
MIPO provides comparable fracture union with superior perioperative outcomes and reduced biological insult compared to conventional plating.
Dr. Mulayam Singh Yadav, Department of Orthopaedics, Government Medical College, Satna, Madhya Pradesh, India. E-mail: myadav.yadav33@gmail.com
Abstract
Introduction: Minimally invasive plate osteosynthesis (MIPO) has been increasingly adopted as an alternative to conventional open reduction and internal fixation due to its potential to preserve soft-tissue integrity and enhance fracture healing. This study aimed to compare surgical outcomes and perioperative laboratory parameters between MIPO and conventional plating.
Materials and Methods: A prospective comparative study was conducted on 60 patients with long bone fractures, divided equally into MIPO (n = 30) and conventional plating (n = 30) groups. Intraoperative parameters, perioperative laboratory values (hemoglobin [Hb], total leukocyte count [TLC], C-reactive protein [CRP], and serum creatinine), and post-operative outcomes, including time to union and complications, were evaluated. Statistical analysis was performed using appropriate tests, with P < 0.05 considered significant.
Results: Baseline characteristics were comparable between groups. The MIPO group demonstrated significantly shorter operative duration (72.5 ± 14.3 vs. 89.6 ± 16.8 min), reduced blood loss (118.4 ± 36.7 vs. 245.2 ± 52.1 mL), lower transfusion requirement (10.0% vs. 33.3%), and shorter hospital stay (6.2 ± 1.5 vs. 9.1 ± 2.3 days) (P < 0.05). Post-operative Hb levels were significantly higher, while TLC and CRP levels were significantly lower in the MIPO group on days 1 and 3 (P < 0.001). Mean time to union was shorter in the MIPO group (14.8 ± 2.6 vs. 17.2 ± 3.1 weeks, P = 0.002). Union rates and complication rates were comparable between groups (P > 0.05).
Conclusion: MIPO offers superior perioperative outcomes and reduced inflammatory response with comparable union rates and complications, making it an effective alternative to conventional plating.
Keywords: Minimally invasive plate osteosynthesis, conventional plating, fracture fixation, perioperative parameters, fracture union.
Fractures of long bones are among the most common injuries encountered in orthopaedic practice and frequently require surgical stabilisation to restore alignment, facilitate early mobilisation, and optimise functional outcomes [1]. Open reduction and internal fixation (ORIF) using plate osteosynthesis has traditionally been considered the standard operative technique; however, it is associated with extensive soft-tissue dissection, periosteal stripping, and disruption of fracture biology, which may contribute to complications such as infection, delayed union, and non-union [2,3]. In recent years, the concept of biological fixation has gained prominence, emphasising preservation of the fracture environment and soft-tissue integrity. Minimally invasive plate osteosynthesis (MIPO) has emerged as an important technique aligned with these principles, utilising indirect reduction and limited surgical exposure to minimise vascular compromise at the fracture site [3,4]. The development of locking compression plates and improved instrumentation has further facilitated the widespread adoption of MIPO in the management of long bone fractures [4]. Several comparative studies and meta-analyses have evaluated the outcomes of MIPO versus conventional plating techniques. Evidence suggests that MIPO is associated with reduced intraoperative blood loss, shorter operative duration, and lower rates of complications such as infection and iatrogenic nerve injury, while maintaining comparable or improved fracture union rates [1,5]. In addition, MIPO has been shown to result in faster fracture healing and reduced post-operative pain due to minimal soft-tissue disruption [5,6]. Despite these advantages, concerns remain regarding technical complexity, radiation exposure, and potential for malreduction. Although multiple studies have compared these techniques in specific fracture types, there remains variability in reported outcomes, particularly with respect to perioperative physiological response and laboratory parameters. Therefore, the present study was undertaken to compare surgical outcomes and perioperative laboratory parameters between MIPO and conventional plating, with the aim of providing a comprehensive evaluation of their clinical effectiveness.
