
Local infiltration analgesia with a ropivacaine-based cocktail provides superior postoperative pain control with fewer complications and promotes early mobilization and enhanced recovery following primary total knee arthroplasty.
Dr Rohit Patil Badarli, Department of Orthopaedics Vydehi Institute of Medical Sciences and Research Centre Whitefield, Bengaluru - 560066, Karnataka, India. E-mail: rohitpatilbadarli@gmail.com
Abstract
Introduction: Post-operative pain following total knee arthroplasty (TKA) poses a significant challenge, often limiting early mobilisation and delaying rehabilitation. While epidural analgesia with bupivacaine has been widely used, it is associated with complications such as motor block and hypotension, which may impair functional recovery. Local infiltration analgesia (LIA) using ropivacaine-based cocktails has emerged as a potential alternative with a better safety profile and effective pain control.
Materials and Methods: This prospective, randomised comparative study was conducted on 50 patients undergoing primary TKA. The participants were divided into two groups: Group A received intra-articular infiltration of 150 mg of 0.75% ropivacaine combined with ketorolac, adrenaline, and clonidine at the end of surgery, whereas Group B received postoperative epidural infusion of 0.125% bupivacaine. Post-operative pain was assessed using the Visual Analogue Scale (VAS) at 6, 12, 18, 24, and 48 h. Additional outcomes measured included the need for rescue analgesia, the incidence of complications (motor block, hypotension, nausea, and vomiting), and functional outcomes such as time to ambulation and range of motion (ROM).
Results: The study demonstrated that Group A had significantly lower VAS scores at all time intervals, indicating better analgesic efficacy. Only 32% of patients in Group A required rescue analgesia compared to 84% in Group B. Moreover, Group B had a higher incidence of motor block and hypotension, which adversely affected early mobilisation. Nausea and vomiting were also more commonly observed in Group B. Patients in the local infiltration analgesia group showed improved functional outcomes, including earlier ambulation and better ROM at 48 h postoperatively.
Conclusion: Local infiltration of a ropivacaine cocktail offers superior pain relief, reduces the need for rescue analgesia, and results in fewer complications compared to post-operative epidural bupivacaine. This technique facilitates faster recovery and enhances patient satisfaction following total knee replacement, making it a safer and more effective approach for post-operative analgesia.
Keywords: Total knee arthroplasty, ropivacaine, epidural bupivacaine, local infiltration analgesia, postoperative pain, Visual Analogue Scale, rescue analgesia, motor block.
Total knee arthroplasty (TKA) is one of the most commonly performed procedures in orthopaedics for the management of end-stage knee osteoarthritis. It is considered highly successful in relieving pain, restoring function, and improving quality of life in patients with degenerative joint disease of the knee [1]. Despite these benefits, TKA is frequently associated with significant postoperative pain, particularly in the early recovery period. Studies indicate that over 60% of patients experience severe post-operative pain in the first 36 h, and around 30% experience moderate pain [2]. Inadequate post-operative pain control not only impedes early mobilisation and physiotherapy but can also lead to delayed recovery, increased morbidity, prolonged hospital stays, and diminished patient satisfaction [3]. The Joint Commission on Accreditation of Healthcare Organisations has emphasised the importance of pain management by designating pain as the “fifth vital sign”, underscoring its essential role in post-operative care [4]. Effective analgesia following TKA is thus critical for facilitating early ambulation, reducing hospital stay, enabling early discharge, and achieving optimal functional outcomes [5]. Furthermore, it can also minimise the risk of complications such as deep vein thrombosis, pulmonary embolism, and nosocomial infections, which are associated with immobility [6]. Traditionally, continuous epidural analgesia using agents such as bupivacaine has been a standard modality for post-operative pain management following lower limb surgeries. While effective, this technique has limitations. Epidural analgesia is associated with adverse effects, including motor block, urinary retention, hypotension, pruritus, and delayed ambulation, which may hinder rehabilitation efforts [7,8]. Moreover, the technical demands and the need for close monitoring of patients receiving epidural analgesia make it less favourable in certain settings. To overcome these limitations, alternative techniques such as local infiltration analgesia (LIA) have gained popularity. LIA involves the periarticular injection of a combination of analgesic agents, such as ropivacaine, ketorolac, clonidine, and adrenaline, into the tissues surrounding the joint during surgery. This approach offers several advantages, including ease of administration, minimal systemic side effects, reduced opioid requirement, and preservation of motor function [9]. The technique, originally described by Kerr and Kohan, has since been widely adopted due to its safety and