
Pre-operative strengthening and neuromuscular training improve quadriceps strength and reduce pain before ACL reconstruction. Patients undergoing prehabilitation demonstrate better post-operative functional recovery and faster return to independent mobility.
Dr. Prajwal Ganesh Senthilnathan, Department of Orthopaedic, Rajam Multi-speciality Hospital, Tiruvannamalai, Tamil Nadu, India. Email: prajwal.ganesh@gmail.com
Abstract
Introduction: Anterior cruciate ligament (ACL) injury is a frequent orthopaedic problem which commonly leads to knee instability, loss of function, and delay in recovery. Even though ACL reconstruction (ACLR) is a common procedure, there are significant differences in the results that follow the procedure. Recent data indicate that prehabilitation, which is a rehabilitation performed before surgery, can enhance postoperative outcomes, although its use has not been widely incorporated into clinical practice yet.
Objectives: The objective of the study was to determine the efficacy of structured prehabilitation in enhancing the pain, muscle strength, functional outcomes, range of motion, and early postoperative recovery after ACLR.
Materials and Methods: A prospective comparative interventional study was done on 50 patients who had primary ACL repair in a tertiary care hospital. The participants were separated into two groups: Group A (n = 25) underwent a structured prehabilitation before surgery, and Group B (n = 25) underwent the usual care that did not involve prehabilitation. Prehabilitation involved strengthening, range-of-motion, balance, proprioception, and patient education. The two groups were subjected to the same postoperative rehabilitation programme. Measures of outcomes such as strength of the quadriceps, pain level with the visual analogue scale (VAS), knee range of motion, functional outcome scores, time to ambulate independently, and overall post-operative outcome were also evaluated.
Findings: The prehabilitation group had better pre-operative quadriceps strength (4.1 ± 0.6 vs 3.5 ± 0.7) and low pre-operative pain scores (4.2 ± 0.9 vs 5.1 ± 1.0). During the post-operative period, Group A had a significantly lower pain level at 6 weeks (2.1 ± 0.7 vs. 3.4 ± 0.8) and had a higher knee range of motion (128.5 ± 6.2 vs. 118.3 ± 7.1). The prehabilitation group had more favourable functional outcome scores at 3 months (86.4 ± 5.8 vs. 78.2 ± 6.4). Excellent overall results were more common in the prehabilitation group (72% vs. 40 per cent of Group A vs. Group B).
Conclusion: Pre-operative structured prehabilitation before ACLR is an important factor in the management of post-operative pain, functional outcome, muscle strength, and early mobility. Prehabilitation can be implemented as a part of the standard ACLR care to potentially improve the outcomes of the surgery and recovery of patients.
Keywords: Anterior cruciate ligament reconstruction, knee function, prehabilitation, post-operative recovery, physiotherapy.
An anterior cruciate ligament (ACL) injury is a common knee injury in sports, especially among the young, physically active population, and is likely to result in knee instability, functional loss, and premature osteoarthritis unless well managed [1]. ACL reconstruction (ACLR) is the current operation used to restore knee stability and allow the patient to resume sports and everyday activities; nevertheless, the outcomes of the postoperative period differ significantly among patients despite the improved approach to surgery and rehabilitation regimen [2]. Recovery following ACLR is affected by a number of factors, among them being pre-operative knee functioning, muscle strength, range of motion, neuromuscular control, psychological preparedness, and compliance with rehabilitation programmes [3]. The traditional focus has been on the post-operative rehabilitation time with little formal consideration of the pre-operative time. The idea of prehabilitation, which is considered to be purposeful physical and psychological interventions before surgery to increase post-operative recovery, has been gaining popularity in orthopaedic and sports medicine within recent years [4]. Prehabilitation should be used to maximise the functional state of the patient before “ACLR”, with a focus on quadriceps and hamstring strength, decreasing knee effusion, restoring full movement considerations, proprioception, and psychological issues such as fear of motion and low self-efficacy [5]. The weakness of the quadriceps has been thoroughly reported as one of the outcomes of ACL injury and is highly correlated with poor functional results after ACLR [6]. Research has revealed that patients who arrive in surgery with excellent quadriceps strength and neuromuscular control portray quicker recovery of strength after surgery and excellent functional performance [7]. Furthermore, pre-operative losses in knee extension and sustained swelling have been associated with arthrofibrosis, slow rehabilitation, and poor long-term recovery after reconstruction [8]. Strength training, neuromuscular training, balance training, and movement retraining have been proved to be effective in prehabilitation programmes to enhance pre-operative functional scores and minimise post-operative deficits [9]. Moreover, symmetrical movement pattern restoration in the pre-operative phase can help to eliminate maladaptive motor strategies that remain after surgery [10]. In addition to physical conditioning, psychological preparation is also important in post-ACLR recovery. Kinesiophobia, fear of reinjury, and lack of confidence have been found to be significant impediments to return to sport (RTS) even with patients who have good physical recovery [11]. Prehabilitation offers a chance to teach patients about their surgery, the post-operative experience, and the milestones of rehabilitation and decrease anxiety and enhance motivation and compliance with the post-operative rules [12]. There is evidence to indicate that patients undergoing organised pre-operative programmes achieve better patient-reported outcome measures and an increased rate of RTSs, as well as overall patient satisfaction following ACLR [13]. Although more and more evidence is pointing towards prehabilitation, it is still not fully adopted in clinical practice because of time constraints, limited resources, and poorly standardised protocols [14]. In addition, the difference in the programme length, exercise elements, and results of the studies has led to the heterogeneity of the results, and it is hard to conclude about the effectiveness of the programme in general. Underdeveloped countries such as India may have a shortage of monitored pre-operative rehabilitation, and the role of prehabilitation in enhancing surgical outcomes is not well studied. To come up with cost-effective evidence-based care pathways, it is important to understand how prehabilitation affects post-operative pain, functional recovery, muscle strength, and return-to-activity. Hence, the present research should be a comparative assessment of the benefits of structured prehabilitation in enhancing post-operative outcomes after ACLR, aimed at maximising the recovery, increasing the functional performance, and improving the quality of life of ACLR patients.
Study design:
This study was conducted as a multicentric, prospective, comparative, interventional study across the departments of orthopaedics and physiotherapy at multiple tertiary care teaching hospitals. The study protocol was approved by the institutional ethics committees of all participating centres, and written informed consent was obtained from all patients before inclusion in the study.
Study setting:
The study was carried out in collaboration between the Departments of Orthopaedics and Physiotherapy at participating tertiary care teaching hospitals. All surgical procedures were performed by experienced orthopaedic surgeons at their respective centres, and rehabilitation sessions were supervised by qualified physiotherapists following standardised protocols to ensure uniformity of treatment across all study sites.
Study duration:
The total duration of the study was 12 months. This period included patient recruitment, implementation of the prehabilitation protocol, surgical intervention, post-operative rehabilitation, and follow-up assessments. Each participant was followed from the pre-operative period until completion of the early post-operative rehabilitation phase.
Participants:
Patients diagnosed with ACL injury and planned for ACLR were screened for eligibility.
Inclusion criteria:
- Patients aged between 18 and 45 years
- Clinically and radiologically confirmed ACL tear
- Patients planned for primary ACLR
- Patients willing to participate and provide informed consent
- Patients able to follow rehabilitation instructions.
Exclusion criteria:
- Multiligament knee injuries
- Associated fractures around the knee
- Previous surgery on the affected knee
- Advanced osteoarthritis of the knee joint
- Neurological disorders affecting lower limb function
- Patients medically unfit for surgery or exercise therapy.
Study sampling:
A non-probability purposive sampling technique was used to select participants who met the inclusion criteria. Eligible patients presenting to the orthopaedic outpatient department during the study period were approached consecutively and enrolled after obtaining informed consent.
Study sample size:
The total sample size for the study was 50 participants. The sample size was determined based on feasibility, availability of eligible patients during the study period, and institutional constraints. All enrolled participants completed the study protocol.
Study groups:
Participants were divided into two equal groups, with 25 patients in each group.
- Group A (Prehabilitation Group): Patients received a structured prehabilitation programme before ACLR in addition to standard post-operative rehabilitation.
- Group B (Control Group): Patients received standard care without structured prehabilitation and underwent routine postoperative rehabilitation only.
Study parameters:
The following parameters were assessed to evaluate outcomes:
- Quadriceps and hamstring muscle strength
- Knee range of motion
- Pain intensity using VAS
- Functional outcome using standardised knee scoring systems
- Time to achieve post-operative rehabilitation milestones
- Patient-reported functional recovery
These parameters were assessed pre-operatively and during the post-operative follow-up period.