Study design and setting:
This was a prospective, comparative, observational study conducted in a tertiary care teaching hospital. The study aimed to compare surgical outcomes and perioperative laboratory parameters in patients undergoing MIPO versus conventional ORIF.
Ethical considerations:
Ethical considerations were strictly adhered to throughout the study. Approval was obtained from the Institutional Ethics Committee before commencement (IEC/GMC/155; dated February 22, 2024). Written informed consent was secured from all participants before enrollment. The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki.
Sample size estimation:
Sample size was determined based on previously published comparative studies evaluating MIPO and conventional plating, where individual study sample sizes ranged from approximately 30 to 70 patients [1,7,8]. Assuming a moderate effect size in perioperative blood loss and operative duration, a confidence level of 95%, and a power of 80%, the calculated minimum sample size was 54 patients. To account for possible attrition, a total of 60 patients were included and divided equally into two groups. Group A: MIPO (n = 30) and Group B: ORIF (n = 30)
Study population:
Patients presenting with diaphyseal fractures of long bones (e.g., humerus, tibia, or femur) requiring surgical fixation were screened for eligibility.
Inclusion criteria:
- Age 18 years
- Closed fractures or Gustilo-Anderson type I fractures
- Patients fit for surgery under anesthesia
- Patients providing informed written consent
Exclusion criteria:
- Pathological fractures
- Open fractures, types II and III
- Polytrauma patients with life-threatening injuries
- Previous surgery at the fracture site
- Patients with severe systemic illness (e.g., uncontrolled diabetes and renal failure).
Grouping and intervention:
Patients were allocated into two groups based on the surgical technique used:
- Group A (MIPO): Fractures were treated using MIPO, involving indirect fracture reduction and percutaneous plate insertion with minimal soft-tissue dissection.
- Group B (Conventional plating): Patients underwent ORIF using standard plating techniques with direct visualisation of the fracture site.
Both procedures were performed by experienced orthopaedic surgeons using standard operative protocols.
Perioperative parameters assessed:
Duration of surgery (min), Intraoperative blood loss (mL), Need for blood transfusion, and Length of hospital stay (days) were recorded.
Laboratory parameters:
Blood samples were collected preoperatively and on postoperative days 1 and 3 to assess haemoglobin (Hb), total leukocyte count (TLC), C-reactive protein (CRP), and serum creatinine. These parameters were selected to evaluate perioperative physiological stress and inflammatory response [1].
Outcome measures:
Primary outcomes:
- Fracture union (clinically and radiologically assessed)
- Time to union (weeks).
Secondary outcomes:
- Post-operative complications (infection, non-union, implant failure)
- Functional outcome using standardised scoring systems (e.g., DASH or equivalent depending on bone involved).
Previous literature indicates that union rate, complication profile, and functional scores are key endpoints in such comparisons [1].
Follow-up:
Patients were followed up at 6 weeks, 3 months, and 6 months postoperatively. Clinical and radiological assessments were performed at each visit.
Statistical analysis:
Statistical analysis was performed using the Statistical Package for the Social Sciences version 25.0 after initial data entry in Microsoft Excel. Continuous variables were summarised as mean with standard deviation, whereas categorical variables were presented as proportions and percentages. Comparison of means between the two groups was carried out using the independent t-test, while categorical variables were analysed using the Chi-square test. A P < 0.05 was considered indicative of statistical significance.
A total of 60 patients were included in the study, with 30 patients in each group. The baseline demographic and clinical characteristics were comparable between the two groups, with no statistically significant differences observed in terms of age, gender distribution, mode of injury, bone involved, or fracture type (P > 0.05) (Table 1).