efficacy in TKA [10]. Ropivacaine, an amide-type local anaesthetic with reduced cardiotoxicity compared to bupivacaine, is commonly used in LIA protocols. It provides effective sensory blockade with minimal motor blockade, thereby supporting early mobilisation [11]. The addition of ketorolac, a non-steroidal anti-inflammatory drug (NSAID), enhances the anti-inflammatory and analgesic effects of the cocktail, whereas adrenaline prolongs the duration of action through local vasoconstriction [12]. Numerous studies have demonstrated the efficacy of LIA in reducing postoperative pain, opioid consumption, and hospital stay. Xu et al. conducted a meta-analysis of randomised controlled trials and concluded that single-dose LIA significantly reduced VAS scores at multiple postoperative intervals and facilitated faster rehabilitation without increasing complications [13]. Similarly, Niemeläinen et al. and Lamplot et al. reported that patients receiving intraoperative LIA required less rescue analgesia, had fewer opioid-related side effects, and achieved better functional outcomes compared to those managed with intravenous (IV) opioids or epidural analgesia [14,15]. Given the growing interest in optimising multimodal analgesia strategies in TKA, this study was undertaken to compare the analgesic efficacy, complication rates, and functional recovery associated with intra-articular local infiltration of a ropivacaine cocktail versus postoperative epidural bupivacaine (EB) infusion.
This study was designed as a prospective, randomised, comparative clinical trial conducted at the Department of Orthopaedics, Vydehi Institute of Medical Sciences and Research Centre, Bengaluru, with IEC NO: VIEC/2022/APP/PG/095, approved on July 21, 2022. After obtaining clearance from the Institutional Ethical Committee, 50 adult patients scheduled for primary unilateral TKA were enrolled in the study. Written informed consent was obtained from all participants before surgery, in accordance with the ethical standards laid out in the Declaration of Helsinki [16]. Inclusion criteria consisted of patients aged between 50 and 80 years, with a radiologically and clinically confirmed diagnosis of end-stage osteoarthritis of the knee, who were planned for elective primary TKA under spinal anaesthesia. Patients with an American Society of Anaesthesiologists physical status of I–III were included. Exclusion criteria included patients with a known allergy to local anaesthetics or NSAIDs, history of coagulopathy, chronic opioid use, psychiatric illness affecting pain perception, revision arthroplasty, spinal abnormalities preventing neuraxial blockade, and those unwilling to participate. Patients were randomly divided into two groups (Group A and Group B) using a computer-generated randomisation table. Group A (LIA): Received 150 mg of 0.75% ropivacaine (20 mL), 30 mg of ketorolac (1 mL), 1 mL of adrenaline (1:1000), and 1 mL of clonidine (150 µg) diluted to a total of 50 mL with normal saline. The cocktail was infiltrated intraoperatively into the periarticular tissues at the end of the surgery by the operating surgeon. The injection sites included the posterior capsule, medial and lateral collateral ligaments, extensor retinaculum, periosteum, and subcutaneous tissues [9,10]. Group B (EB): Received 0.125% bupivacaine administered through an epidural catheter postoperatively. The epidural catheter was placed preoperatively at the lumbar level under aseptic conditions after spinal anaesthesia. A bolus of 8 mL was administered at skin closure, followed by 5 mL every 8 h for 48 h. All patients underwent TKA under spinal anaesthesia using 3 mL of 0.5% hyperbaric bupivacaine. A standardised medial parapatellar approach was used. In all cases, cemented implants were used, and surgeries were performed by experienced orthopaedic surgeons. Post-operative pain was evaluated using the Visual Analogue Scale (VAS) at 6, 12, 18, 24, and 48 h after surgery. Rescue analgesia in the form of IV paracetamol 1 g was administered when VAS ≥ 4, and the requirement for rescue analgesics was recorded. Additional parameters included the incidence of post-operative complications such as motor block (graded through Bromage score), hypotension, nausea, and vomiting [17]. Functional outcomes such as time to independent ambulation and knee range of motion (ROM) were assessed at 48 h postoperatively by a blinded physiotherapist. The presence of complications related to either analgesic technique was also documented. Statistical analysis was conducted using the Statistical Package for the Social Sciences software version 22. Continuous variables such as age and VAS scores were expressed as mean ± standard deviation and compared using the independent t-test. Categorical variables such as gender, rescue analgesia requirement, and complication rates were analysed using the Chi-square test or Fisher’s exact test where appropriate. P < 0.05 was considered statistically significant. The choice of analgesic agents and dosages for LIA was based on previously validated protocols in the literature, including those by Kerr and Kohan [9] and Andersen and Kehlet [5], which demonstrated that a multimodal intraoperative infiltration approach results in significantly reduced opioid consumption, better pain scores, and early mobilisation following TKA.
