
Early total hip arthroplasty leads to significant improvement in pain relief and functional outcomes, with maximal recovery achieved within 6–12 months, especially when intervention is performed at an earlier stage of disease.
Dr. S Venkatesh Kumar, Department of Orthopaedics, Saveetha Institute of Medical and Technical Sciences, Saveetha Medical College, Chennai, Tamil Nadu, India. E-mail: mailvenkatesh91@gmail.com
Abstract
Introduction: Total hip arthroplasty (THA) is a well-established surgical procedure for relieving pain and improving function in patients with advanced hip disorders. Functional outcomes can be effectively assessed using validated tools such as the modified Harris hip score (MHHS) and Oxford hip score (OHS). The aim of the study is to evaluate the functional outcomes of THA using MHHS and OHS and to assess post-operative recovery over a 12-month follow-up period.
Materials and Methods: This prospective study included 50 patients aged 45–70 years undergoing THA. Pre-operative and post-operative functional status was assessed using MHHS and OHS at 6 weeks, 3 months, 6 months, and 12 months. Statistical analysis was performed using paired t-tests and analysis of variance, with significance set at P < 0.05.
Results: The mean MHHS improved significantly from 61.2 ± 8.5 preoperatively to 88.6 ± 5.1 at 12 months (P < 0.001). Early improvement at 6 weeks was significant (P < 0.05), with highly significant gains thereafter. At final follow-up, 60% of patients had excellent outcomes, 33.3% good, and 6.7% fair (P < 0.001). The OHS improved from 21.4 ± 6.8 to 43.6 ± 4.3, with insignificant improvement at 6 weeks (P > 0.05) but highly significant improvement at later intervals (P < 0.001). Complications were minimal, with 80% of patients having no complications.
Conclusion: THA results in significant improvement in pain, function, and quality of life. Early improvement is detected by MHHS, while OHS reflects sustained functional recovery. Early surgical intervention is associated with better outcomes.
Keywords: Total hip arthroplasty, modified Harris hip score, Oxford hip score, functional outcome, hip replacement, prospective study, osteoarthritis, avascular necrosis.
Total hip arthroplasty (THA) is widely regarded as one of the most effective orthopaedic procedures for alleviating pain and restoring function in patients with advanced hip conditions such as osteoarthritis, avascular necrosis, and post-traumatic arthritis. Recent advancements in implant materials, including highly cross-linked polyethylene and ceramic components, along with minimally invasive techniques and innovations like robotic-assisted navigation, have markedly enhanced surgical precision, implant durability, and post-operative outcomes. In addition, improved perioperative care – such as early mobilisation, multimodal analgesia, and comprehensive patient education – has contributed to better recovery, higher patient satisfaction, and improved quality of life [1]. The modified Harris hip score (MHHS) is a well-established and reliable tool for evaluating hip function and clinical outcomes following arthroplasty. It has been shown to be valid, consistent, and sensitive to clinical changes across diverse patient populations [2]. Its standardised approach to assessing both pre-operative status and post-operative recovery facilitates meaningful comparisons across studies and clinical settings [3]. With the increasing prevalence of degenerative hip disorders driven by ageing, metabolic conditions, and changing lifestyles, the demand for THA in India continues to rise. However, disparities in socioeconomic status can affect access to timely surgery and the choice of implants. Previous research in India has highlighted that disease aetiology, socioeconomic factors, and baseline functional status significantly influence postoperative outcomes [4]. Therefore, this study aims to prospectively assess the functional outcomes of THA, focusing on improvements in mobility, pain relief, and overall quality of life, with the goal of optimising surgical planning, rehabilitation strategies, and healthcare policies for this population.
This hospital-based prospective study was conducted for 2 years at Vinayaka Missions Kirupananda Variyar Medical College’s Department of Orthopaedics in Salem, Tamil Nadu, India.
Study population:
50 individuals with hip pathology, aged 45–70, were enrolled using a consecutive sampling method.
Study design:
This is a hospital-based prospective study.
Inclusion and exclusion criteria:
Patients who were eligible for total hip replacement and had hip discomfort, instability, osteoarthritis, or avascular necrosis met the inclusion criteria. Patients with inflammatory hip diseases, neoplasms, significant vascular dysfunction, or current infections were not eligible.
