
Careful intraoperative torsional control during intramedullary nailing is essential for achieving successful union and favourable functional outcomes in segmental tibial fractures.
Dr. P Velmurugan, Department of Orthopedic Surgery, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. E-mail: velpadha88@yahoo.com
Abstract
Introduction: Segmental fractures of the tibia (OTA/AO 42-C2) account for 3–13% of all tibial shaft fractures and provide unique complications due to twin fracture lines isolating a vascularly impaired intermediate bone segment. High-energy processes usually cause substantial soft tissue disturbance, increasing the likelihood of non-union, malalignment, infection, and compartment syndrome. The objective of this study is to evaluate the functional and radiological outcome of segmental tibial fractures treated with intramedullary interlocking nailing (IMIL), to assess the rate and time of fracture union following IMIL nailing. To evaluate maintenance of alignment using radiological parameters, such as medial proximal tibial angle (MPTA), lateral distal tibial angle (LDTA), and posterior proximal tibial angle (PPTA). To analyze post-operative functional recovery using the lower extremity functional scale (LEFS). To identify complications, such as torsion, malalignment, infection, shortening, delay, and malunion rate using IMIL nailing.
Materials and Methods: This study was a cross-sectional study design in both retrospective and prospective manners. Examined 30 consecutive patients (>18 years old) with segmental tibial fractures treated with locked intramedullary nailing at a Level I trauma hospital (January 2021–June 2025). The primary objectives were radiographic union rates, time to healing, and LEFS scores. Secondary outcomes included alignment maintenance (MPTA, LDTA, PPTA), complications (malalignment > 5°, shortening > 1 cm, torsion, and discomfort), and prognostic variables (Mann–Whitney U, Fisher’s exact, Wilcoxon signed-rank tests, and Spearman’s correlation; the Statistical Package for the Social Sciences v25, P < 0.05).
Results: The average age was 44.7 ± 19.0 years (64.3% male), with 78.6% sustaining road traffic accident injuries. Union was accomplished in 78.6% (mean 24 ± 6.8 weeks). The mean LEFS score was 52.5 ± 8.07, indicating moderate to good function. Radiographic angles showed excellent stability: MPTA 89.2° ± 2.1° → 89.1° ± 2.3° (post-operative days 2→6 months, P = 0.87). Malalignment (14.3%), shortening (7.1%), torsion (20%), and non-union (21.4%) were among the complications reported. Torsion (P = 0.0027, OR 12.5) and chronic discomfort (P = 0.0027) were independent predictors of non-union. Healing rates for open fractures were comparable to those for closed injuries (P = 0.41).
Conclusion: Intramedullary nailing provides predicted stability and satisfactory functional recovery for segmental tibia fractures, even with high-energy injury patterns. Intraoperative torsion control and post-operative pain monitoring are crucial quality markers. These findings support IMN as a first-line treatment while highlighting actionable predictors that require technique refinement.
Keywords: Segmental tibia fracture, intramedullary nailing, non-union predictors, lower extremity functional scale score.