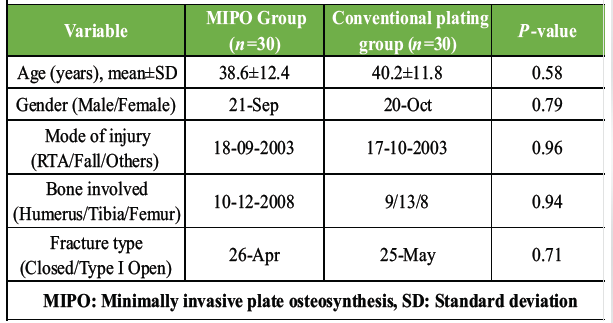
Table 1: Baseline demographic and clinical characteristics of study participants
Intraoperative and perioperative parameters demonstrated significant differences between the groups. The mean duration of surgery was significantly lower in the MIPO group compared to the conventional plating group (72.5 ± 14.3 min vs. 89.6 ± 16.8 min, P < 0.001). Similarly, intraoperative blood loss was markedly reduced in the MIPO group (118.4 ± 36.7 mL) compared to the conventional group (245.2 ± 52.1 mL), which was statistically significant (P < 0.001). The requirement for blood transfusion was also significantly lower in the MIPO group (3 patients) as compared to the conventional group (10 patients) (P = 0.03). Furthermore, the mean duration of hospital stay was significantly shorter in patients treated with MIPO (6.2 ± 1.5 days) compared to those undergoing conventional plating (9.1 ± 2.3 days) (P < 0.001) (Table 2).
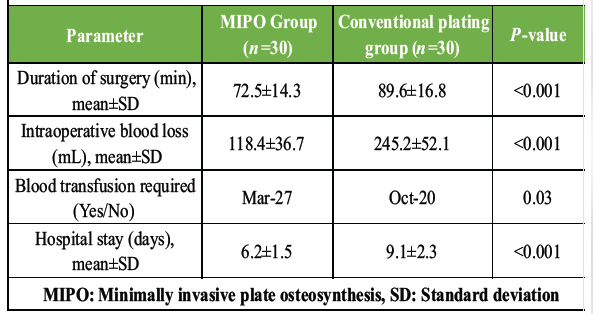
Table 2: Comparison of intraoperative and perioperative parameters
With respect to perioperative laboratory parameters, no significant differences were observed in pre-operative Hb, TLC, CRP, or serum creatinine levels between the two groups (P > 0.05). However, post-operative changes showed significant variations. On post-operative day 1, Hb levels were significantly higher in the MIPO group (11.6 ± 1.1 g/dL) compared to the conventional group (10.2 ± 1.4 g/dL) (P < 0.001), and this difference persisted on day 3 (P < 0.001). TLC and CRP levels were significantly elevated in the conventional plating group on post-operative days 1 and 3, indicating a higher inflammatory response compared to the MIPO group (P < 0.001). Serum creatinine levels did not differ significantly between the groups postoperatively (P > 0.05) (Table 3).
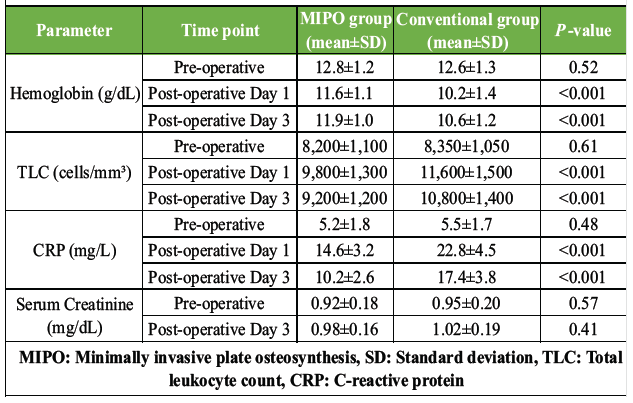
Table 3: Comparison of perioperative laboratory parameters
Post-operative outcomes (Fig. 1) revealed that the mean time to fracture union was significantly shorter in the MIPO group (14.8 ± 2.6 weeks) compared to the conventional plating group (17.2 ± 3.1 weeks) (P = 0.002).