A total of 50 patients undergoing primary unilateral TKA were enrolled in the study. Patients were randomly assigned to two equal groups of 25 each: Group A received LIA using a ropivacaine cocktail, and Group B received postoperative epidural analgesia with bupivacaine. All patients completed the study, and there were no dropouts.
Demographic characteristics:
The baseline characteristics, including age, gender, and comorbidities such as diabetes and hypertension, were comparable between the two groups. The mean age in Group A was 58 ± 10.4 years, whereas that in Group B was 61.4 ± 11.6 years (P = 0.28), indicating no statistically significant difference (Table 1). Both groups had a similar male-to-female distribution (Group A: 14 males, 11 females; Group B: 12 males, 13 females; P = 0.56), as shown in Table 2.
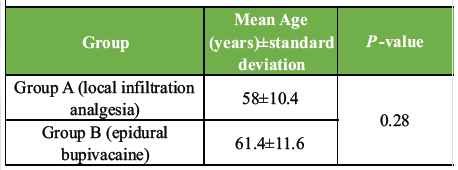 Table 1: Comparison of age between the two groups
Table 1: Comparison of age between the two groups
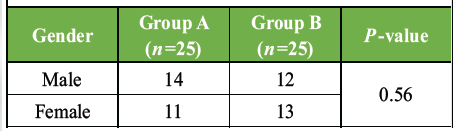 Table 2: Distribution according to gender
Table 2: Distribution according to gender
Pain scores (VAS assessment):
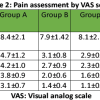
Pain was assessed using the VAS preoperatively and at 6, 12, 18, 24, and 48 h postoperatively. Group A consistently demonstrated significantly lower mean VAS scores at all time intervals postoperatively compared to Group B, suggesting superior analgesic efficacy of LIA (Table 3). For instance, at 6 h postoperatively, the VAS score in Group A was 5.7 ± 0.84, whereas it was 6.3 ± 1.1 in Group B (P < 0.05). This pattern persisted across all time points up to 48 h, as confirmed in earlier trials by Andersen and Kehlet, and Kerr and Kohan [5,9].
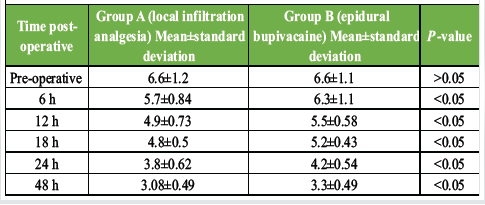
Table 3: VAS scores at different time intervals
Rescue analgesia requirement:
The need for additional analgesia (IV paracetamol 1 g) was significantly lower in Group A. Only 8 out of 25 patients (32%) in Group A required rescue analgesia, compared to 21 out of 25 patients (84%) in Group B (P < 0.05), as shown in Table 4. These findings align with previous studies that demonstrate reduced opioid and analgesic requirements with LIA techniques [10].
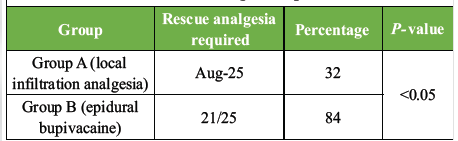
Table 4. Rescue analgesia requirement
Post-operative functional outcomes:
At 48 h, significantly more patients in Group A were independently ambulatory (16/25; 64%) compared to Group B (9/25; 36%) (P < 0.05) (Table 5). In addition, Group A showed a larger number of patients who achieved a full range of knee motion, 14 (56%) versus 7 (28%) in Group B (P < 0.05). Early ambulation and ROM are crucial for TKA recovery and are supported by findings from Niemeläinen et al. and Lamplot et al. [14,15].