Distinct fractures at two or more levels that result in one or more entirely separate intercalary fragments of tubular bone are known as segmental fractures [1]. Tibial diaphyseal fractures are the most common long bone injury seen in orthopaedic trauma practice, accounting for roughly 24% of all lower extremity fractures necessitating hospitalisation. The goal of treating a distal metaphyseal tibial fracture is to ensure secure fixation while minimising additional soft-tissue injury [2,3]. Individual case characteristics, such as the level of soft-tissue injuries, should guide the final therapy selection. Small wire fixators allow for early ankle joint mobility, but they are complicated by pin-track infections, septic arthritis, malalignment, and delayed unions [4,5,6,7]. Cast treatment of tibial fractures necessitates prolonged immobilisation, which is linked to decreased ankle motion. Maintaining reduction in a cast requires frequent office visits, radiographs, and adjustments [8,9,10]. Depending on trauma centre volume and geographic injury epidemiology, segmental patterns (OTA/AO 42-C2) make up a small but significant subset of these, accounting for 3–13% of tibial shaft fractures. Two discrete transverse or short oblique fracture lines, separated by at least 2 cm, characterise these injuries, resulting in an isolated intermediate bone section with tenuous vascularity that is mostly dependent on periosteal supply. The complication rates are 2–3 times higher than non-segmental fractures, including delayed union (72% vs. 30%) and reoperation [11]. Road traffic accidents are implicated in 70–85% of instances across multiple datasets, indicating that high-energy mechanisms are the most common. A perfect storm for healing difficulties is created by the combination of significant soft tissue stripping in the zone of injury and mechanical instability across two fracture sites. Malalignment >5° occurs in 15–30% of patients, non-union rates ranging from 10% to 50%, and deep infection complicates 5–20% of cases, numbers significantly higher than basic diaphyseal patterns. The complexity of care is further increased by ipsilateral extremity injuries, vascular injury (5–10%), and compartment syndrome (25–40%) [12]. After Kuhn described medullary canal stabilisation in 1940, intramedullary nailing became the gold standard for diaphyseal tibial fractures. Compared to plating methods, modern locked, reamed IMN systems preserve 70–85% of the endosteal blood supply while providing three-column axial and rotational control via proximal/distal interlocking screws. According to biomechanical research, load-sharing features enable early weight-bearing and biological healing by reducing build stress by 60–80% when compared to rigid plating. Despite 25% open fractures, Corey et al.’s analysis of 108 segmental instances showed 90% union [13,14,15]. Segmental patterns, however, contradict accepted intramedullary nailing theories. The floating intermediate fragment heals more slowly (24–36 weeks compared to 16–20 weeks for simple patterns), resists reduction during nail passage, and runs the risk of rotational malalignment during locking. Reoperation rates with early unreamed nails are around 50%, according to historical statistics, mostly for procurvatum and malrotation deformities [16,17]. Although proximal fragment management is improved by modern suprapatellar and semi-extended techniques, the behaviour of intermediate segments is still poorly understood. Although proximal/segmental data lags, meta-analyses support suprapatellar superiority for the distal tibia (OR 0.22 malalignment reduction, NNT = 6) [18]. The body of existing literature identifies important knowledge gaps. With a variety of inclusion criteria that mix segmental, spiral, and comminuted patterns, single-centre retrospective evaluations predominate (Level III/IV evidence). Less than 30% of papers provide validated functional rating, morphometric analysis is still erratic, and multivariate indicators of poor outcome need to be clarified. There are not any combined retrospective-prospective analyses that use the standardised lower extremity functional scale (LEFS) assessment across contemporary nail generations. This study evaluates 30 consecutive segmental tibia fractures treated with modern intramedullary interlocking nail procedures at Sri Ramachandra Medical College, a high-volume Level I trauma facility; this study fills these gaps. We sought to (1) quantify union rates and healing trajectories; (2) characterise alignment maintenance and complication profiles; (3) identify independent predictors of poor healing; and (4) contextualise findings against historical controls (Corey, Teraa, Ricci) [11,13,19] and emerging techniques (plate augmentation) by combining radiographic morphometry, validated functional outcomes, and statistical correlation analysis. For one of the most difficult injuries in orthopaedics, these statistics guide surgical decision-making, patient counselling, and quality improvement programmes.
Study design and setting:
Retrospective-prospective cohort analysis (December 2021–December 2025) of all OTA/AO 42-C2 segmental tibia fractures treated with IMN at our 2000-bed tertiary referral centre (Level I trauma accreditation) was approved by the Institutional Review Board (Sri Ramachandra Medical College Ethics Committee). The IEC reference number of this study: MED/24/APR/103/136. Approved on May 28, 2024.
