
We described a novel technique for revision ACL reconstruction that is safe and provides good post-operative functional outcomes at short-term follow-up. With revision ACL reconstruction procedures on the rise, this is a safe technique that may assist with additional stability and can be considered in young active adults.
Dr. Taylor Manes, Department of Orthopedic Surgery, OhioHealth Doctors Hospital, Columbus, Ohio, USA. E-mail: taylormanes14@gmail.com
Abstract
Introduction: Revision anterior cruciate ligament (ACL) procedures are becoming more prevalent. Variable grafts for ACL reconstruction are available, including autograft, allograft, and synthetic graft options. Various augmentation techniques are also available and typically consist of synthetic material such as an Artelon graft. This type of synthetic material has been used and shown to produce safe and reliable augmentation in ligament injuries. The purpose of this study was to describe our unique revision ACL reconstruction technique utilising an Artelon graft augmentation and report our short-term results.
Materials and Methods: We retrospectively reviewed patients undergoing revision ACL reconstruction with an Artelon graft augmentation, a Flexband polyurethane-urea and polycaprolactone scaffold, to a tibialis anterior tendon allograft. We performed ACL reconstruction with an Artelon graft augmentation utilising the novel “ice cream sandwich” technique in both patients. Range of motion, return to activity, subjective pre- versus post-injury strength and stability, and Lysholm knee scores were evaluated with a 2-year follow-up.
Results: Two patients met the inclusion criteria with an average age of 25.5 years (22–29 years). A 24-month follow-up was obtained for both patients through a telephone encounter. Lysholm knee scores were recorded for each patient, with an average score of 86, demonstrating a good outcome 2 years postoperatively. No reoperations or complications, including infection, failed reconstruction, or neurovascular injury, were recorded for either patient.
Conclusion: We described a novel technique for revision ACL reconstruction that is safe and provides good post-operative functional outcomes at short-term follow-up. With revision ACL reconstruction procedures on the rise, this is a safe technique that may assist with additional stability around the graft and can be considered in young active adults.
Keywords: Artelon, anterior cruciate ligament, anterior cruciate ligament reconstruction, revision, allograft, autograft, graft failure, hypersensitivity reaction, biologic, scaffold.
Revision anterior cruciate ligament (ACL) reconstructions are becoming more prevalent, with approximately 13,000 cases performed in the United States each year (Grassi et al., 2017) [1]. Studies have shown that revision ACL reconstructions carry a risk of failure ranging from 2 to 5.4% (Grassi et al., 2017) [1]. Tibialis anterior tendon (TAT), quadriceps tendon, bone-patellar tendon-bone, and hamstring tendons are all graft options used in primary and revision ACL reconstruction. TAT is a commonly utilised allograft for revision, with a reported usage of 23% in multicentre cohort studies due to decreased donor site morbidity as seen with the harvest of autografts (Wright et al., 2010) [2]. However, allografts pose an increased risk for worse postoperative outcomes, function, and rupture compared to autografts (MARS group, 2014) [3]. Interestingly, prior studies have confirmed via knee arthroscopy that autografts fail significantly more near their femoral attachment (like the native ACL) compared to allografts (Magnussen et al., 2012) [4]. Of the autograft failures in the Magnussen et al. [4] study, midsubstance ruptures occurred in 10.5% of autografts and 32% of allografts (Magnussen et al., 2012) [4]. Therefore, allograft augmentation techniques to strengthen the midsubstance while preserving the overall healing potential are of particular interest (Looney et al., 2020) [5]. Scaffolds are favourable materials to support graft healing as they provide a matrix for cell migration and mimic the mechanical characteristics of native connective tissue (Takayama and Kuroda 2017) [6]. Specifically, synthetic materials may benefit revision allografts more than collagen derivatives in preventing midsubstance tear, as they have superior tensile strength while maintaining their bioconductive properties (Bellincampi et al., 1998) [7]. Polycaprolactone and polyurethane-urea copolymer (Artelon, Marietta, Georgia) have offered promising results as a safe bio-scaffold for augmentation in the knee and ankle (Kelly et al., 2021 [8]; Myers et al., 2022 [9]). In this article, we describe the “ice cream sandwich” technique to incorporate Artelon within a doubled TAT allograft through suture fixation in two young adult patients who underwent a revision ACL reconstruction.
This study did not require institutional review board approval since this was performed in two patients and was retrospective in nature. Verbal consent was obtained from both subjects to include their information and results for the design of the study.