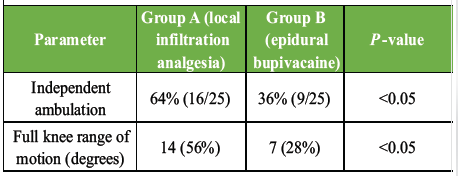
Table 5: Functional recovery parameters at 48 h
Post-operative complications:
Group B exhibited a higher incidence of complications. A motor block occurred in 4 (16%) of patients in Group B, compared to 2 (8%) in Group A (P < 0.05). Hypotension was observed in 5 (20%) of Group B versus 2 (8%) in Group A (P < 0.05). Bradycardia was also more frequent in Group B6 (24%) compared to Group A1 (4%) (P < 0.05) (Table 6). These adverse events are consistent with the side-effect profile of EB, as noted in prior literature [8].
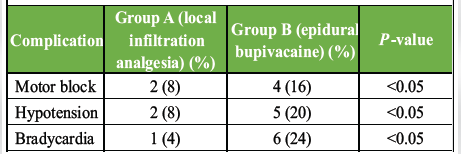
Table 6: Post-operative complications
These findings reinforce that local infiltration with ropivacaine-based multimodal analgesia is not only effective but also safer in the early post-operative period following TKA, supporting conclusions from other high-level studies [8,9,14].
Effective pain control following TKA remains one of the most critical factors influencing early rehabilitation, patient satisfaction, and overall outcomes. The findings of this study clearly demonstrate that LIA using a ropivacaine cocktail provides significantly better post-operative pain relief than EB, as evidenced by consistently lower VAS scores at all observed intervals, reduced need for rescue analgesia, fewer complications, and superior early functional recovery. The lower pain scores in the LIA group align with the results of previous randomised controlled trials and meta-analyses. Andersen and Kehlet conducted a systematic review that concluded LIA provides equivalent or superior analgesia compared to traditional techniques such as epidural or peripheral nerve blocks, especially in the first 48 h postoperatively [5]. Similarly, Kerr and Kohan, who originally popularised LIA, demonstrated that periarticular infiltration of local anaesthetics significantly reduces pain scores and facilitates early mobilisation following TKA [9]. Our study reinforces these findings, as patients in the LIA group had significantly lower VAS scores at 6, 12, 18, 24, and 48 h postoperatively. In terms of rescue analgesia requirements, only 32% of patients in the LIA group required additional analgesia compared to 84% in the epidural group. This difference is both statistically and clinically significant and consistent with prior literature. Xu et al., in a meta-analysis of 18 RCTs, concluded that single-dose periarticular infiltration significantly reduces opioid consumption and pain intensity within the early post-operative period [13]. Reduced opioid requirement also translates to fewer opioid-related side effects, improving overall patient comfort and safety. An important clinical outcome in this study was the difference in early ambulation and knee ROM. At 48 h postoperatively, 56% of patients in the LIA group were independently ambulatory versus only 28% in the epidural group. In addition, more patients in the LIA group achieved full knee ROM versus the epidural group. These results highlight the functional benefits of preserving motor function – a well-documented advantage of LIA over epidural or femoral nerve blocks [10]. In contrast, the epidural group experienced a higher rate of motor block (16%), which significantly delayed mobilisation, a drawback that has also been noted by Chelly et al. in comparative studies of regional analgesic techniques [8]. Furthermore, the incidence of hypotension in the epidural group (20%) compared to the LIA group (8%) underscores a critical safety concern associated with neuraxial techniques. EB causes sympathetic blockade, which can result in vasodilation and subsequent hypotension – especially in elderly or volume-depleted patients [7]. No such haemodynamic instability was observed in the LIA group, confirming the safety of local infiltration when used appropriately. The occurrence of bradycardia, which was significantly higher in the epidural group, is likely secondary to both systemic absorption of bupivacaine and