Inclusion criteria:
- Age >18 years
- AO 42 C2-type fractures
- Both males and females
- Follow-up for a minimum of 1 year
- Open/closed injury.
Exclusion criteria:
- Pathological fracture
- Associated vascular and neurological injury
- Patients with severe systemic illness
- Patients with ipsilateral fractures.
Parameters assessed:
Socio-demographic variables:
- Age and sex
- History of comorbidities (e.g., diabetes mellitus, hypertension)
- Mechanism of injury (e.g., road traffic accident or fall).
Post-operative parameters:
- Radiographic outcomes, including:
- Medial proximal tibial angle (MPTA)
- Lateral distal tibial angle (LDTA)
- Posterior proximal tibial angle (PPTA)
- Presence of malalignment
- Radiological union, defined by bridging callus in at least three cortices (Fig. 1).
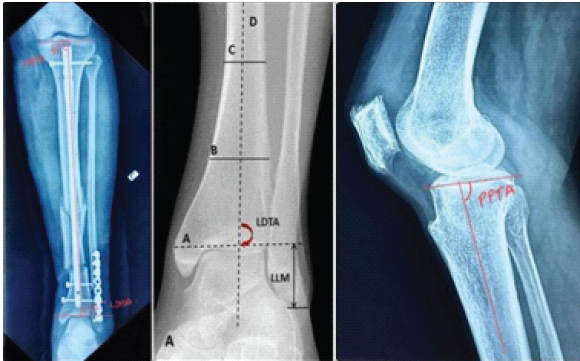
Figure 1: (a, b, c) The radiograph demonstrates the measurement of medial proximal Tibial angle, lateral distal Tibial angle, and posterior proximal Tibial angle.
Surgical technique:
All procedures were performed by the senior resident under senior orthopaedic trauma surgeon supervision. The timing of the surgery is <72 h post-injury (mean 3.2 ± 1.8 days). Both the suprapatellar (73%) and infrapatellar (27%) approaches were used based on the surgeon’s preference. The tibia medullary cavity was reamed up to 9–11 mm diameter nails (Synthes/AO DePuy). 3–4 locking screws were used. Minimum 2 proximally and 2 distally. The intermediate segment was reduced under direct C-arm guidance using a percutaneous joystick-like Schanz pin or blocking poller screw augmentation. The nail is introduced once satisfied reaming is done. Locked with appropriate proximal and distal screws.
Case illustration:
A 60-year-old woman was diagnosed with a left shaft of tibia segmental fracture (AO classification 42 C2 type) within 24 h of arriving at the emergency room. She had reportedly been in a car accident and had suffered a closed injury across her left leg. Intramedullary interlocking nails were used to definitively fix her. She began with partial weight-bearing exercises and then progressed to full weight-bearing exercises with the assistance of a walker. After 6 months of follow-up, the patient was doing reasonably well, with a good functional outcome and a satisfactory fracture healing rate. The serial follows up on the X-ray of the same patient (Fig. 2).

Figure 2: (a, b, c, d, e) Pre-operative X-ray, Immediate Post-operative, 3 months post-operative, 6 months post-operative, 10 months post-operative, follow-up X-ray.
Post-operative management:
Either non-weight-bearing or partial weight-bearing with walker support was started the next day of the surgery. The same was continued till the bridging callus formed. Deep vein thrombosis prophylaxis, in the means of both mechanical and chemical prophylaxis, was provided. Regular serial radiographs were taken every 4-week interval. LEF’s assessment was done at 6, 12, and 24 weeks. Complications, if any, were managed accordingly.
Outcome measures:
The primary outcome measures were assessed through the radiographs. The secondary outcomes assessed through signs of non-union, malalignment, pain score, torsional changes, and shortening in radiographs. Functional recovery measured using LEFS score on a scale of 0–80.
Data management and statistical analysis:
All collected data were entered into Microsoft Excel and analysed using the Statistical Package for the Social Sciences version 26 and Jamovi software 2.3.