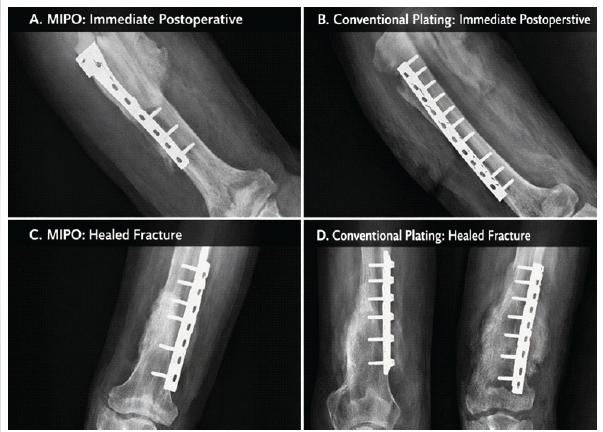
Figure 1: Radiographs of clinical cases comparing the two methods.
Although the union rate was higher in the MIPO group (96.7%) than in the conventional group (90.0%), this difference was not statistically significant (P = 0.30). The incidence of post-operative infection was lower in the MIPO group (1 patient) compared to the conventional group (5 patients), though this did not reach statistical significance (P = 0.08). Similarly, rates of non-union and implant failure were lower in the MIPO group, but the differences were not statistically significant (P > 0.05). Functional outcomes were better in the MIPO group, with a higher proportion of patients achieving good outcomes; however, the difference was not statistically significant (P = 0.18) (Table 4).
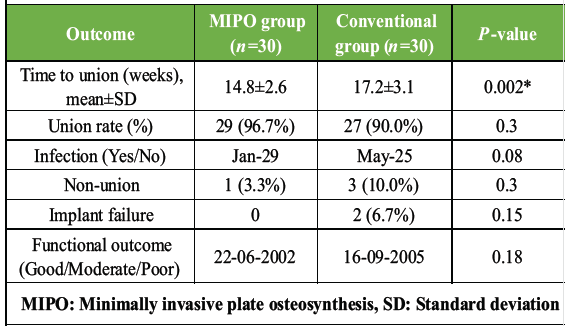
Table 4: Post-operative outcomes and complications
The present study demonstrates that MIPO offers significant perioperative advantages over conventional plating, particularly in terms of reduced operative time, blood loss, and hospital stay. These findings are consistent with multiple recent studies reporting that MIPO minimises surgical trauma due to limited soft-tissue dissection, thereby improving perioperative outcomes [9,10]. A recent retrospective cohort study also observed reduced operative duration, lower blood loss, and decreased post-operative pain in patients treated with MIPO compared to conventional techniques [9]. The significantly lower intraoperative blood loss and better preservation of post-operative Hb levels observed in this study can be attributed to the biological fixation principles of MIPO. Similar findings have been reported in prospective comparative studies, where MIPO demonstrated a statistically significant reduction in intraoperative blood loss compared to ORIF [10]. Meta-analytical evidence further supports that MIPO is associated with less intraoperative blood loss and shorter operative duration, reinforcing its minimally invasive advantage [11]. In the present study, post-operative inflammatory markers such as TLC and CRP were significantly lower in the MIPO group, suggesting a reduced systemic inflammatory response. Although limited studies have directly evaluated laboratory parameters, the reduced tissue handling and preservation of periosteal blood supply in MIPO are believed to contribute to a decreased inflammatory response and improved biological healing [6,11]. With respect to fracture healing, the MIPO group demonstrated a significantly shorter time to union, while overall union rates were comparable between the two groups. These findings are in agreement with previous studies and systematic reviews, which have shown either similar or slightly improved union times with MIPO, likely due to preservation of fracture haematoma and vascularity [6,12]. A recent study on radial shaft fractures also reported comparable union rates and functional outcomes between MIPO and ORIF, highlighting that both techniques are effective in achieving fracture healing [5]. The incidence of complications, including infection, non-union, and implant failure, was lower in the MIPO group in the present study, although the differences were not statistically significant. This trend is supported by existing literature, which suggests that MIPO may reduce soft-tissue complications and nerve injuries, although overall complication rates between the two techniques are often comparable [12,13]. In addition, systematic reviews have demonstrated lower risks of specific complications such as nerve palsy and surgical site morbidity with MIPO [13]. Functional outcomes were better in the MIPO group in this study, although not statistically significant. Similar observations have been reported in comparative studies, where MIPO provided