Ethical consideration:
The institutional ethics committee provided ethical approval. All participants provided informed consent, and patient privacy was maintained at all times.
Data collection:
To confirm the diagnosis and assess joint health, all 50 patients underwent a full pre-operative evaluation that included a medical history, physical examination, and relevant imaging modalities (X-ray, magnetic resonance imaging, and computed tomography scans). The MHHS, which ranges from 0 to 100 and measures pain, functional capacity, range of motion, and deformity, was used to establish functional status. Higher levels imply better hip function. The patients’ function was classified into four categories: poor (<70), fair (70–79), good (80–89), and excellent (90–100) [2]. The Oxford hip score (OHS) was also calculated in all the patients. The patients were treated with the usual THA surgical procedure by expert orthopaedic surgeons. To monitor clinical and radiological outcomes, post-operative follow-up consultations were scheduled at 6 weeks, 3 months, 6 months, and 12 months. Repeated MHHS evaluations were utilised to monitor functional recovery, while radiography was used to assess implant location and stability.
Outcome measures:
The primary outcome measures in this study were functional and clinical improvements following THA, assessed using standardised scoring systems:
- MHHS: Used as the principal outcome measure to evaluate hip function. It assesses pain, functional capacity, range of motion, and absence of deformity, with scores ranging from 0 to 100. Higher scores indicate better hip function and are categorised as poor (<70), fair (70–79), good (80–89), and excellent (90–100).
- OHS: A patient-reported outcome measure used to assess pain and functional ability in daily activities. It reflects the patient’s perception of recovery and quality of life following surgery.
- Temporal assessment: Both MHHS and OHS were recorded preoperatively and at 6 weeks, 3 months, 6 months, and 12 months postoperatively to evaluate the progression of recovery over time.
- Complication profile: Post-operative complications such as infection, implant loosening, heterotopic ossification, and deep vein thrombosis/pulmonary embolism (DVT/PE) were documented to assess the safety of the procedure.
- Correlation analysis: The relationship between duration of symptoms and functional improvement (MHHS) was analysed to determine the impact of timing of surgery on outcomes.
Statistical analysis:
The data were analysed using the Statistical Package for the Social Sciences software. Clinical and demographic characteristics were summarised using descriptive statistics. Pre- and post-operative outcomes were compared using paired t-tests and analysis of variance, and the relationship between recovery and symptom duration was investigated using correlation analysis. Statistical significance was considered as a P < 0.05.
The study included 50 patients, with an average age of 56.2 ± 6.8 years. The plurality (26.7%) was between the ages of 51 and 55, with the age range spanning 45–70. The group consisted of 40% females and 60% males. The most prevalent diagnosis was osteoarthritis (73.3%), followed by avascular necrosis (26.7%).
Comparison of mean pre-operative and post-operative MHHS scores:
The pain scores improved by 78.2%, from 28.4 ± 6.2 before surgery to 6.2 ± 3.7 after a year. During the same time span, functional scores increased from 25.6 ± 7.5 to 46.7 ± 5.2 (P < 0.001). Range of motion ratings improved by 98.8% (from 2.1 ± 1.2 to 4.3 ± 0.7). The absence of deformities score increased from 1.9 ± 0.9 before surgery to 3.8 ± 0.4 after (Table 1). The mean MHHS gradually increased from 61.2 ± 8.5 before surgery to 88.6 ± 5.1 after 12 months (P < 0.001) (Table 2).
