tunnel diameter does not hold for all patients. In some patients, the screw is either too tight to insert or too loose to fix the graft. Whenever the screw is loose, we need to fix it with additional cortical fixation, this accounts for extra cost and the possibility of tissue reaction to non-absorbable sutures (Fig. 4). When there is difficulty in inserting the screw, we need to dilate the tunnel, which in some situations widens the tunnel more than desired. As there is no standard guideline for the selection of a screw for the fixation of the graft into the tunnel, there is the possibility of an undesirable situation in the theater. Besides we have not considered the factors influencing the selection of screw size like bone quality, swelling of graft, etc, we presume that bone quality of the proximal tibia could be a major factor in deciding the screw diameter. Bone quality is decided by various factors such as age, gender, and physical activity of the individual. We can access the bone quality of the proximal tibia by X-ray or dual-energy X-ray absorptiometry (DEXA), but not helpful because of different exposure of X-ray beam and opacity modulation by the digital X-rays. The role of DEXA in this particular scenario is not well known, but as orthopedic surgeons, we are well versed in accessing the quality of bone to some extent from the difficulty in drilling the bone. Hence, the bone quality of the proximal tibia can be also felt while drilling the tibial tunnel. As we know drilling is also affected by various factors such as the torque of the drill, sharpness of the drill bit, battery power of the drill, etc, we thought of considering this feeling and accessing the bone quality of the tibial tunnel with an arthroscopic probe, the probe test.
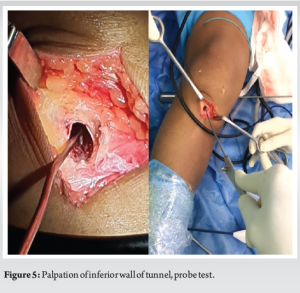
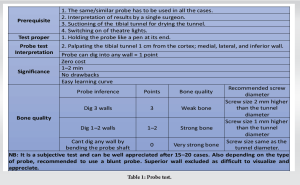
Probe test: Evaluating the bone quality of the tibial tunnel with the arthroscopic probe and classifying bone quality into three groups. Based on bone quality, ideal screw size is decided (Table 1, Fig. 5, and Video 1). The purpose of this study is to present a series of ACL reconstructions with bio-screws whose size is decided based on bone quality accessed by novel probe tests. We hypothesize that the bone quality of the proximal tibia could be influencing the fixation of the graft with an interferential screw. Our probe test does not add any additional cost and can be executed in <2 min, which could help in accessing the bone quality and selection of ideal screw size for graft fixation in the tibial tunnel.
We have included ACL reconstruction surgeries performed between January 2016 and May 2019. All revision ACL reconstructions and tibial fixation other than biodegradable screws were not included in the study. Graft fixation with metallic screw was excluded from the study. After all exclusion, a total of 187 patients (male 140 and female 47) in whom probe test was employed for the selection of interferential screw were included in the study. All the patients were in the age group of 21 years–56 years (Ave 36 years). Hamstring tendons either semitendinosus alone or with gracilis harvested in all the patients to prepare the graft to achieve at least 7-mm graft diameter.
The routine surgical procedure was employed in all patients with appropriate anesthesia. The anatomical femoral tunnel was prepared with a transportal approach. The anatomical tibial tunnel was created routinely and the diameter of the tunnel was decided as per the diameter of the graft. The bone quality of the tibial tunnel was accessed as per our probe test (Table 1 and Fig. 5). Quadrupled or 5-stranded graft fixed to femoral cortex with suspensory loop and button. The knee was put into 20 cycles of movement with tension on the graft. The length of the screw was decided as per the length of the tibial tunnel usually between 25 mm and 35 mm. The diameter of the tibial screw is decided as per the probe test outcome. A tibial screw was inserted from the posteromedial aspect of the graft with a posterior thrust on the tibia at 30° of knee flexion. All the screws were applied by a single surgeon and torque sound was appreciated where ever it was audible (Video 2).
It was part of routine ACL reconstruction but additional cortical fixation such as a suture wheel, post, and bone stapler along with screws of all sizes was kept ready to meet any additional need where the torque sound was not audible (Video 3). The significance of probe test is zero cost in terms of financial expenditure, less time consuming to perform (1–2 min), no drawbacks, and easy learning curve.
From the probe test, we had very strong bone in 25 (13%) cases, strong bone in 118 (63%) cases, and weak in 44 (23%) cases. Bio-screw of diameter same size as tunnel width was given in 25 cases, 1 mm more than tunnel width in 117, and 2 mm more than tunnel width in 45 cases (one case screw revised to higher screw) (Table 2).