Study procedure:
On recruitment, a baseline of demographic and clinical information was collected among all the participants. Group A patients went through a formal pre-operative course for a specified time before surgery. The programme involved strengthening exercises of the quadriceps and hamstrings, range-of-motion exercises, balance and proprioceptive training, and patient education as per post-operative expectations. Group B patients were not given structured prehabilitation and took standard preoperative advice. The participants were then all subjected to arthroscopic ACLR done in the normal surgical procedure. Both groups also received the same standardised rehabilitation protocol to ensure a reduction in treatment bias in the post-operative period.
Study data collection:
Data were collected using a structured data collection form. Baseline assessments were performed before surgery, including pain scores, range of motion, and functional status. Post-operative assessments were conducted at scheduled follow-up visits. All measurements were recorded by trained assessors using standardised assessment tools to ensure consistency and reliability of data.
Data analysis:
Collected data were entered into Microsoft Excel and analyzed using Statistical Package for the Social Sciences software. Descriptive statistics such as mean, standard deviation, frequency, and percentage were used to summarize demographic and clinical variables. Inferential statistics were applied to compare outcomes between the two groups. Appropriate statistical tests were used based on data distribution, and a P < 0.05 was considered statistically significant.
Ethical considerations:
Ethical permission to conduct the study was granted by the Institutional Ethics Committee before the study began. All participants gave informed consent in writing after being informed about the objectives of the study, the procedures, the risks, and the benefits. The privacy of the information of the participants was granted during the study, and they were assured of their right to leave the study any time without interfering with their medical services. The research was carried out in line with the ethical principles contained in the Declaration of Helsinki.
Demographic and clinical characteristics of participants:
The majority of participants were aged 26–35 years (46%), and male patients predominated (74%), which reflects the typical epidemiology of ACL injuries among young active individuals. Both groups were comparable in age, gender distribution, and side of injury, indicating baseline similarity between groups (Table 1).
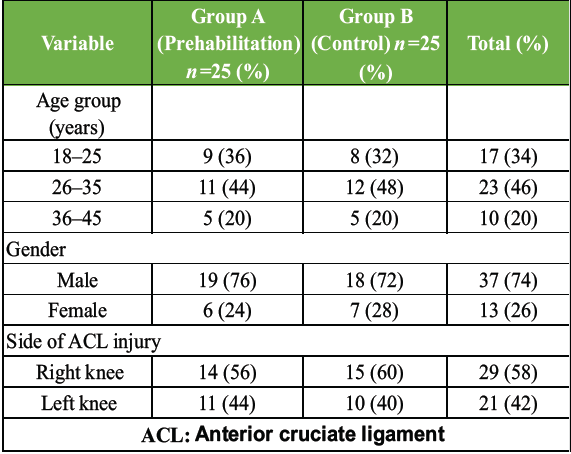
Table 1: Demographic and clinical characteristics of participants
Preoperative clinical parameters:
Participants who underwent prehabilitation demonstrated higher quadriceps strength and lower pain scores before surgery compared to the control group, suggesting that structured preoperative exercises improve muscle conditioning and reduce symptoms before ACLR (Table 2 and Fig. 1).
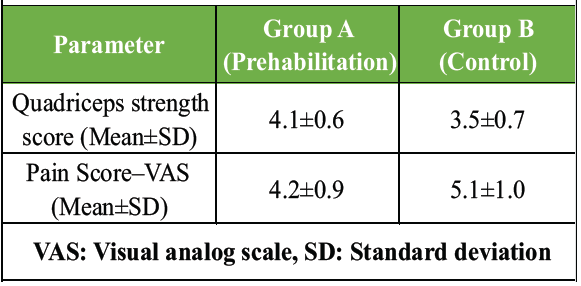
Table 2: Pre-operative clinical parameters
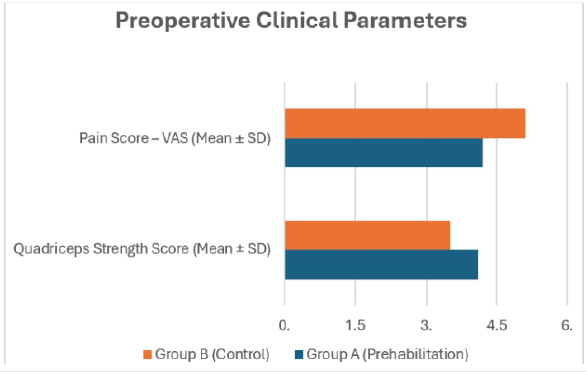
Figure 1: Preoperative Clinical Parameters
Post-operative clinical outcomes:
Patients in the prehabilitation group showed lower postoperative pain, better knee range of motion, and higher functional outcome scores, indicating that prehabilitation enhances early postoperative recovery and functional performance after ACLR (Table 3 and Fig. 2).