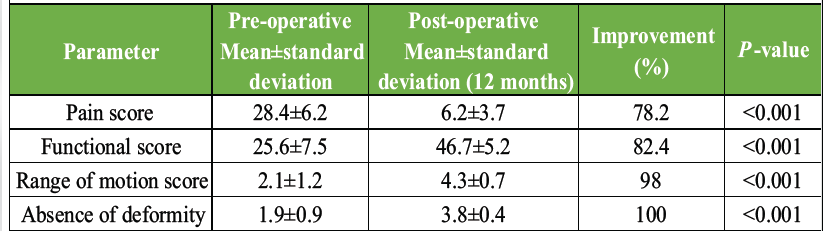
Table 1: Comparison of mean pre-operative and post-operative modified Harris hip score
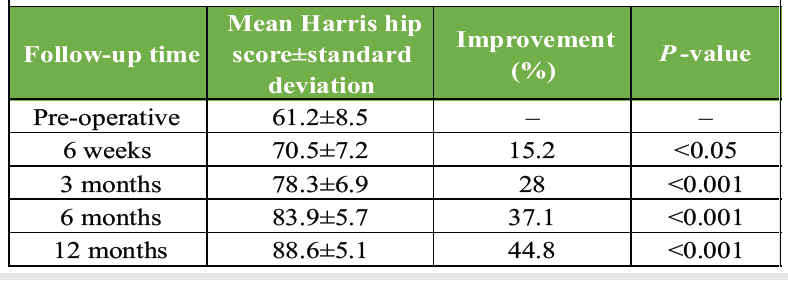
Table 2: Mean modified Harris hip core during follow-up among study participants
Mean MHHS score during follow-up:
The Harris hip score (HHS) improved progressively from 61.2 ± 8.5 preoperatively to 88.6 ± 5.1 at 12 months. Early improvement at 6 weeks was significant (P < 0.05), while gains at 3, 6, and 12 months were highly significant (P < 0.001), indicating sustained post-operative functional recovery (Fig. 1).
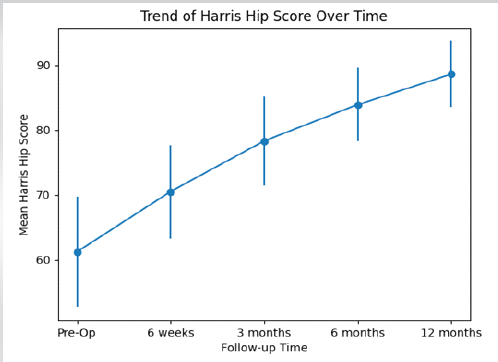
Figure 1: Mean modified Harris hip score during follow-up among study participants.
Comparison of pre-operative and post-operative MHHS categories:
At the final follow-up, 33.3% of patients had good results, 6.7% had fair results, and 60% had excellent results (90–100). Thus, there was a statistically significant (P < 0.001) improvement found after 1 year of surgery (Table 3 and Fig. 2).
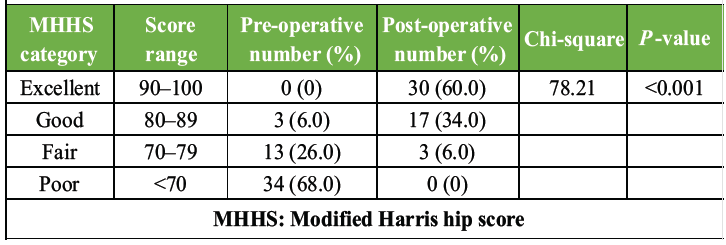
Table 3: Comparison of pre-operative and post-operative MHHS category
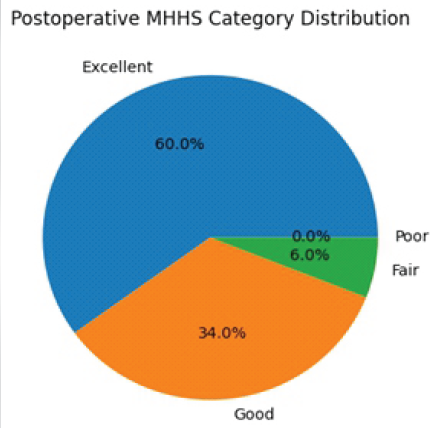
Figure 2: Post-operative modified Harris hip score.
OHS progression over time:
The OHS improved from 21.4 ± 6.8 preoperatively to 43.6 ± 4.3 at 12 months. Improvement at 6 weeks was not statistically significant (P > 0.05), whereas changes at 3, 6, and 12 months were highly significant (P < 0.001), indicating substantial and sustained functional recovery over time (Table 4 and Fig. 3).