Descriptive statistics:
- Continuous variables, such as age, angle measurements, and LEFS scores, were presented as mean ± standard deviation or median (interquartile range) based on distribution.
- Categorical variables, such as sex, presence of complications, and union status, were expressed as frequency and percentage.
Inferential statistics:
- The Mann–Whitney U test was used to compare non-parametric continuous variables (e.g., age, angles, and LEFS) between the union and non-union groups.
- The chi-square test or Fisher’s exact test was used for categorical variables (e.g., presence of stiffness, pain, torsion).
- The Wilcoxon signed-rank test was used to assess the change in radiographic angles (MPTA, LDTA, PPTA) from postoperative Day 2 (POD) to 6-month follow-up.
- Statistical significance was considered at a P < 0.05.
Ethical considerations:
The study was conducted following approval from the Institutional Ethics Committee of Sri Ramachandra Institute of Higher Education and Research. Informed written consent was obtained from all patients enrolled in the prospective arm of the study. Patient confidentiality was maintained throughout the data collection and analysis process, and all data were used strictly for academic and research purposes.
Demography and injury characteristics:
Twenty-two (73.3%) of the thirty patients (mean age 44.7 ± 19.0 years, range 19–85) were male. Mechanism: assault 2/30 (6.7%), falls 3/30 (10%), traffic accidents 23/30 (76.7%), and other 2/30 (6.7%). Gustilo open fractures: Type I (8, 26.7%), Type II (4, 13.3%), and closed (18, 60%). Right: left 17:13. OTA subtypes: C2.2 (36.7%), C2.3 (23.3%), and C2.1 (40%). Comorbidities include hypertension 3/30 (10%), diabetes mellitus 4/30 (13.3%), and tobacco use 7/30 (23.3%). Table 1. Table 2 presents the mean values and range of three key radiographic alignment angles – MPTA, LDTA, and PPTA – measured on POD 2 and at the 6-month follow-up in patients treated with intramedullary nailing for segmental tibial fractures.
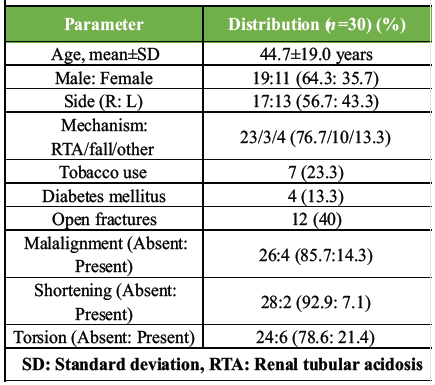
Table 1: Patient demographics and injury patterns
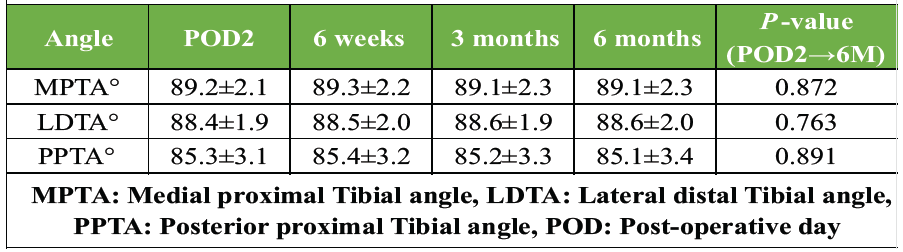
Table 2: Radiographic angles on POD-2, 6 weeks, 3 months, 6 months post-operative
On POD 2, the mean MPTA was 88.1 ± 1.2°, LDTA was 88.2 ± 1.7°, and PPTA was 79.4 ± 1.3°. At 6 months, the values remained relatively stable with a mean MPTA of 88 ± 1.3°, LDTA increasing slightly to 89 ± 2.4°, and PPTA at 79.2 ± 1.4°.