increased opioid use for rescue analgesia. Lamplot et al. reported similar findings in their randomised study comparing LIA with PCA-based opioid regimens, where LIA patients had fewer side effects, higher satisfaction scores, and better functional outcomes [15]. The local infiltration technique used in this study included ropivacaine, ketorolac, adrenaline, and clonidine. Ropivacaine, a long-acting amide local anaesthetic, is known for its preferential sensory block over motor block and reduced cardiotoxicity compared to bupivacaine [11]. Ketorolac acts as an effective adjunct through COX inhibition, reducing inflammatory pain and opioid consumption [12]. Adrenaline prolongs the effect of local anaesthetics by causing vasoconstriction, whereas clonidine enhances the duration and depth of analgesia by acting on alpha-2 adrenergic receptors [18]. This multimodal approach not only enhances efficacy but also minimises systemic toxicity and side effects. Several studies have advocated for the use of such cocktails. Niemeläinen et al. demonstrated that a combination of levobupivacaine, ketorolac, and adrenaline reduced opioid usage and improved ROM in the immediate post-operative period, findings that parallel the results observed in our LIA group [14]. Although the specific anaesthetic agents varied slightly, the principle of multi-agent local infiltration remains the cornerstone of effective multimodal analgesia. Despite its strengths, our study is not without limitations. The sample size, while adequate to detect significant differences in pain and functional parameters, limits the generalisability of the findings. In addition, longer-term outcomes such as patient satisfaction at 3 or 6 months, incidence of chronic knee pain, and cost-effectiveness analysis were not assessed. Future multicentre trials with larger cohorts and extended follow-up could provide further validation. Nonetheless, the present study adds to the growing body of evidence supporting the use of LIA as a safe, effective, and easily administrable technique for postoperative analgesia in TKA. It allows for improved pain control, fewer systemic side effects, enhanced early mobility, and potentially shorter hospital stays. As current trends in arthroplasty move toward enhanced recovery after surgery (ERAS) protocols, the use of LIA aligns perfectly with these goals [19].
This prospective randomised study demonstrates that LIA with a ropivacaine-based multimodal cocktail is superior to postoperative EB in managing pain following primary TKA. LIA provided significantly lower pain scores, reduced the need for rescue analgesia, caused fewer complications (such as motor block and hypotension), and improved early functional outcomes such as ambulation and ROM. By avoiding the drawbacks of neuraxial techniques and enhancing analgesic efficacy through adjuncts such as ketorolac, adrenaline, and clonidine, LIA offers a safe, effective, and easily administered alternative. These findings support the integration of LIA into multimodal analgesia and ERAS protocols, promoting opioid-sparing, early rehabilitation, and improved patient satisfaction. Further large-scale studies are warranted to confirm its long-term benefits and cost-effectiveness.
Local infiltration analgesia with a ropivacaine-based cocktail represents a safe, effective, and practical alternative to epidural analgesia for postoperative pain management in primary total knee arthroplasty. Its use is associated with superior pain control, reduced reliance on additional analgesics, and a lower risk of systemic and neuraxial complications. By facilitating early mobilisation and improved functional recovery, LIA aligns well with enhanced recovery after surgery (ERAS) protocols and contributes to improved patient satisfaction. Given its ease of administration and favourable safety profile, LIA can be routinely incorporated into standard perioperative care protocols for TKA to achieve optimal clinical outcomes.