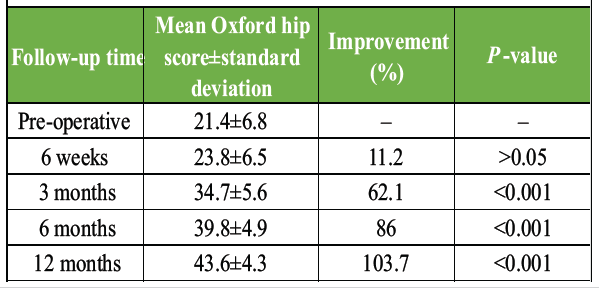
Table 4: Oxford hip score progression over time
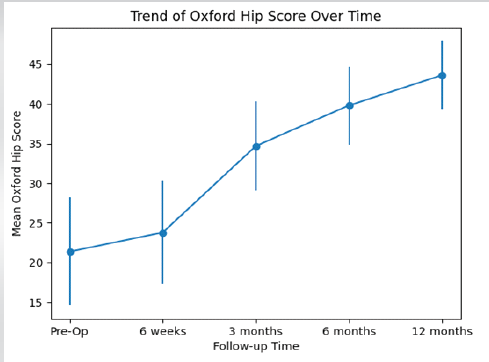
Figure 3: Oxford hip score progression over time.
Distribution of complications among study participants:
Among the 50 patients, 80.0% had no complications. The most common complications were infection and DVT/PE (each 6.0%), followed by implant loosening and heterotopic ossification (each 4.0%). Overall, the complication rate was low (Table 5).
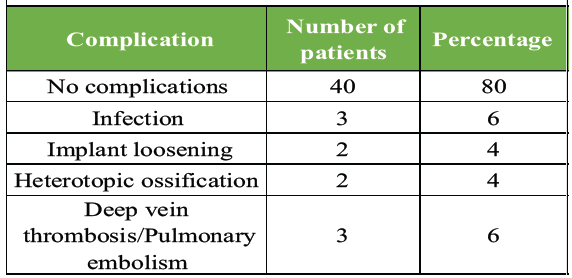
Table 5: Distribution of complications among study participants (n=30)
Correlation of mean MHHS score and duration of symptoms:
The improvement in MHHS decreased with increasing duration of symptoms. Patients with symptoms <12 months showed the highest improvement (30.1 ± 5.8) with strong correlation (r = 0.72, P < 0.001), while those with longer durations (>24 months) had comparatively lower improvement (24.8 ± 7.1) with moderate correlation (r = 0.62, P = 0.002). Overall, earlier intervention was associated with better functional outcomes (Table 6).
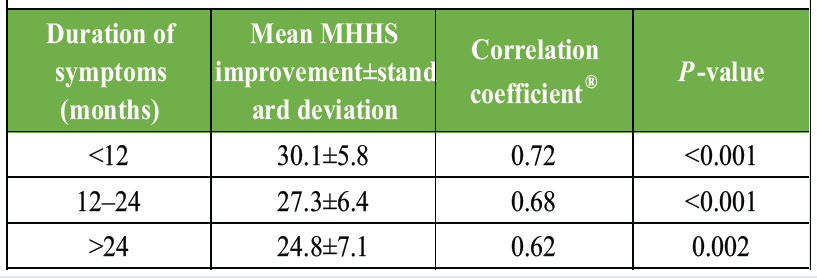
Table 6: Correlation of mean MHHS score and duration of symptoms
This prospective study demonstrated that patients with advanced hip pathology experience substantial benefits from THA, including significant pain relief, improved functional mobility, enhanced range of motion, and correction of deformities. The demographic profile of the study population, with a mean age of 56.2 years and a predominance of osteoarthritis (73.3%), aligns with global trends reported by the World Health Organization, which indicate that most individuals affected by osteoarthritis are older than 55 years [5]. The observed male predominance (60%) is consistent with findings by Ripoll-Romero et al. [6], attributing this to higher occupational strain and lifestyle-related risk factors such as alcohol consumption and smoking. Conversely, studies like those by Keen et al. [7] highlight the considerable burden of hip disorders among women, particularly in relation to postmenopausal osteoporosis, underscoring the need for gender-specific management strategies. The mean pre-operative MHHS of 61.2 in our study indicates moderate to severe functional impairment, comparable to previously reported data. Harold et al. [8] documented post-operative MHHS values exceeding 85 in well-managed THA patients, which is similar to the improvement observed in our cohort, where the score increased to 88.6 at 12 months. The results of this study are consistent with existing literature demonstrating marked functional improvement following THA. In our study, the HHS improved from 61.2 to 88.6, with early significant gains and sustained improvement over 12 months. Comparable findings were reported by Pandian et al. [9], who observed an increase in HHS from 38 preoperatively to 84 postoperatively, with the majority of patients achieving good to excellent outcomes – similar to the 93.3% good-to-excellent