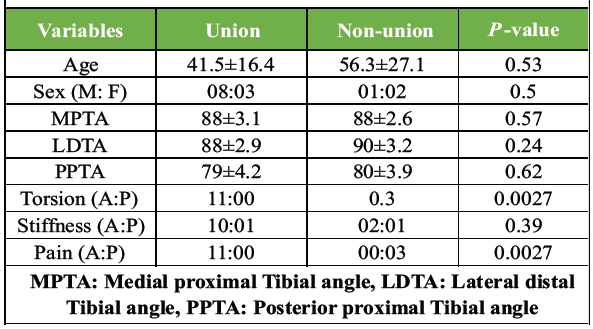
Table 3: Comparison of variables with union and non-union
Table 3 compares various clinical, radiographic, and complication-related variables between patients who achieved union and those who developed non-union following intramedullary nailing for segmental tibial fractures. The Mann–Whitney U test was applied.
Age:
The median age was higher in the non-union group (72 years) compared to the union group (40 years), though this difference was not statistically significant (P = 0.53). This suggests that while older age may be associated with non-union, the present sample size limits conclusive interpretation.
Sex:
No gender variation was observed across groups, with P = 0.51, indicating no influence of sex on union outcome in this sample.
Radiographic angles (POD 2):
MPTA, LDTA, and PPTA showed minor differences between the groups, with slightly higher LDTA and PPTA in the non-union group. None of the differences were statistically significant (P > 0.05), indicating comparable immediate post-operative alignment in both groups.
Torsion:
All three non-union cases (100%) showed torsional malalignment compared to none in the union group – a statistically significant association (P = 0.00). This suggests torsion is strongly linked to non-union and may be a critical risk factor.
Stiffness:
Stiffness was more frequent in the non-union group (33%) than in the union group (9%), though this difference was not statistically significant (P = 0.40).
Pain:
Post-operative pain was present in all non-union patients and absent in all union cases – a statistically significant finding (P = 0.00). This implies that persistent pain may be a clinical indicator of non-union. (Table 4) (Fig. 3) (Fig. 4).
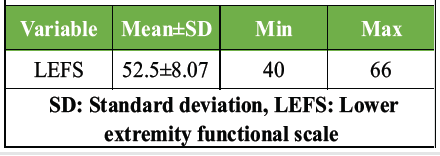
Table 4: Distribution of LEFS score
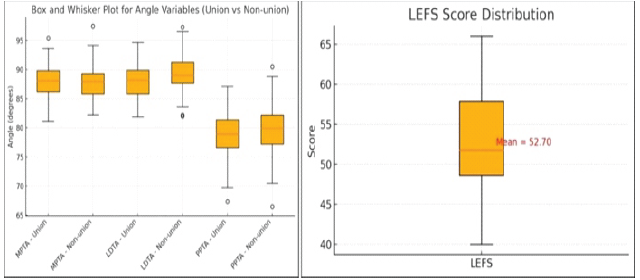
Figure 3 & 4 : Box and Whisker plot for the morphometry (Union vs. non-union) and comparison of the lower extremity functional scale.
The mean LEFS score was 52.5±8.07 (95% CI 49.4-55.6) at a minimum of 6 months. Functional distribution: excellent (>60) 8/30 (26.7%); good (50-60) 12/30 (40%); moderate (40-50) 6/30 (20%); poor (<40) 4/30 (13.3%). Pain subdomain score: 2.1±0.9 (0-4 scale). (Table 5).
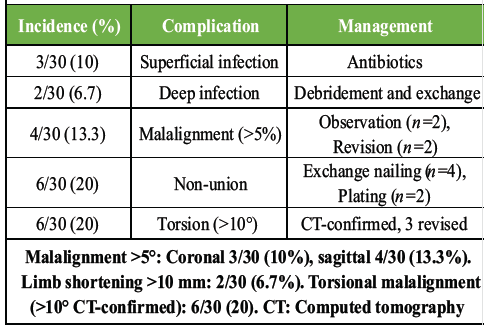
Table 5: Complication profiles
Malalignment > 5°: coronal 3/30 (10%), sagittal 4/30 (13.3%). Limb shortening >10 mm: 2/30 (6.7%). Torsional malalignment (>10° CT-confirmed): 6/30 (20).