Patient selection:
We conducted a retrospective review of two patients (ages 22 and 29 years old) who both underwent revision ACL reconstruction with Artelon scaffold augmentation after failing their primary ACL reconstruction procedures. Patients who underwent revision ACL reconstruction with Artelon scaffold augmentation were included in the study. The patients were followed for at least 2 years. Exclusion criteria included (1) revision ACL reconstruction without Artelon scaffold augmentation, (2) patients <18 years old, and (3) patients not undergoing a revision ACL reconstruction procedure. All surgeries were performed by a single, senior surgeon at a level 1 trauma centre. Both procedures were performed under general anaesthesia with the patient in the standard supine position. A circumferential leg holder was placed at the mid-thigh region with a tourniquet underneath. Both arthroscopic revision procedures were performed with TAT allograft, and Artelon Flexband 1.2 mm polycaprolactone and polyurethane-urea copolymer (Artelon, Marietta, Georgia) augmentation was performed in both cases as described in the surgical technique section below. The choice of graft was left up to the patient, and residual harvest pain was the reason for choosing an allograft option instead of harvesting an autograft. Nonetheless, this is a novel technique that has not yet been described in previous studies for its use in revision ACL reconstruction.
Two patients met the inclusion criteria with an average age of 25.5 years (patient 1: 22 years; patient 2: 29 years). A 24-month follow-up was obtained for both patients. Lysholm Knee Scores were recorded for each patient, and both reported a score of 86, demonstrating a good outcome 2 years postoperatively. No reoperations or complications, including infection, failed reconstruction, or neurovascular injury, were recorded for either patient. Return to full activity was achieved on average 7.5 months from the procedure (patient 1: 8 months; patient 2: 7 months). The level of activity before injury was similar in both patients (occasional, recreational athletes). Full knee range of motion (0–120°) was achieved at 8 months in patient 1 and 7 months in patient 2. Full strength (5/5) in knee flexion and extension was achieved in patient 1 at 8 months and 7 months in patient 2. At 24 months postoperatively, both patients admit their strength and stability are near 90% of their pre-injury level.
Technique overview:
Graft preparation with artelon scaffold:
Once an ACL tear was confirmed on pre-operative imaging, as shown in Figs. 1, 2, and 3, a revision ACL reconstruction utilising a TAT allograft with an Artelon bio-scaffold augmentation was performed.
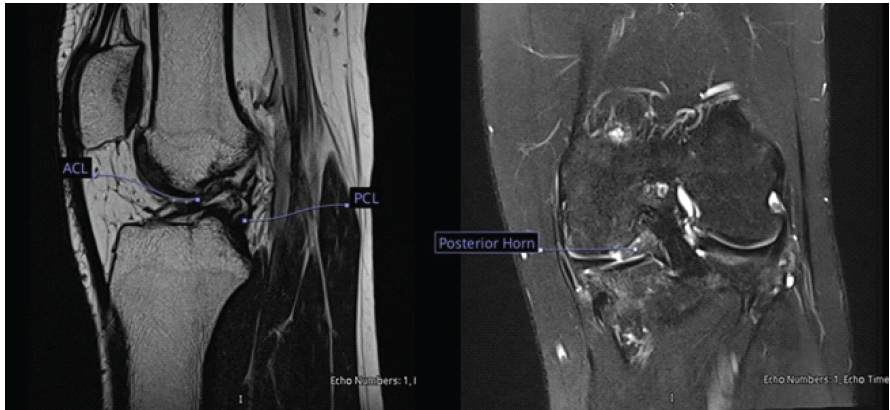
Figure 1: T2 sagittal magnetic resonance imaging (MRI) (left image) of the left knee demonstrates a complete tear in the anterior cruciate ligament with buckling of the posterior cruciate ligament. T2 coronal MRI (right image) of the left knee demonstrates a complex tear in the posterior horn of the medial meniscus as represented by the graphic detailing this structure.
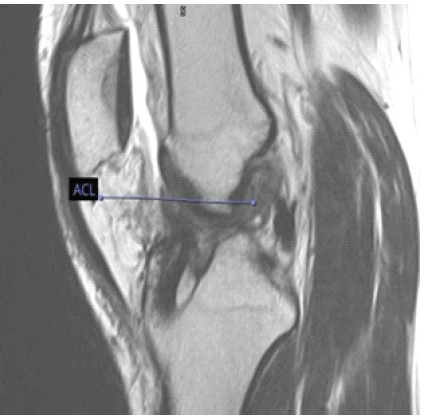
Figure 2: T2 sagittal magnetic resonance imaging of the left knee demonstrating post-surgical changes following anterior cruciate ligament (ACL) reconstruction. There is a complete midsubstance ACL tear noted in this image and represented by the graphic detailing this structure.