equal or slightly improved functional scores due to reduced soft-tissue damage and earlier mobilisation [5,10]. However, some studies indicate that long-term functional outcomes tend to equalise between the two techniques, suggesting that both methods are clinically effective when performed appropriately [5]. Despite its advantages, MIPO is associated with certain limitations, including increased dependence on fluoroscopic guidance and a steeper learning curve for surgeons. Increased radiation exposure and potential for indirect reduction-related malalignment have been reported in previous studies, emphasising the need for adequate surgical expertise [11]. Therefore, careful patient selection and surgical proficiency are essential to maximise the benefits of MIPO. The present study has several limitations that should be acknowledged while interpreting the findings. First, the relatively small sample size may have limited the statistical power of the analysis and may restrict the generalisability of the results to a broader population. Second, the single-centre design further constrains external validity, as the findings may not fully represent variations in patient characteristics and clinical practices across different healthcare settings. Third, the absence of randomisation in patient allocation introduces a potential risk of selection bias, which could have influenced comparative outcomes between groups. In addition, the relatively short follow-up period of 6 months may not be sufficient to evaluate long-term outcomes, including delayed complications or late functional deterioration. These factors collectively suggest that while the observed results are clinically informative, they should be interpreted with caution, and larger multicenter randomised studies with extended follow-up are warranted to validate and strengthen the evidence base.
MIPO demonstrated superior perioperative outcomes compared to conventional plating, including reduced operative time, lower intraoperative blood loss, a decreased need for blood transfusion, and a shorter hospital stay. In addition, MIPO was associated with a lesser postoperative inflammatory response and better preservation of Hb levels. Although fracture union rates and complication profiles were comparable between the two techniques, MIPO showed a significantly shorter time to union and a trend toward improved functional outcomes. These findings suggest that MIPO is a safe and effective alternative to conventional plating, offering distinct perioperative advantages with comparable overall clinical outcomes.
MIPO offers significant perioperative advantages over conventional plating, particularly in reducing surgical trauma, blood loss, and hospital stay. The technique is associated with a lower inflammatory response and faster fracture healing, without increasing complication rates. These benefits make MIPO a preferable option in appropriately selected patients requiring fracture fixation. However, surgical expertise and proper patient selection remain critical to achieving optimal outcomes.
References
- 1. Keshav K, Baghel A, Kumar V, Neradi D, Kaustubh K, Mishra P. Is minimally invasive plating osteosynthesis better than conventional open plating for humeral shaft fractures? A systematic review and meta-analysis of comparative studies. Indian J Orthop 2021;55 Suppl 2:283-303. [Google Scholar] [PubMed]
- 2. Marazzi C, Wittauer M, Hirschmann MT, Testa EA. Minimally invasive plate osteosynthesis (MIPO) versus open reduction and internal fixation (ORIF) in the treatment of distal fibula Danis-Weber types B and C fractures. J Orthop Surg Res 2020;15:491. [Google Scholar] [PubMed]
- 3. Li F, Liu X, Wang F, Gu Z, Tao Q, Yao C, et al. Comparison between minimally invasive plate osteosynthesis and open reduction-internal fixation for proximal humeral fractures: A meta-analysis based on 1050 individuals. BMC Musculoskelet Disord 2019;20:550. [Google Scholar] [PubMed]