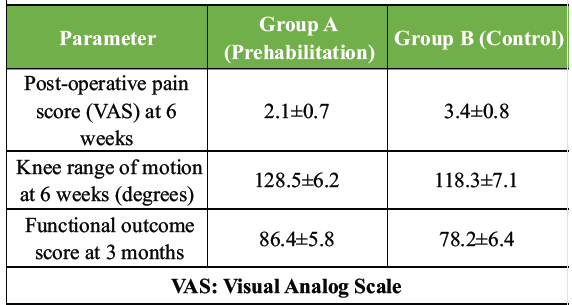
Table 3: Post-operative clinical outcomes
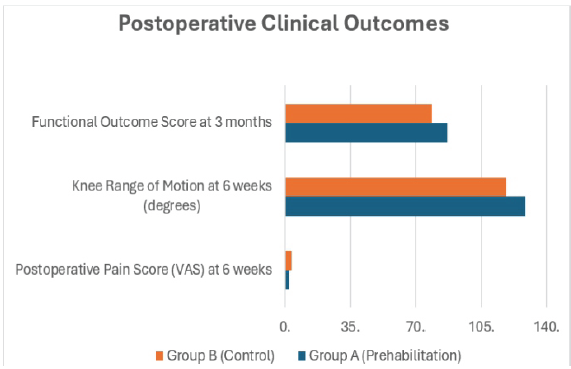
Figure 2:Postoperative Clinical Outcomes
Recovery milestones and overall outcome:
A significantly higher proportion of patients in the prehabilitation group achieved early independent walking and excellent post-operative outcomes, highlighting the positive role of pre-operative rehabilitation in accelerating recovery and improving surgical outcomes (Table 4 and Fig. 3).
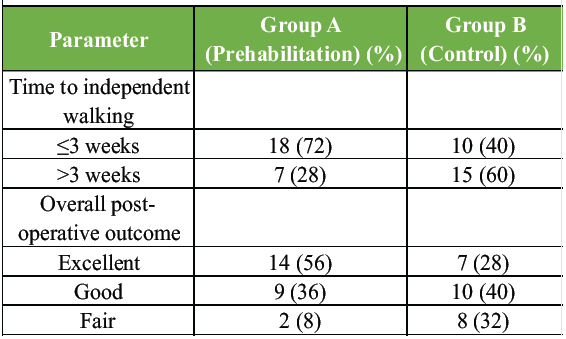
Table 4: Recovery milestones and overall outcome
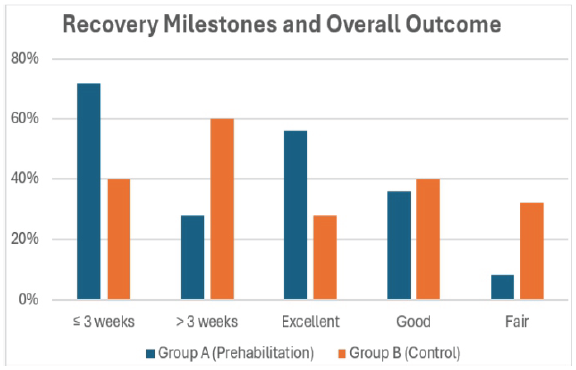
Figure 3:Recovery Milestones and Overall Outcome
The given research examined the value of structured prehabilitation in enhancing post-operative results after ACLR and showed that the patients with pre-operative rehabilitation recorded consistently better outcomes in a variety of clinical and functional measures as compared to the patients treated with standard care only. The study population is characterised by the demographic distribution of the participants (mostly young adults aged 2635 years, 46%, and a larger number of male participants, 74%), which is consistent with the normal epidemiology of ACL injuries, which has been reported in the literature. The comparability of the baseline between the prehabilitation and the control group, considering age, sex distribution, and side of injury, meant that the observed postoperative differences could be due to the influence of prehabilitation and not the intervening factors. Among the most significant results of the given study was the fact that the pre-operative quadriceps strength was clearly more advanced in the prehabilitation group (4.1 ± 0.6) as opposed to the control group (3.5 ± 0.7). This result is similar to the systematic review conducted by Giesche et al. (2020) [15], who showed greater increases in maximal quadriceps torque between baseline and pre-reconstruction in prehabilitation groups and limb symmetry index improvements over controls. This capacity to increase the quadriceps strength before surgery is a clinically significant factor since quadriceps weakness is a significant predictor of slow functional recovery and long-term functional deficiency after ACLR. The current study also found the pre-operative level of pain was lower in the prehabilitation group, with the mean VAS scores of 4.2 ± 0.9 as compared to the control group of 5.1 ± 1.0. Although the study of Carter et al. (2020) [16] found no consistent results about the pain reduction after prehabilitation, as one randomised controlled study reported no essential difference in the pain outcomes, the positive result obtained in the given study provides evidence that the targeted exercise and neuromuscular training can help change the perception of pain and decrease the level of joint irritability before surgery. Notably, pain after surgery decreased more, with higher VAS scores recorded at six weeks after the surgery at a significantly lower level in the prehabilitation group (2.1 ± 0.7) than the controls (3.4 ± 0.8). These results indicate the idea suggested by Fu et al. (2025) [17] when the 12-month pain control is better in the group where prehabilitation was performed, as the scores of pain in the prehabilitation group were 0.0 and 1.0 in the non-prehabilitation group. The prehabilitation group was significantly more improved on functional recovery after ACLR. In the current research, the knee range of motion was significantly higher in patients who received prehabilitation at 6 weeks after operation (128.5 ± 6.2) than it was in controls (118.3 ± 7.1). Knee range of motion restoration is of utmost importance in the prevention of stiffness and arthrofibrosis, and these results correspond to the conclusions of Zakharia et al. (2025) [18], who documented that modern prehabilitation activities focus on impairment resolution and the restoration of the range of motion, as well as that patients following prehabilitation achieved and exceeded patient-acceptable symptom state thresholds. There was also a higher functional outcome score at 3 months