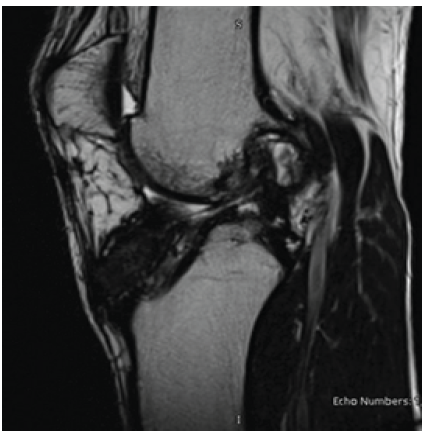
Figure 3: A T2 sagittal anterior cruciate ligament (ACL) warp magnetic resonance imaging view demonstrating a complete rupture of the ACL graft with the posterior cruciate ligament still intact.
First, a freeze-dried TAT allograft was thawed on the sterile field and prepared through standard technique. A 1.2 mm Artelon Flexband polyurethane-urea and polycaprolactone graft was introduced between the folds while doubling over the graft (Fig. 4).

Figure 4: This image shows the Artelon graft (grasped by the instrument) before securing it via suture to the tibialis anterior tendon allograft.
Monofilament absorbable suture was then used to secure the doubled ends of the graft and to interlock the Artelon Flex band within the stitching of the TAT allograft in a running fashion, best described as an “ice cream sandwich” (Fig. 5). The graft was next covered and kept damp with sterile saline solution until final passage.
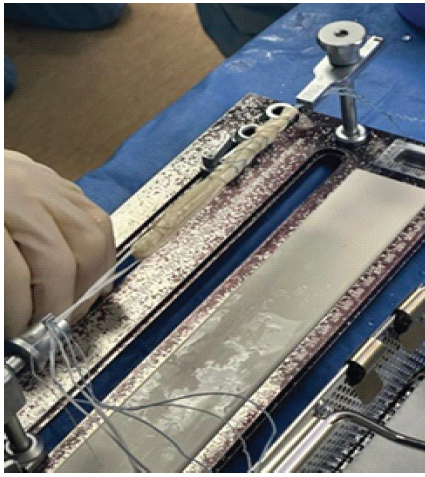
Figure 5: This image demonstrates the final product with the Artelon graft successfully secured to the tibialis anterior tendon allograft.
Diagnostic arthroscopy and debridement:
The knee was prepped and draped in a sterile fashion. Standard anterolateral and anteromedial arthroscopic portals were created, and diagnostic arthroscopy was performed to confirm an ACL mid-substance rupture in both cases. All three compartments were evaluated for chondromalacia. Next, both menisci were evaluated for any tears. The ACL stump, intercondylar notch, and femoral footprint of the ACL were then debrided with an arthroscopic shaver.
Tunnel preparation, graft passage, and fixation:
In our cases, a flip cutter for the femur (25 mm tunnel length) and a standard transtibial reamer with an anteromedial guide were used for the tibia based upon the size of the graft (between 8 and 9 mm). The tibial tunnel was placed according to intraoperative sizing of the graft, which may increase due to incorporation of the Artelon scaffold. The tunnels were shaved to remove debris and smooth the edges for easier passage. The TAT allograft with Artelon augmentation was then passed while the button was flipped on the femur. The knee was then cycled with tension applied to the ligaments and Artelon scaffold concurrently. Finally, a retrograde tibial tunnel interference screw was placed in standard fashion.
Closure and post-operative protocol:
Incisions were irrigated with sterile saline and closed with 3-0 nylon after a local anaesthetic injection was administered. Postoperatively, the patients were allowed to weight-bear right away in a hinged knee brace, limiting motion from 0 to 30° of knee flexion for the first 2 weeks and progressively working up to a full range of motion by 6 weeks. Both patients received routine follow-ups for 24 months to monitor for recurrent knee instability, hypersensitivity, and graft failure. At 24 months postoperatively, the patients admitted they were back to approximately 85% of their pre-injury strength and pain-free in their injured knees. They both demonstrated a full range of motion and a return to the pre-injury level of activity with the ability to run brace-free again without signs of pain or instability, even during quick-cutting movements. Lysholm knee scores were obtained during a telephone encounter at 2 years postoperatively, which resulted in a score of 86 for both patients, demonstrating good postoperative functional outcomes. No reoperations or complications were noted in either patient following the revision procedure, and both noted significant satisfaction with the ability to play recreational sports again, like their pre-injury level.