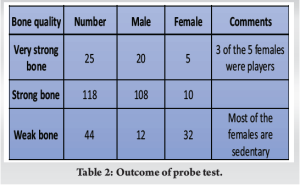
Graft fixation on the tibial tunnel is considered satisfactory when we can hear the torque sounds while screwing the screw. As per our definition of satisfactory fixation, we achieved so in 182 patients (97.3%). There was no additional cortical fixation in all the above 182 cases. In 4 cases, all females were not satisfied with our fixation, as there was no torque sound heard during screwing nor we were happy from the feel of screwing the screw. Of the 4 patients, in one case, the next higher diameter screw was used and in three patients, additional cortical fixation was used. With the use of next higher diameter, screw fixation was satisfactory. In one case (probe score = 0), we struggled to insert the screw and ended up with a breakage of the screw tip. We further dilated the cortical margin of the tibial tunnel and reused the same screw. The fate of interferential screws with and without probe test has been tabulated in Table 3.
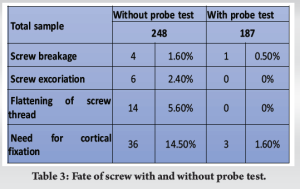
It is imperative to ensure complete immobilization of the ACL graft within the tibial tunnel to effectively mitigate any potential loosening of the graft following the surgical procedure. From the femoral aspect if the suspensory button is placed correctly on the cortex, further loosening of the graft depends on the quality of the suspensory loop. From the tibial aspect whenever the surgeon is not confident of his graft fixation, there is invocation of additional cortical fixation to prevent graft slippage with the rehabilitation of the knee. There are multiple opinions in the literature on the selection of screw diameter for fixation of ACL graft into the tibial tunnel. Harvey et al. [1] found that the pull-out strength of the interference screw depends upon the length of the screw but the correlation was not significant. They found better fixation of graft when the head of the screw engages the cortex of the tibia. Increasing the length of the screw in the cancellous bone did not improve graft fixation [1]. We would like to appreciate that the torque sound is produced during the engagement of the screw in the cortical part of the tibial tunnel. For the same reason, we evaluated the bone quality only on the cortical part of the tibia, i.e., within 1 cm of the tunnel from the tibial cortex. Similarly, Phillips et al. [16] found a difference in the insertion torque at different depths of the tibial tunnel. The average torque values for the insertion in the distal third, middle third, and proximal third were recorded as 8.7, 4.7, and 4.3 in/lb, respectively. The highest torque was observed at the cortical region of the tibial tunnel. Debieux et al. [17] found no difference in the functional outcome of the knee in regard to interferential screw, i.e., biodegradable screw and metallic screw. They observed breakage of the biodegradable screw during the insertion of the screw in the tibial tunnel. We presume that this could be due to very strong bone and the use of a standard 1 mm or 2 mm larger diameter screw for fixation of graft in the tibial tunnel. In our previous observation before advocating the probe test, we had a problem with 24 cases in which the screw tip was broken in 4 cases, screw excoriation in 6 cases, and flattening of screw thread in 14 cases. Such an outcome could be due to swelling of graft or very strong bone. With the implementation of the probe test, our issues with screw breakage decreased from 1.6% (4 of 248) to 0.5% (1 of 187) and all possible screw damage decreased from 9.6% (24 of 248) to 0.5% (1 of 187). We used biodegradable screws in all the cases and cannot opine the effect of metallic screws in similar situations. Emond et al. [18] in their study on 745 patients comparing bio-screws with metallic screws observed similar complications in both groups and no difference in functional outcome and laxity of graft tested by arthrometry. Brand et al. [9] in their cadaveric study found better fixation of graft in tibial tunnel in bone with good bone mineral density. Besides the pull-out strength was directly related to the torque of the application of the screw, higher torque of application, better fixation of graft, and less graft slippage. They have postulated the role of torque in the application of screws and post-operative rehabilitation. In our study, we lack a torque-limiting screwdriver and for us, the torque sound during screw application was considered a satisfactory fixation. As an orthopedician, we are well versed with the bone quality and difficulty in screw fixation. In tibial screw fixation, we could well correlate the difficulty in screw fixation and the production of torque sound. Although we have less literature support on torque sound for us, it is the marker of satisfactory fixation of the graft. There was no addition of extra cortical fixation when screw insertion produced torque sound. Weiler et al. [8] showed that screw length