References
- 1. Ritter MA, Wing JT, Berend ME, Davis KE, Meding JB. The clinical effect of gender on outcome of total knee arthroplasty. J Arthroplasty 2008;23:331-6. [Google Scholar] [PubMed]
- 2. Apfelbaum JL, Chen C, Mehta SS, Gan TJ. Postoperative pain experience: Results from a national survey suggest postoperative pain continues to be undermanaged. Anesth Analg 2003;97:534-40. [Google Scholar] [PubMed]
- 3. Chavis TD. Pain and function after TKA: The patient’s perspective. J Arthroplasty 2007;22:23-25. [Google Scholar] [PubMed]
- 4. Joint Commission on Accreditation of Healthcare Organizations. Pain: The fifth vital sign. Joint Comm Perspect 2001;21:1-3. [Google Scholar] [PubMed]
- 5. Andersen LØ, Kehlet H. Analgesic efficacy of local infiltration analgesia in hip and knee arthroplasty: A systematic review. Br J Anaesth 2014;113:360-74. [Google Scholar] [PubMed]
- 6. Hawker GA, Badley EM, Borkhoff CM, Croxford R, Davis AM, Dunn S, et al. Which patients are most likely to benefit from total joint arthroplasty? Arthritis Rheum 2013;65:1243-52. [Google Scholar] [PubMed]
- 7. Sites BD, Brull R, Chan VW, Spence BC, Gallagher J, Beach ML, et al. Complications of neuraxial anesthesia. Int Anesthesiol Clin 2011;49:71-90. [Google Scholar] [PubMed]
- 8. Chelly JE, Greger J, Gebhard R, Coupe K, Clyburn TA, Buckle R, et al. Continuous femoral blocks improve recovery and outcome of patients undergoing total knee arthroplasty. J Arthroplasty 2001;16:436-45. [Google Scholar] [PubMed]
- 9. Kerr DR, Kohan L. Local infiltration analgesia: A technique for the control of acute postoperative pain following knee and hip surgery. Acta Orthop 2008;79:174-83. [Google Scholar] [PubMed]
- 10. Vendittoli PA, Makinen P, Drolet P, Lavigne M, Fallaha M, Guertin MC, et al. A multimodal analgesia protocol for total knee arthroplasty. A randomized, controlled study. J Arthroplasty 2006;21 6 Suppl 2:90-6. [Google Scholar] [PubMed]
- 11. McCartney CJ, Duggan E, Apatu E. Should we add clonidine to local anesthetic for peripheral nerve blockade? A meta-analysis of randomized controlled trials. Anesth Analg 2007;104:1570-7. [Google Scholar] [PubMed]
- 12. Andersen LJ, Poulsen T, Krogh B, Nielsen T. A randomized, double-blind study comparing ropivacaine with or without ketorolac and epinephrine for local infiltration analgesia after total knee arthroplasty. Br J Anaesth 2013;111:782-8. [Google Scholar] [PubMed]
- 13. Xu CP, Li XM, Zhang Q, Jiang Y, Zhang ZY, Zhan XL. Local infiltration analgesia for postoperative pain control in total knee arthroplasty: A systematic review and meta-analysis. Int J Surg 2016;29:210-7. [Google Scholar] [PubMed]
- 14. Niemeläinen M, Kalliovalkama J, Kariste A, Mäkelä K. Single-injection periarticular infiltration after total knee arthroplasty: A randomized, double-blind, placebo-controlled trial. Acta Orthop 2014;85:613-9. [Google Scholar] [PubMed]
- 15. Lamplot JD, Wagner ER, Manning DW. Multimodal pain management in total knee arthroplasty: A prospective randomized controlled trial. J Arthroplasty 2014;29:329-34. [Google Scholar] [PubMed]
- 16. World Medical Association. World medical association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013;310:2191-4. [Google Scholar] [PubMed]
- 17. Bromage PR. Epidural Analgesia. Philadelphia, PA: WB Saunders; 1978. [Google Scholar] [PubMed]
- 18. Elia N, Culebras X, Mazza C, Schiffer E, Tramer MR. Clonidine as an adjuvant to local anesthetics for peripheral nerve and plexus blocks: A meta-analysis of randomized trials. Anesthesiology 2008;109:280-94. [Google Scholar] [PubMed]
- 19. Khan SK, Malviya A, Muller SD, Carluke I, Partington PF, Emmerson KP, et al. Enhanced recovery programme for hip and knee replacement reduces death rate. Acta Orthop 2014;85:26-31. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 October 1, 2025 Comparative Evaluation of Multimodal Analgesia Techniques in Total Knee Arthroplasty: A Comparative Study
October 1, 2025 Comparative Evaluation of Multimodal Analgesia Techniques in Total Knee Arthroplasty: A Comparative Study August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report
August 1, 2026 The Boba Tea Sign: A Novel Magnetic Resonance Imaging Finding in Synovial Chondromatosis of the Knee – A Case Report August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty
August 1, 2026 Intrawound Vancomycin and Povidone-Iodine Treatment to Reduce Infection Rates in Arthroplasty July 1, 2026 Lipoma Arborescens of the Knee: An Intraoperative Mimicker of Pigmented Villonodular Synovitis in Bilateral Knee Osteoarthritis – A Case Report
July 1, 2026 Lipoma Arborescens of the Knee: An Intraoperative Mimicker of Pigmented Villonodular Synovitis in Bilateral Knee Osteoarthritis – A Case Report