Rates of revision vary widely in the literature, as there are many techniques for ACL reconstruction; however, graft failure remains a major concern among surgeons. Therefore, studies aimed at graft augmentation in revision cases have become a point of focus in the literature. In our study, we sewed the Artelon graft between the folded TAT allograft (Figs. 4 and 5) to help resist rotational forces, since this has been a reported risk contributing to revision failure (Looney et al., 2020) [5]. Methods to decrease graft strain without introducing an impairment to healing are crucial in revision ACL reconstruction to improve graft healing and reduce the rate of re-rupture. Artelon, a FlexBand polycaprolactone and polyurethane-urea copolymer, is a suitable material to combine with a TAT allograft, as it provides a biocompatible matrix to support healing and increases the graft’s tensile strength and resistance to rotational forces, mimicking a native ligament (Looney et al., 2020) [5]. Similar reported applications of Artelon for tendon and ligament reconstruction suggest it is reasonable for application in ACL allograft scaffolding. Previous case series utilizing Artelon demonstrated non-inferior results compared to primary repair in collateral ligament injuries associated with knee dislocations in a series of 32 patients (Myers et al., 2022) [9]. Comparative studies of Artelon augmentation for patellar tendon repairs in dogs noted improved earlier range of motion, less post-operative pain, and improved strength when compared to animals treated with tendon repair alone (Gersoff et al., 2019) [10]. Larger sample studies with comparative results to non-augmented ligamentous repair and reconstruction are necessary to validate Artelon’s clinical effectiveness. In comparison, the suture tape internal brace mechanism is an increasingly popular technique to limit stress on ACL grafts at different working lengths and knee positions (Wilson et al., 2022) [11]. The suture tape is independently tensioned through a button or interference screw to create a “seatbelt” before the graft is stressed (Wilson et al., 2022) [11]. However, biomechanical stimulation is necessary to support mesenchymal cell migration and fibroblast differentiation (Bellincampi et al., 1998) [7]. The process of ligamentization is well-established to begin with an initial period of weakening due to strain as the extracellular matrix is remodeled (Sanchez et al., 2010) [12]. Scaffolds, such as Artelon, mimic the stress-strain curve and material architecture of ligaments (Panas-Perez et al., 2013) [13]. The isometric working length of the graft and the scaffold is the same when tensioned concurrently, eliminating stress shielding that ultimately reduces healing (Moreau et al., 2008) [14]. We propose that scaffolds provide a better supportive construct for an ACL allograft in revision procedures due to the concern of biological healing, which is not supported by internal braces. Potential concerns regarding Artelon use for soft-tissue reconstruction include adverse foreign body reactions and graft failure. In foot and ankle surgery, a retrospective review found no foreign body reactions to Artelon graft with soft-tissue reconstruction (MARS group, 2014) [3]. Other minor complications reported were cellulitis (5.5%) and delayed wound healing (9.1%) (Kelly et al., 2021) [8]. A case series of three patients reported a foreign body reaction confirmed with pathohistology after Artelon implantation for carpometacarpal interposition arthroplasty (Robinson et al., 2011) [15]. In cases where non-human tissue is used as a graft or for augmentation, foreign body reactions are always a possibility. Studies with higher levels of evidence are warranted to investigate the incidence of these reactions and the true safety profile of Artelon. Other limitations, specifically in the validity of this technique, include a small, reported sample size of only two patients with short-term follow-up data. A higher level of evidence and support would be achieved with a larger sample size and long-term follow-up data to further describe suture patterns for incorporating the Artelon during revision ACL reconstruction. The literature would benefit from additional prospective studies comparing different types of allograft and autograft options with Artelon augmentation. It would also be beneficial to explore other bio-scaffold materials to assist with graft fixation in revision ACL reconstruction.
There is a paucity of literature regarding Artelon augmentation in ACL reconstruction. This was a unique description of the “ice cream sandwich” technique for Artelon incorporation into a TAT allograft during revision ACL reconstruction. Successful results utilising this technique were demonstrated in both patients 24 months postoperatively. Increased case volume and follow-up duration are necessary to further evaluate the longevity and safety of this technique with the incorporation of the Artelon scaffold.
With revision ACL reconstruction procedures on the rise, we describe a novel technique that may assist with additional stability and can be considered in young active adults.