- 4. Jin C, Weng D, Yang W, He W, Liang W, Qian Y. Minimally invasive percutaneous osteosynthesis versus ORIF for Sanders type II and III calcaneal fractures: A prospective, randomized intervention trial. J Orthop Surg Res 2017;12:10. [Google Scholar] [PubMed]
- 5. Kang HT, Jo YH, Kang HJ. Comparison of minimally invasive plate osteosynthesis (MIPO) and open reduction and internal fixation (ORIF) for the treatment of radial shaft fractures: A retrospective study. BMC Musculoskelet Disord 2025;26:320. [Google Scholar] [PubMed]
- 6. Erivan R, Caputo T, Monadjemi S, Pereira B, Descamps S, Boisgard S, et al. A comparison of minimally invasive plate osteosynthesis (MIPO) versus open reduction and internal fixation (ORIF) in the management of tibial pilon fractures: A prospective randomized study. Orthop Traumatol Surg Res 2025;111:104323. [Google Scholar] [PubMed]
- 7. Sohn HS, Kim WJ, Shon MS. Comparison between open plating versus minimally invasive plate osteosynthesis for acute displaced clavicular shaft fractures. Injury 2015;46:1577-84. [Google Scholar] [PubMed]
- 8. Oh CW, Byun YS, Oh JK, Kim JJ, Jeon IH, Lee JH, et al. Plating of humeral shaft fractures: Comparison of standard conventional plating versus minimally invasive plating. Orthop Traumatol Surg Res 2012;98:54-60. [Google Scholar] [PubMed]
- 9. Charles-Lozoya S, López-Galindo E, Cobos-Aguilar H, Manilla-Muñoz E, De La Parra-Márquez ML, Arriaga-Cazares HE, et al. Operative time, postoperative pain, and functional recovery in MIPO versus ORIF for humeral shaft fractures: A retrospective cohort case series. Ann Med Surg (Lond) 2025;88:88-94. [Google Scholar] [PubMed]
- 10. Sugumar N, Sathiyaseelan N, Purushothaman JR, Natarajan S. Assessing functional and radiological outcomes: Open reduction and internal fixation vs. Minimally invasive plate osteosynthesis for humerus shaft fractures – a prospective comparative study. Int Orthop 2024;48:2979-91. [Google Scholar] [PubMed]
- 11. Kim YG, Park KH, Kim JW, Oh JK, Yoon JP, Kim HJ, et al. Is minimally invasive plate osteosynthesis superior to open plating for fixation of two-part fracture of the proximal humerus? J Orthop Surg (Hong Kong) 2019;27:2309499019836156. [Google Scholar] [PubMed]
- 12. Beeres FJ, Diwersi N, Houwert MR, Link BC, Heng M, Knobe M, et al. ORIF versus MIPO for humeral shaft fractures: A meta-analysis and systematic review of randomized clinical trials and observational studies. Injury 2021;52:653-63. [Google Scholar] [PubMed]
- 13. La Banca V, Lima GH, Vigano AV, Gonzalez FF, Schaffhausser HL, Almeida LH, et al. Complications and clinical outcomes with minimally invasive plate osteosynthesis (MIPO) technique for midshaft clavicle fractures: A systematic review and meta-analysis. JSES Int 2023;8:257-67. [Google Scholar] [PubMed]



Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 A Prospective Analysis of Physeal-Sparing Intramedullary Interlocking Nail for Adolescent Tibial Shaft Fractures
August 1, 2026 A Prospective Analysis of Physeal-Sparing Intramedullary Interlocking Nail for Adolescent Tibial Shaft Fractures August 1, 2026 Dual Fixation in Complex Long Bone Fractures: A Case Series of 30 Patients
August 1, 2026 Dual Fixation in Complex Long Bone Fractures: A Case Series of 30 Patients July 1, 2026 Fracture Fixation Sequencing in Polyskeletal Trauma: Clinical Experience from a Five-Patient Retrospective Series
July 1, 2026 Fracture Fixation Sequencing in Polyskeletal Trauma: Clinical Experience from a Five-Patient Retrospective Series May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing
May 1, 2026 Assessment of Teriparatide’s Effect on Post-operative Functional Outcome and Fracture Healing