post-operatively in the prehabilitation group (86.4 ± 5.8) than in the control group (78.2 ± 6.4), which indicated better recovery of knee functions. Giesche et al. (2020) [15] reported clinically significantly better results of self-reported knee functioning before reconstruction and at a 2-year follow-up of patients receiving prehabilitation. The positive impact of prehabilitation is further brought out by the rapid attainment of functional milestones. In the current study, 72% of patients in the prehabilitation group were able to walk on their own within 3 weeks after surgery as opposed to 40% of the control group. Such a quicker recovery course resembles results by Fu et al. (2025) [17], which showed that prehabilitation shortened recovery time by 2.6 weeks (7.2 weeks vs. 9.8 weeks) and was the most powerful predictor of enhanced knee functioning. On the same note, Giesche et al. (2020) [15] showed that there was a tendency to have faster RTS in prehabilitation groups, and more RTS was reported in one of the included studies at 2 years post-intervention. Even though RTS was not directly measured in the present study, the increased early functional outcomes and accelerated ambulation seen indicate a possible positive effect on the longer-term return-to-activity outcomes. The general distribution of the post-operative outcome in the current study also supports the clinical importance of prehabilitation. There were significant improvements in 56% of the patients who took prehabilitation and fair improvement in the control group (32 vs. 8), and excellent outcomes were more prevalent in the prehabilitation group (56 vs. 28). Such data can be explained by the findings of Shaarani et al. (2013) [19], who showed sustained changes in single-leg hop performance and the modified Cincinnati Knee Rating System over 12 weeks post-operatively in patients who received a 6-week progressive prehabilitation course. Interestingly, Shaarani et al. also reported mechanistic information, and as they noted, prehabilitation led to increased expression of hypertrophic IGF-1 genes and favourable changes in muscle fibre composition, a fact that could be partially responsible for the better functional recovery in their study and the current one. Although Carter et al. (2020) [16] found extremely low-quality evidence and emphasised the variability of prehabilitation programme content, frequency, and duration, they still found statistically significant change in quadriceps strength and single-leg hop performance at 3 months’ follow-up after ACLR in favour of prehabilitation. These reported benefits are thus consistent with the findings of the present study of improved quadriceps strength, functional scores, and early mobility even though the programmes were designed differently and the outcome measures varied. Notably, Zakharia et al. (2025) [18] systematic review further confirms the safety and efficacy of prehabilitation with no pre-operative complications and similar post-operative complication rates as standard care and retains functional improvements up to 10 years after operation.” Even though the present study did not measure long-term outcomes, it is evident that the observed consistent early benefits indicate a positive course towards long-term recovery. Nevertheless, in spite of its advantages, the current study has been limited in several aspects, such as the size of the sample and the duration of the follow-up recruited, which did not allow the researcher to evaluate further results of the intervention, such as returning to sport and graft survival. However, the uniformity of the gains in pain, strength, range of motion, functional scores, and recovery milestones is a compelling point that can be used to support the idea of introducing structured prehabilitation into the regular treatment of ACLR. The findings, when interpreted in conjunction with available literature, support the rising literature that prehabilitation is a safe, effective, and clinically meaningful intervention that maximises neuromuscular preparedness, improves post-operative recovery, and enhances patient-reported outcomes after ACLR.