results in the present study. Likewise, Lakhotia and Agrawal [10] reported a significant rise in modified HHS from 13.28 to 88.52 (P < 0.001), with 80% of patients achieving favourable outcomes, further supporting our findings. Regarding recovery trends, our study showed that HHS improved significantly as early as 6 weeks, whereas improvements in the OHS were not significant at 6 weeks but became highly significant from 3 months onwards. This pattern is consistent with previous research indicating that functional recovery after arthroplasty is gradual, with significant improvements typically observed at 3 and 6 months and continuing thereafter [11]. Radiological evaluation in our cohort demonstrated a 97% implant stability rate at 1 year, reflecting the effectiveness of modern implant materials and surgical techniques. Similar implant survival rates exceeding 95% have been reported by Junnila et al. [12], emphasising the durability of current prosthetic designs and fixation methods. Furthermore, the low rate of implant malalignment observed in our study is in agreement with the literature, highlighting improved component positioning through minimally invasive and navigation-assisted techniques. The complication rate of 8.8% in our study falls within acceptable limits, as reported by Mori et al. [13], where infection rates range from 1% to 7% and thromboembolic events from 3% to 6% with appropriate prophylaxis. These findings highlight the importance of early mobilisation and comprehensive perioperative care in minimising complications. A strong correlation was observed between shorter symptom duration and better functional outcomes (r = 0.72, P < 0.001), suggesting that earlier surgical intervention leads to improved recovery. This is supported by Holzapfel et al. [14], who reported poorer long-term outcomes with delayed surgery. Similarly, Hadeed et al. [15] emphasised the cost-effectiveness and enhanced quality of life associated with early intervention, while Swarup et al. [16] demonstrated that patients undergoing THA before severe deformity develop better implant survival and require fewer revision procedures.
THA provides significant improvement in pain relief, functional mobility, and overall quality of life in patients with advanced hip disorders. Both MHHS and OHS demonstrated substantial post-operative gains, with early improvement detected by HHS and sustained recovery reflected by OHS over time. The majority of patients achieved good to excellent outcomes with a low complication rate, confirming the safety and effectiveness of the procedure. Early surgical intervention was associated with better functional recovery, highlighting the importance of timely management in optimising outcomes.
Total hip arthroplasty is a safe and effective procedure that provides substantial improvement in mobility, pain, and quality of life; early diagnosis and timely surgical intervention are crucial for optimal functional outcomes and reduced complications.