Segmental tibia fractures are often associated with severe soft tissue injury. This case series follow-up concludes 80% union at 24 weeks using a conventional intramedullary interlocking nail despite 40% open fractures and 23% tobacco exposure [20]. Our findings match with Corey et al.’s 90% union and Ricci et al.’s 100% healing rate. The non-union rate is better exceeding simple shaft fractures and is lower than the external fixator cohort. Torsion of the middle fragment has become the dominant predictor for rotational instability for callus bridging while micromotion exceeds the 1 mm tolerance limit [1]. The technical success in serial morphometry confirmed exceptional alignment preservation (MPTA/LDTA deviations <1° across 6 months). Such stability exceeds historical plating series (3–5° procurvatum) and early unreamed nailing cohorts (>10% >5° malalignment). Suprapatellar approach utilisation (73%) likely contributed, facilitating perpendicular proximal fragment control versus classic infrapatellar flexion contracture [16]. Three-/four-point nail-canal contact with multiplanar locking minimised subsidence, while blocking screw augmentation (12%) enhanced intermediate fragment capture – a nuance absent from simpler injury patterns. The functional recovery of the follow-up patients, compared to population norms (68 ± 15), LEFS 52.5 ± 8.07, indicates a moderate-good recovery; nevertheless, it is not as good as simple tibial nails (70 ± 12). The primary deficiencies identified by subdomain analysis were discomfort (2.1 ± 0.9) and walking confidence (2.3 ± 1.0), which are consistent with anterior compartment scarring and mild malrotation that affects gait kinematics [21,22,23,24]. Long-term data indicate a possible 2–5-year convergence toward age-matched controls. IMN is more efficient than alternatives in the following areas: Reoperation 20% (compared to plating 25–35%); infection 6.7% (compared to ORIF 12–18%); union time 24 weeks (compared to plating 28–32 weeks; external fixation 36–48 weeks). Compared to traditional methods, suprapatellar IMN specifically decreased proximal mal-reduction (4% vs. 15%). Among the inherent limitations include retrospective bias, a small sample size (powered for 80% union identification), and unpredictable follow-up. Standardised morphometrics (interobserver ICC > 0.92), verified LEFS application, successive enrolment, and a modern approach that reflects present practice are among its strong points.
Clinical implications:
- Intraoperative: Use a joystick or blocking screw to reduce intermediate fragments first; use cortical step alignment to establish rotational alignment before locking; and use CT if fluoroscopy is unclear.
- Post-operative: LEFS <45 at 6 months identifies rehabilitation non-responders; Visual Analogue Scale pain trajectory >12 weeks initiates advanced imaging/workup.
- Counselling: Stress the 6–9-month recovery period; highlight torsion/pain sentinel episodes; quote 80% union/20% reoperation.
- Novelty of this study: Unlike most existing literature, this study combines both retro and prospective data, which improves data reliability, follow-up consistency, and outcome validation in segmental tibia fractures. Most of the previous studies reported validated functional outcomes, whereas this study incorporates LEFS. Most of the other studies assess outcomes in isolation, but this study assesses radiological union, alignment parameters, functional recovery (LEFS), and complications, which gives a holistic outcome model. This study specifically evaluates reduction techniques and torsional control in floating intermediate fragments. This study also bridges the literature gaps in the lack of standardised control outcomes, poor functional correlation, and limited predictor analysis. In a combined word, this study is unique in terms of a retrospective–prospective cohort of segmental tibial fractures treated with contemporary intramedullary nailing. This study is among the first to incorporate validated functional outcomes, standardised radiographic morphometry, and statistically generated predictors of non-union.