The current research finds out that prehabilitation before ACLR is an important process that helps in improving the post-surgery outcomes. Pre-operative rehabilitation patients boasted of superior quadriceps strength, lower pain levels, greater knee range of motion, faster functional milestones attained, and better overall functional outcomes than those who were only subjected to standard care. Prehabilitation established advantageous pre-operative conditioning and neuromuscular control that developed a positive post-operative recovery in terms of patient-reported ability and earlier mobility. These conclusions uphold the importance of structured prehabilitation programmes as a part and parcel of an overall ACLR management to enhance recovery and functional performance.
Structured prehabilitation before ACL reconstruction significantly improves post-operative recovery, functional outcomes, and early mobility. Incorporating prehabilitation into routine ACL management may enhance surgical success and patient quality of life.
References
- 1. Van Melick N, Van Cingel RE, Brooijmans F, Neeter C, Van Tienen T, Hullegie W, et al. Evidence-based clinical practice update: Practice guidelines for anterior cruciate ligament rehabilitation based on a systematic review and multidisciplinary consensus. Br J Sports Med 2016;50:1506-15. [Google Scholar] [PubMed]
- 2. Wright RW, Haas AK, Anderson J, Calabrese G, Cavanaugh J, Hewett TE, et al. Anterior cruciate ligament reconstruction rehabilitation: MOON guidelines. Sports Health 2015;7:239-43. [Google Scholar] [PubMed]
- 3. Kyritsis P, Bahr R, Landreau P, Miladi R, Witvrouw E. Likelihood of ACL graft rupture: Not meeting six clinical discharge criteria before return to sport is associated with a four times greater risk of rupture. Br J Sports Med 2016;50:946-51. [Google Scholar] [PubMed]
- 4. Herring SA, Kibler WB, Putukian M. The team physician and the return-to-play decision: A consensus statement-2012 update. Med Sci Sports Exerc 2012;44:2446-8. [Google Scholar] [PubMed]
- 5. Creighton DW, Shrier I, Shultz R, Meeuwisse WH, Matheson GO. Return-to-play in sport: A decision-based model. Clin J Sport Med 2010;20:379-85. [Google Scholar] [PubMed]
- 6. Shrier I. Strategic assessment of risk and risk tolerance (StARRT) framework for return-to-play decision-making. Br J Sports Med 2015;49:1311-5. [Google Scholar] [PubMed]
- 7. Barber-Westin SD, Noyes FR. Objective criteria for return to athletics after anterior cruciate ligament reconstruction and subsequent reinjury rates: A systematic review. Phys Sportsmed 2011;39:100-10. [Google Scholar] [PubMed]
- 8. Barber-Westin SD, Noyes FR. Factors used to determine return to unrestricted sports activities after anterior cruciate ligament reconstruction. Arthroscopy 2011;27:1697-705. [Google Scholar] [PubMed]
- 9. Hildebrandt C, Muller L, Zisch B, Huber R, Fink C, Raschner C. Functional assessments for decision-making regarding return to sports following ACL reconstruction. Part I: Development of a new test battery. Knee Surg Sports Traumatol Arthrosc 2015;23:1273-81. [Google Scholar] [PubMed]
- 10. Ashigbi EY, Banzer W, Niederer D. Return to sport tests’ prognostic value for reinjury risk after anterior cruciate ligament reconstruction: A systematic review. Med Sci Sports Exerc 2019;52:1263-71. [Google Scholar] [PubMed]
- 11. Paterno MV, Schmitt LC, Ford KR, Rauh MJ, Myer GD, Huang B, et al. Biomechanical measures during landing and postural stability predict second anterior cruciate ligament injury after anterior cruciate ligament reconstruction and return to sport. Am J Sports Med 2010;38:1968-78. [Google Scholar] [PubMed]