References
- 1. Total Hip Arthroplasty Techniques. StatPearls. Available from: https://www.ncbi.nlm.nih.gov/books/nbk507864 [Last accessed on 2025 Oct 15]. [Google Scholar] [PubMed]
- 2. Vishwanathan K, Pathan SK, Makadia RC, Chaudhary CB. Psychometric assessment of modified Harris hip score for femoral neck fracture in Indian population. Indian J Orthop 2020;54 Suppl 1:87-100. [Google Scholar] [PubMed]
- 3. Berliner JL, Brodke DJ, Chan V, SooHoo NF, Bozic KJ. John Charnley award: Preoperative patient-reported outcome measures predict clinically meaningful improvement in function after tha. Clin Orthop Relat Res 2015;474:321-9. [Google Scholar] [PubMed]
- 4. Mittal G, Kulshrestha V, Kumar S, Datta B. Epidemiology of revision total hip arthroplasty: An Indian experience. Indian J Orthop 2020;54:608-15. [Google Scholar] [PubMed]
- 5. Osteoarthritis. Available from: https://www.who.int/news-room/fact-sheets/detail/osteoarthritis [Last accessed on 2025 Oct 15]. [Google Scholar] [PubMed]
- 6. Ripoll-Romero E, Agüera Z, Puig-Llobet M, Bassas M, Manzanares-Céspedes MC, Galimany-Masclans J. Gender differences in pre-surgical hip arthroplasty patients. Front Glob Womens Health 2025;6:1565899. [Google Scholar] [PubMed]
- 7. Keen MU, Barnett MJ, Anastasopoulou C. Osteoporosis in females. In: StatPearls. Treasure Island, FL: StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/nbk559156 [Last accessed on 2025 Oct 15]. [Google Scholar] [PubMed]
- 8. Harold RE, Butler BA, Delagrammaticas D, Sullivan R, Stover M, Manning DW. Patient-reported outcomes measurement information system correlates with modified harris hip score in total hip arthroplasty. Orthopedics 2021;44:e19-25. [Google Scholar] [PubMed]
- 9. Pandian PM, Vignesh KA, Thulasi Raman D. Analysis of functional outcome of total hip arthroplasty in lower socio economic people. Int J Orthop Sci 2019;5:260-7. [Google Scholar] [PubMed]
- 10. Lakhotia D, Agrawal U. Functional outcome of uncemented total hip replacement in low socioeconomic group using modified Harris hip score: A prospective midterm follow-up study. Cureus 2023;15:e50005. [Google Scholar] [PubMed]
- 11. Teimouri M, Salehi A, Shahsavan M, Rezaei H, Dayani Dardashti A. Effectiveness of total knee arthroplasty on pain reduction and functional improvement in elderly patients: A quasi-experimental study. Adv Biomed Res 2025;14:86. [Google Scholar] [PubMed]
- 12. Junnila M, Laaksonen I, Eskelinen A, Pulkkinen P, Ivar Havelin L, Furnes O, et al. Implant survival of the most common cemented total hip devices from the Nordic arthroplasty register association database. Acta Orthop 2016;87:546-3. [Google Scholar] [PubMed]
- 13. Mori Y, Tarasawa K, Tanaka H, Kamimura M, Harada K, Mori N, et al. Thromboembolic and infectious complication risks in TKA and UKA: Evidence from a Japanese nationwide cohort. Knee Surg Relat Res 2025;37:19. [Google Scholar] [PubMed]
- 14. Holzapfel DE, Meyer M, Thieme M, Pagano S, Von Kunow F, Weber M. Delay of total joint replacement is associated with a higher 90-day revision rate and increased postoperative complications. Arch Orthop Trauma Surg 2023;143:3957-64. [Google Scholar] [PubMed]
- 15. Hadeed GJ, Smith J, O’Keeffe T, Kulvatunyou N, Wynne JL, Joseph B, et al. Early surgical intervention and its impact on patients presenting with necrotizing soft tissue infections: A single academic center experience. J Emerg Trauma Shock 2016;9:22-7. [Google Scholar] [PubMed]
- 16. Swarup I, Lee YY, Christoph EI, Mandl LA, Goodman SM, Figgie MP. Implant survival and patient-reported outcomes after total hip arthroplasty in young patients with juvenile idiopathic arthritis. J Arthroplasty 2015;30:398-402. [Google Scholar] [PubMed]






Related Articles in Journal of Orthopaedic Case Reports
 July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach
July 1, 2026 A Comparative Study of Functional Outcome Following Total Hip Replacement by Posterolateral and Anterolateral Approach July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach
July 1, 2026 Managing Complications of Total Hip Arthroplasty for Avascular Necrosis Hip Performed Via Anterior Approach May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes
May 1, 2026 Direct Anterior THA with Leg Positioning Traction System for Avascular Necrosis: Technique and Early Outcomes March 1, 2026 Total Hip Arthroplasty in Lubumbashi (DR Congo), Outcomes in a Resource-Limited Setting
March 1, 2026 Total Hip Arthroplasty in Lubumbashi (DR Congo), Outcomes in a Resource-Limited Setting