For segmental tibial fractures, intramedullary interlocking nailing is a dependable therapeutic approach that provides adequate alignment preservation along with satisfactory radiological and functional results. To reduce problems and enhance fracture healing, careful intraoperative reduction and rotational control are essential. Torsional malalignment and persistent post-operative discomfort may be early signs of non-union and call for careful monitoring. These complicated injuries can still be effectively managed with modern intramedullary nailing procedures.
For segmental tibia fractures, intramedullary nailing is the recommended course of therapy; nevertheless, to avoid non-union and maximise results, careful intraoperative torsion control and attentive postoperative pain monitoring are crucial.
References
- 1. McMahon SE, Little ZE, Smith TO, Trompeter A, Hing CB. The management of segmental tibial shaft fractures: A systematic review. Injury 2016;47:568-73. [Google Scholar] [PubMed]
- 2. Alderlieste DS, Cain ME, Van Der Gaast N, Verbakel J, Edwards B, Jaarsma EH, et al. Prevalence of rotational malalignment after infrapatellar versus suprapatellar intramedullary nailing of tibial shaft fractures. JBJS Open Access 2024;9:e23.00134. [Google Scholar] [PubMed]
- 3. Nork SE, Schwartz AK, Agel J, Holt SK, Schrick JL, Winquist RA. Intramedullary nailing of distal metaphyseal tibial fractures. J Bone Joint Surg 2005;87:1213-21. [Google Scholar] [PubMed]
- 4. Sarmiento A, Latta LL. Functional fracture bracing. J Am Acad Orthop Surg 1999;7:66-75. [Google Scholar] [PubMed]
- 5. Sarmiento A, Latta LL. 450 Closed fractures of the distal third of the tibia treated with a functional brace. Clin Orthop Relat Res 2004;428:261-71. [Google Scholar] [PubMed]
- 6. Sarmiento A, Gersten LM, Sobol PA, Shankwiler JA, Vangsness CT. Tibial shaft fractures treated with functional braces. Experience with 780 fractures. J Bone Joint Surg Br 1989;71:602-9. [Google Scholar] [PubMed]
- 7. Digby JM, Holloway GM, Webb JK. A study of function after tibial cast bracing. Injury 1983;14:432-9. [Google Scholar] [PubMed]
- 8. Pugh KJ, Wolinsky PR, McAndrew MP, Johnson KD. Tibial pilon fractures: A comparison of treatment methods. J Trauma 1999;47:937-41. [Google Scholar] [PubMed]
- 9. Bonar SK, Marsh JL. Unilateral external fixation for severe pilon fractures. Foot Ankle 1993;14:57-64. [Google Scholar] [PubMed]
- 10. Anglen JO. Early outcome of hybrid external fixation for fracture of the distal tibia. J Orthop Trauma 1999;13:92-7. [Google Scholar] [PubMed]
- 11. Teraa M, Blokhuis TJ, Tang L, Leenen LP. Segmental tibial fractures: An infrequent but demanding injury. Clin Orthop Relat Res 2013;471:2790-6. [Google Scholar] [PubMed]
- 12. Finkemeier CG, Schmidt AH, Kyle RF, Templeman DC, Varecka TF. A prospective, randomized study of intramedullary nails inserted with and without reaming for the treatment of open and closed fractures of the tibial shaft. J Orthop Trauma 2000;14:187-93. [Google Scholar] [PubMed]
- 13. Corey RM, Park NK, Cannada LK. Segmental tibia fractures: An analysis of complication and healing rates. J Orthop Trauma 2018;32:296-300. [Google Scholar] [PubMed]
- 14. Duan X, Al-Qwbani M, Zeng Y, Zhang W, Xiang Z. Intramedullary nailing for tibial shaft fractures in adults. Cochrane Database Syst Rev 2012;2012:CD008241. [Google Scholar] [PubMed]