- 12. Paterno MV, Rauh MJ, Schmitt LC, Ford KR, Hewett TE. Incidence of second ACL injuries 2 years after primary ACL reconstruction and return to sport. Am J Sports Med 2014;42:1567-73. [Google Scholar] [PubMed]
- 13. Niederer D, Engeroff T, Wilke J, Vogt L, Banzer W. Return to play, performance, and career duration after anterior cruciate ligament rupture: A case-control study in the five biggest football nations in Europe. Scand J Med Sci Sports 2018;28:2226-33. [Google Scholar] [PubMed]
- 14. Eitzen I, Holm I, Risberg MA. Preoperative quadriceps strength is a significant predictor of knee function two years after anterior cruciate ligament reconstruction. Br J Sports Med 2009;43:371-6. [Google Scholar] [PubMed]
- 15. Giesche F, Niederer D, Banzer W, Vogt L. Evidence for the effects of prehabilitation before ACL-reconstruction on return to sport-related and self-reported knee function: A systematic review. PloS One 2020;15:e0240192. [Google Scholar] [PubMed]
- 16. Carter HM, Littlewood C, Webster KE, Smith BE. The effectiveness of preoperative rehabilitation programmes on postoperative outcomes following anterior cruciate ligament (ACL) reconstruction: A systematic review. BMC Musculoskelet Dis 2020;21:647. [Google Scholar] [PubMed]
- 17. Fu Y, Tian Y, Zhao Z, Li Z. Prehabilitation enhances functional and structural recovery following anterior cruciate ligament reconstruction: A randomized controlled trial. Knee Surg Sports Traumatol Arthrosc 2025;???:1-12. [Google Scholar] [PubMed]
- 18. Zakharia A, Zhang K, Al‐Katanani F, Rathod P, Uddandam A, Kay J, et al. Prehabilitation prior to anterior cruciate ligament reconstruction is a safe and effective intervention for short‐to long‐term benefits: A systematic review. Knee Surg Sports Traumatol Arthrosc 2025;33:4148-66. [Google Scholar] [PubMed]
- 19. Shaarani SR, O’Hare C, Quinn A, Moyna N, Moran R, O’Byrne JM. Effect of prehabilitation on the outcome of anterior cruciate ligament reconstruction. Am J Sports Med 2013;41:2117-27. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 May 1, 2026 Comparative Effects of Therapeutic Exercise versus Muscle Energy Technique Combined with Transcutaneous Electrical Nerve Stimulation on Pain, Range of Motion, and Functional Outcomes after Anterior Cruciate Ligament Reconstruction: A Prospective Pilot Study
May 1, 2026 Comparative Effects of Therapeutic Exercise versus Muscle Energy Technique Combined with Transcutaneous Electrical Nerve Stimulation on Pain, Range of Motion, and Functional Outcomes after Anterior Cruciate Ligament Reconstruction: A Prospective Pilot Study August 1, 2026 CT-Based Tunnel Position Analysis and its Correlation with Residual Instability after Anterior Cruciate Ligament Reconstruction
August 1, 2026 CT-Based Tunnel Position Analysis and its Correlation with Residual Instability after Anterior Cruciate Ligament Reconstruction August 1, 2026 Comparative Outcomes of Hamstring Tendon versus Peroneus Longus Tendon Autograft in Arthroscopic Single-Bundle Anterior Cruciate Ligament Reconstruction: A Prospective Comparative Study
August 1, 2026 Comparative Outcomes of Hamstring Tendon versus Peroneus Longus Tendon Autograft in Arthroscopic Single-Bundle Anterior Cruciate Ligament Reconstruction: A Prospective Comparative Study July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study
July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study