is more important than screw diameter for fixation strength. More screw length gives more hamstring tendon interference fit fixation. Heier et al. [19] commented on the outcome of ACL reconstruction which depends more on the biological age than the chronological age of the patient. Basically, he is pointing at the quality of bone and muscle quality influencing the outcome of ACL reconstruction. We had a similar experience on female patients where the chronological age did not correspond to their biological age in terms of their bone quality. In these patients, we had to change to 1 mm higher screw diameter or added cortical fixation. Age of the patient is not sufficient to assess the bone quality, and there should be real-time feedback during the operation to evaluate the bone quality. Both difficulty in drilling and access of bone quality by probe test can give an idea about the bone quality. Difficulty in drilling can be biased by the sharpness of drill bit, drill rpm (rotation per minute), power of drill, etc. However, probe test is simple and easy to access, which can be well appreciated in 15–20 cases. Besides it is no way hindering the outcome of surgery, it takes only 2 min to do the test and part of routine surgical procedure. Whenever there is doubt about fixation, an additional cortical fixation can be used. In our series, the need for additional cortical fixation before the use of probe test was 36 cases out of 248 (14%) patients and only in 3 of 187 patients (1.6%). The rate of screw damage or breakage before the advent of probe test was 9.6% (24 of 248 patients) and it was only 0.5% (1 of 187 patients) after we used the probe test for the selection of interferential screws. Probe test was never detrimental in any way either from time-consuming or in terms of the selection of screw. Careful graft preparation, accurate measurement of graft diameter, and preparing matched tunnel account for graft stability and withstanding the load during post-operative rehabilitation till there is bony ingrowth into the graft [4]. Dual photon absorptiometry can be used to measure the bone quality of proximal tibia which is a non-invasive and in vivo procedure. However, access to high-end equipment is a matter of concern and the costs involved outweigh the benefits. Probe test as per our perspective can meet the need of the hour in accessing the bone quality about the selection of interferential screw at no additional cost [20]. The present study warrants careful consideration of its inherent limitations. First, it is crucial to recognize the lack of specificity associated with the probe test utilized in our research. The variability in the applied force during this test across different surgeons presents a notable challenge in achieving standardization. Furthermore, the reliance on torque sound, as suggested by the author, poses an additional limitation, given its inherent inability to be quantitatively measured.
At present, there exists a lack of a parameter that can aid the surgeon in the selection of the appropriate screw diameter for the fixation of the ACL graft in the tibial tunnel. The probe test, which is both cost-effective and safe, can be completed within a span of 2 min. The test has been successfully employed in 15–20 cases, and its underlying principles are not overly complex. We propose advocating for the use of this test until a superior method for selecting the optimal screw diameter for ACL graft fixation in the tibial tunnel becomes available. Further research endeavors have the potential to reinforce the validity of this test.
The use of a simple, cost-effective probe test to assess tibial tunnel bone quality can guide the selection of the optimal diameter for biodegradable interference screws, leading to a significant reduction in screw-related complications and the need for additional fixation in ACL reconstruction.
References
- 1.Harvey AR, Thomas NP, Amis AA. The effect of screw length and position on fixation of four-stranded hamstring grafts for anterior cruciate ligament reconstruction. Knee 2003;10:97-102. [Google Scholar | PubMed]
- 2.Zeng C, Lei G, Gao S, Luo W. Methods and devices for graft fixation in anterior cruciate ligament reconstruction. Cochrane Database Syst Rev 2018;2018:CD010730. [Google Scholar | PubMed]
- 3.Kurosaka M, Yoshiya S, Andrish JT. A biomechanical comparison of different surgical techniques of graft fixation in anterior cruciate ligament reconstruction. Am J Sports Med 1987;15:225-9. [Google Scholar | PubMed]
- 4.Caborn DN, Coen M, Neef R, Hamilton D, Nyland J, Johnson DL. Quadrupled semitendinosus-gracilis autograft fixation in the femoral tunnel: A comparison between a metal and a bioabsorbable interference screw. Arthroscopy 1998;14:241-5. [Google Scholar | PubMed]
- 5.Brown CH, Wilson DR, Hecker AT, Ferragamo M. Graft-bone motion and tensile properties of hamstring and patellar tendon anterior cruciate ligament femoral graft fixation under cyclic loading. Arthroscopy 2004;20:922-35. [Google Scholar | PubMed]