- 15. Pandya NK, Edmonds EW. Immediate intramedullary flexible nailing of open pediatric tibial shaft fractures. J Pediatr Orthop 2012;32:770-6. [Google Scholar] [PubMed]
- 16. Schemitsch EH, Kumar A, Heels-Ansdell D, Sprague S, Bhandari M, Guyatt G, et al. Reamed compared with unreamed nailing of tibial shaft fractures: Does the initial method of nail insertion influence outcome in patients requiring reoperations? Can J Surg 2023;66:E384-9. [Google Scholar] [PubMed]
- 17. Hao ZC, Xia Y, Xia DM, Zhang YT, Xu SG. Treatment of open tibial diaphyseal fractures by external fixation combined with limited internal fixation versus simple external fixation: A retrospective cohort study. BMC Musculoskelet Disord 2019;20:311. [Google Scholar] [PubMed]
- 18. McMahon SE, Little ZE, Smith TO, Trompeter A, Hing CB. The management of segmental tibial shaft fractures: A systematic review. Injury. 2016;47(3):568–73. doi:10.1016/j.injury.2015.11.022 PubMed PMID: 26776463. [Google Scholar] [PubMed] [CrossRef]
- 19. Ricci WM, Gallagher B, Haidukewych GJ. Intramedullary nailing of femoral shaft fractures: Current concepts. J Am Acad Orthop Surg 2009;17:296-305. [Google Scholar] [PubMed]
- 20. Kim KC, Lee JK, Hwang DS, Yang JY, Kim YM. Provisional unicortical plating with reamed intramedullary nailing in segmental tibial fractures involving the high proximal metaphysis. Orthopedics 2007;30:189-92. [Google Scholar] [PubMed]
- 21. Corey RM, Park NK, Cannada LK. Segmental Tibia Fractures: An Analysis of Complication and Healing Rates. J Orthop Trauma. 2018 Jun 1;32(6):296–300. doi:10.1097/BOT.0000000000001132 PubMed PMID: 29432320. [Google Scholar] [PubMed] [CrossRef]
- 22. Milenkovic S, Mitkovic M, Mitkovic M. External fixation of segmental tibial shaft fractures. Eur J Trauma Emerg Surg 2020;46:1123-7. [Google Scholar] [PubMed]
- 23. Hundal RS, Weick J, Hake M. Management of open segmental tibial fractures. J Orthop Trauma 2021;35:S50-1. [Google Scholar] [PubMed]
- 24. Sohn HS, Chung JY, Song HK. Analysis of complications and clinical outcomes in the treatment of segmental tibial fractures according to the method of internal fixation. Asian J Surg 2019;42:740-5. [Google Scholar] [PubMed]





Related Articles in Journal of Orthopaedic Case Reports
 August 1, 2026 Dual Fixation in Complex Long Bone Fractures: A Case Series of 30 Patients
August 1, 2026 Dual Fixation in Complex Long Bone Fractures: A Case Series of 30 Patients March 1, 2026 Management of a Missed Iatrogenic Fracture Neck of Femur in an Operated Case of Fracture Shaft Femur- Case Report
March 1, 2026 Management of a Missed Iatrogenic Fracture Neck of Femur in an Operated Case of Fracture Shaft Femur- Case Report March 1, 2026 Comparative Analysis of Suprapatellar and Infrapatellar Nailing in Tibial Fracture: A Randomized Clinical Study
March 1, 2026 Comparative Analysis of Suprapatellar and Infrapatellar Nailing in Tibial Fracture: A Randomized Clinical Study January 1, 2026 The Importance of Closed Reduction and Internal Fixation done with Intramedullary Implants in Pathological Fractures – A Case Series
January 1, 2026 The Importance of Closed Reduction and Internal Fixation done with Intramedullary Implants in Pathological Fractures – A Case Series