References
- 1. Grassi A, Kim C, Marcheggiani Muccioli GM, Zaffagnini S, Amendola A. What is the mid-term failure rate of revision ACL reconstruction? A systematic review. Clin Orthop Relat Res 2017;475:2484-99. [Google Scholar] [PubMed]
- 2. Wright RW, Huston LJ, Spindler KP, Dunn WR, Haas AK, Allen CR, et al. Descriptive epidemiology of the Multicenter ACL Revision Study (MARS) cohort. Am J Sports Med 2010;38:1979-86. [Google Scholar] [PubMed]
- 3. MARS Group. Effect of graft choice on the outcome of revision anterior cruciate ligament reconstruction in the multicenter ACL revision study (MARS) Cohort. Am J Sports Med 2014;42:2301-10. [Google Scholar] [PubMed]
- 4. Magnussen RA, Taylor DC, Toth AP, Garrett WE. ACL graft failure location differs between allografts and autografts. Sports Med Arthrosc Rehabil Ther Technol 2012;4:22. [Google Scholar] [PubMed]
- 5. Looney AM, Leider JD, Horn AR, Bodendorfer BM. Bioaugmentation in the surgical treatment of anterior cruciate ligament injuries: A review of current concepts and emerging techniques. SAGE Open Med 2020;8:2050312120921057 . [Google Scholar] [PubMed]
- 6. Takayama K, Kuroda R. Biological augmentation of anterior cruciate ligament grafts. Oper Techn Orthop 2017;27:33-7. [Google Scholar] [PubMed]
- 7. Bellincampi LD, Closkey RF, Prasad R, Zawadsky JP, Dunn MG. Viability of fibroblast-seeded ligament analogs after autogenous implantation. J Orthop Res 1998;16:414-20. [Google Scholar] [PubMed]
- 8. Kelly MJ, Dean DM, Hussaini SH, Neufeld SK, Cuttica DJ. Safety profile of synthetic elastic degradable matrix for soft tissue reconstruction in foot & ankle surgery. Foot Ankle Spec 2024;17:201-7. [Google Scholar] [PubMed]
- 9. Myers DM, Hyland S, Paulini A, Melaragno A, Passias BJ, Taylor BC. Artelon as a bio-scaffold to augment collateral ligament repair after knee dislocation. Malays Orthop J 2022;16:110-8. [Google Scholar] [PubMed]
- 10. Gersoff WK, Bozynski CC, Cook CR, Pfeiffer FM, Kuroki K, Cook JL. Evaluation of a novel degradable synthetic biomaterial patch for augmentation of tendon healing in a large animal model. J Knee Surg 2019;32:434-40. [Google Scholar] [PubMed]
- 11. Wilson WT, Hopper GP, Banger MS, Blyth MJG, Riches PE, MacKay GM. Anterior cruciate ligament repair with internal brace augmentation: A systematic review. Knee 2022;35:192-200. [Google Scholar] [PubMed]
- 12. Sanchez M, Anitua E, Azofra J, Prado R, Muruzabal F, Andia I. Ligamentization of tendon grafts treated with an endogenous preparation rich in growth factors: Gross morphology and histology. Arthroscopy 2010;26:470-80. [Google Scholar] [PubMed]
- 13. Panas-Perez E, Gatt CJ, Dunn MG. Development of a silk and collagen fiber scaffold for anterior cruciate ligament reconstruction. J Mater Sci Mater Med 2013;24:257-65. [Google Scholar] [PubMed]
- 14. Moreau JE, Bramono DS, Horan RL, Kaplan DL, Altman GH. Sequential biochemical and mechanical stimulation in the development of tissue- engineered ligaments. Tissue Eng Part A 2008;14:1161-72. [Google Scholar] [PubMed]
- 15. Robinson PM, Muir LT. Foreign body reaction associated with Artelon: Report of three cases. J Hand Surg Am 2011;36:116-20. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 April 1, 2025 Ipsilateral Autologous Peroneus Longus and Bone Patellar Tendon Graft for Revision Anterior Cruciate Ligament Reconstruction Leads to Similar Functional Outcome
April 1, 2025 Ipsilateral Autologous Peroneus Longus and Bone Patellar Tendon Graft for Revision Anterior Cruciate Ligament Reconstruction Leads to Similar Functional Outcome July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study
July 1, 2026 Clinical and Donor-site Outcomes of Full-thickness Peroneus Longus Autograft in Arthroscopic Anterior Cruciate Ligament Reconstruction: A Prospective Indian Cohort Study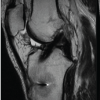 May 1, 2026 Anterior Cruciate Ligament Reconstruction Using Tibial Attachment – Preserving Hamstring Grafts: Early Clinical and Magnetic Resonance Imaging Assessment of Graft Ligamentization
May 1, 2026 Anterior Cruciate Ligament Reconstruction Using Tibial Attachment – Preserving Hamstring Grafts: Early Clinical and Magnetic Resonance Imaging Assessment of Graft Ligamentization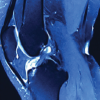 August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain
August 1, 2026 Intra-articular Ganglionic Cysts of Knee: A Cause for Anterior Knee Pain