- 6.Ambrose CG, Clanton TO. Bioabsorbable implants: Review of clinical experience in orthopedic surgery. Ann Biomed Eng 2004;32:171-7. [Google Scholar | PubMed]
- 7.Südkamp NP, Kääb MJ. Biodegradable implants in soft tissue refixation: Experimental evaluation, clinical experience, and future needs. Injury 2002;33 (Suppl 2):B17-24. [Google Scholar | PubMed]
- 8.Weiler A, Hoffmann RF, Siepe CJ, Kolbeck SF, Südkamp NP. The influence of screw geometry on hamstring tendon interference fit fixation. Am J Sports Med 2000;28:356-9. [Google Scholar | PubMed]
- 9.Brand JC, Pienkowski D, Steenlage E, Hamilton D, Johnson DL, Caborn DN. Interference screw fixation strength of a quadrupled hamstring tendon graft is directly related to bone mineral density and insertion torque. Am J Sports Med 2000;28:705-10. [Google Scholar | PubMed]
- 10.Spindler KP, Kuhn JE, Freedman KB, Matthews CE, Dittus RS, Harrell FE. Anterior cruciate ligament reconstruction autograft choice: Bone-tendon-bone versus hamstring: Does it really matter? A systematic review. Am J Sports Med 2004;32:1986-95. [Google Scholar | PubMed]
- 11.Becker R, Voigt D, Stärke C, Heymann M, Wilson GA, Nebelung W. Biomechanical properties of quadruple tendon and patellar tendon femoral fixation techniques. Knee Surg Sports Traumatol Arthrosc 2001;9:337-42. [Google Scholar | PubMed]
- 12.Espejo-Baena A, Ezquerro F, de la Blanca AP, Serrano-Fernandez J, Nadal F, Montañez-Heredia E. Comparison of initial mechanical properties of 4 hamstring graft femoral fixation systems using nonpermanent hardware for anterior cruciate ligament reconstruction: An in vitro animal study. Arthroscopy 2006;22:433-40. [Google Scholar | PubMed]
- 13.Eichinger M, Ploner M, Degenhart G, Rudisch A, Smekal V, Attal R, et al. Tunnel widening after ACL reconstruction with different fixation techniques: Aperture fixation with biodegradable interference screws versus all-inside technique with suspensory cortical buttons. 5-year data from a prospective randomized trial. Arch Orthop Trauma Surg 2023;143:6707-18. [Google Scholar | PubMed]
- 14.Järvinen TL, Nurmi JT, Sievänen H. Bone density and insertion torque as predictors of anterior cruciate ligament graft fixation strength. Am J Sports Med 2004;32:1421-9. [Google Scholar | PubMed]
- 15.Pereira VL, Medeiros JV, Nunes GR, de Oliveira GT, Nicolini AP. Tibial-graft fixation methods on anterior cruciate ligament reconstructions: A literature review. Knee Surg Relat Res 2021;33:7. [Google Scholar | PubMed]
- 16.Phillips BB, Cain EL, Dlabach JA, Azar FM. Correlation of interference screw insertion torque with depth of placement in the tibial tunnel using a quadrupled semitendinosus-gracilis graft in anterior cruciate ligament reconstruction. Arthroscopy 2004;20:1026-9. [Google Scholar | PubMed]
- 17.Debieux P, Franciozi CE, Lenza M, Tamaoki MJ, Magnussen RA, Faloppa F, et al. Bioabsorbable versus metallic interference screws for graft fixation in anterior cruciate ligament reconstruction. Cochrane Database Syst Rev 2016;7:CD009772. [Google Scholar | PubMed]
- 18.Emond CE, Woelber EB, Kurd SK, Ciccotti MG, Cohen SB. A comparison of the results of anterior cruciate ligament reconstruction using bioabsorbable versus metal interference screws: A meta-analysis. J Bone Joint Surg Am 2011;93:572-80. [Google Scholar | PubMed]
- 19.Heier KA, Mack DR, Moseley JB, Paine R, Bocell JR. An analysis of anterior cruciate ligament reconstruction in middle-aged patients. Am J Sports Med 1997;25:527-32. [Google Scholar | PubMed]
- 20.Madsen OR, Schaadt O, Bliddal H, Egsmose C, Sylvest J. Bone mineral distribution of the proximal tibia in gonarthrosis assessed in vivo by photon absorption. Osteoarthritis Cartilage 1994;2:141-7. [Google Scholar | PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study
June 1, 2026 Functional Outcomes of Arthroscopic Anterior Cruciate Ligament Reconstruction Using Hamstring Tendon Autograft in a Predominantly Chronic Anterior Cruciate Ligament Injury Cohort: A Prospective Study June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide
June 1, 2026 Artelon Graft Augmentation in Revision Anterior Cruciate Ligament Reconstruction: Surgical Technique Guide May 1, 2026 All-Inside Anterior Cruciate Ligament Reconstruction: A Minimally Invasive Bone Preserving Approach with Promising Functional Outcomes
May 1, 2026 All-Inside Anterior Cruciate Ligament Reconstruction: A Minimally Invasive Bone Preserving Approach with Promising Functional Outcomes May 1, 2026 Anterior Cruciate Ligament Reconstruction Using Tibial Attachment – Preserving Hamstring Grafts: Early Clinical and Magnetic Resonance Imaging Assessment of Graft Ligamentization
May 1, 2026 Anterior Cruciate Ligament Reconstruction Using Tibial Attachment – Preserving Hamstring Grafts: Early Clinical and Magnetic Resonance Imaging Assessment of Graft Ligamentization